Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i01.002
Year: 2016, Volume: 2, Issue: 1, Pages: 5-10
Original Article
Ninu J Alappatt1, Kumar Sai Sailesh2, J K Mukkadan3
1Post-graduate Student, Department of Physiology, Little Flower Institute of Medical Sciences and Research, Angamaly, Kerala, India,
2Assistant Professor, Department of Physiology, Little Flower Institute of Medical Sciences and Research, Angamaly, Kerala, India,
3Professor & Research Director, Department of Physiology, Little Flower Medical Research Centre, Angamaly, Kerala, India
Address for correspondence: Kumar Sai Sailesh, Department of Physiology, Little Flower Institute of Medical Sciences and Research, Angamaly, Kerala, India. E-mail: [email protected]
Background and Objective: Acute coronary syndrome (ACS) is an umbrella term representing a common end result, acute myocardial ischemia: Including ST-segment elevation myocardial infarction (STEMI), non-ST-STEMI (NSTEMI), and unstable angina (UA). The present study was undertaken to observe and compare the clinical profile of ACS in male and female young adults.
Materials and Methods: The present cross-sectional study was conducted at cardiac ward and cardiac intensive care unit, Little Flower Hospital and Research Centre, Angamaly. 50 male and female participants admitted with ACS were recruited for the study after obtaining written informed consent by purposive sampling. Data were analyzed using SPSS 20.0. The statistical test used is regression analysis and Student’s t-test.
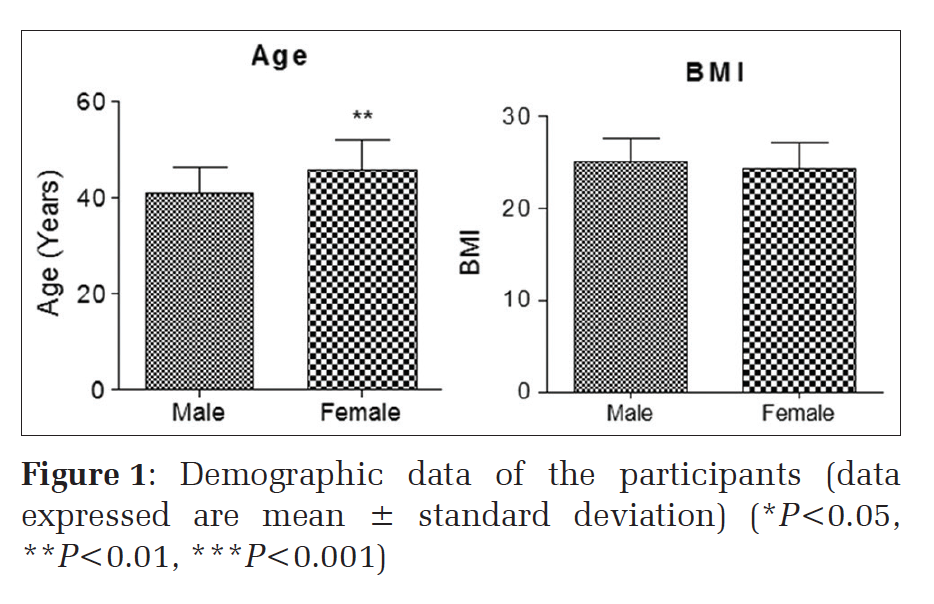
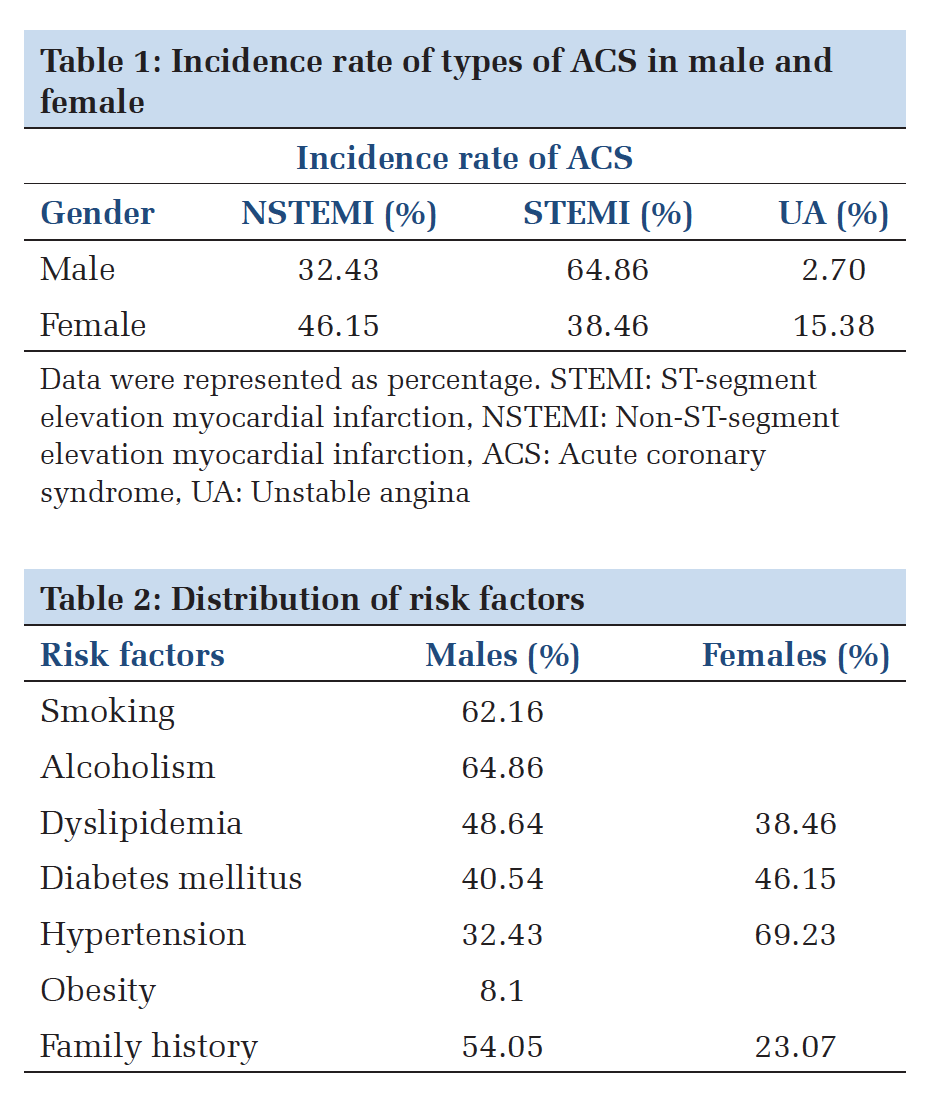
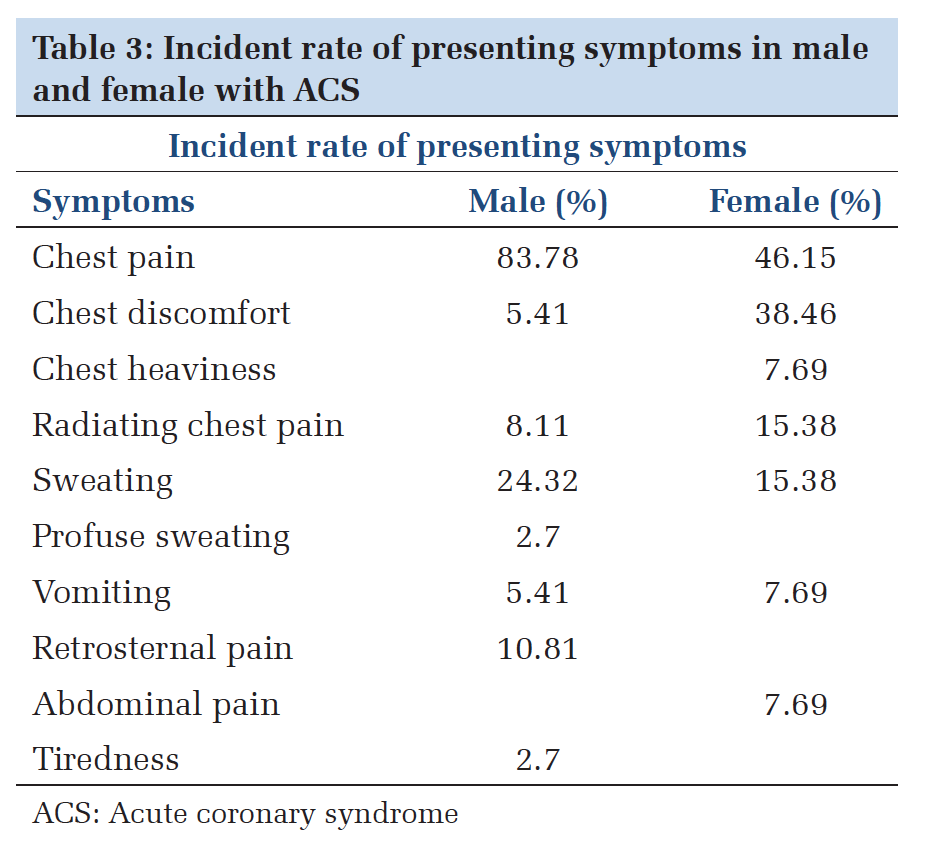
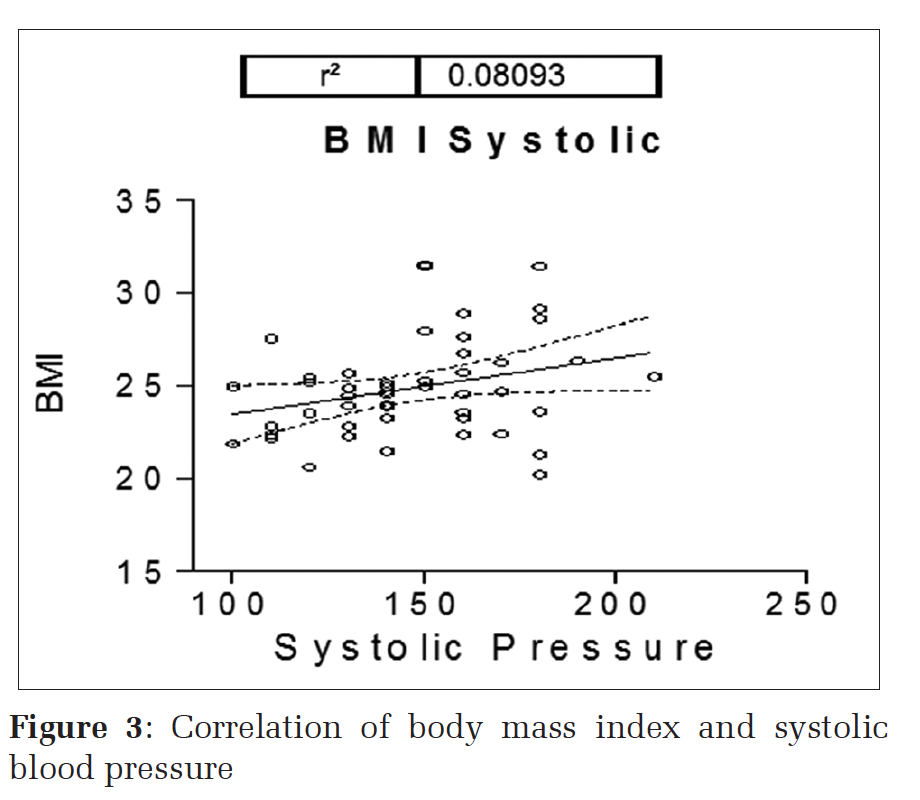
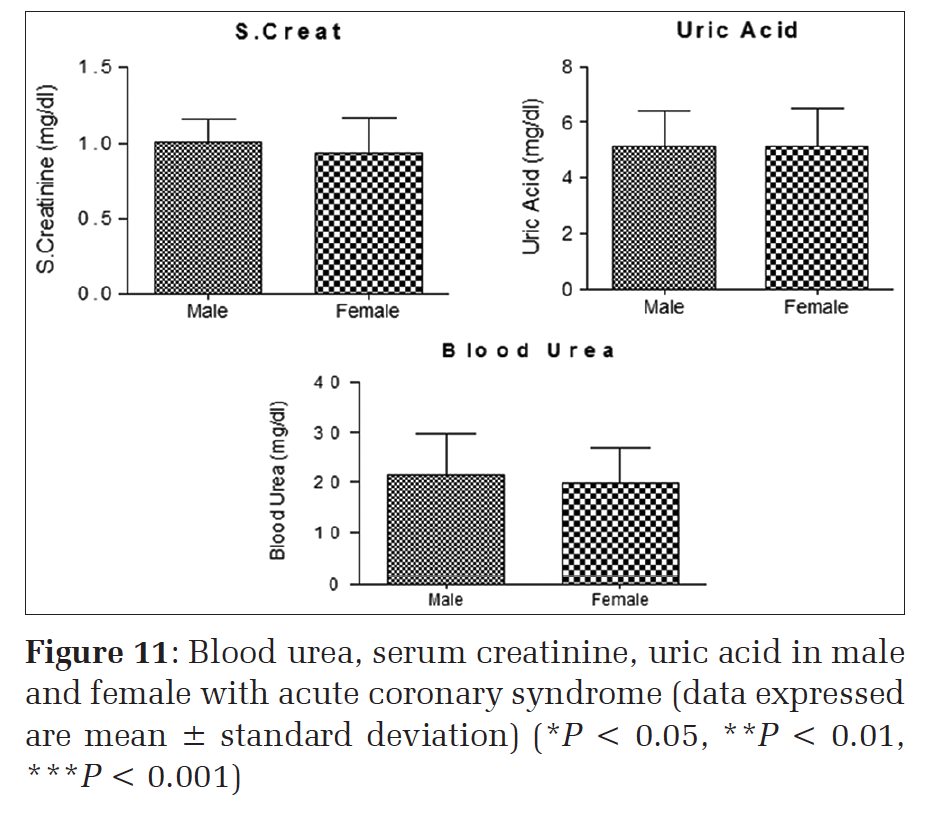
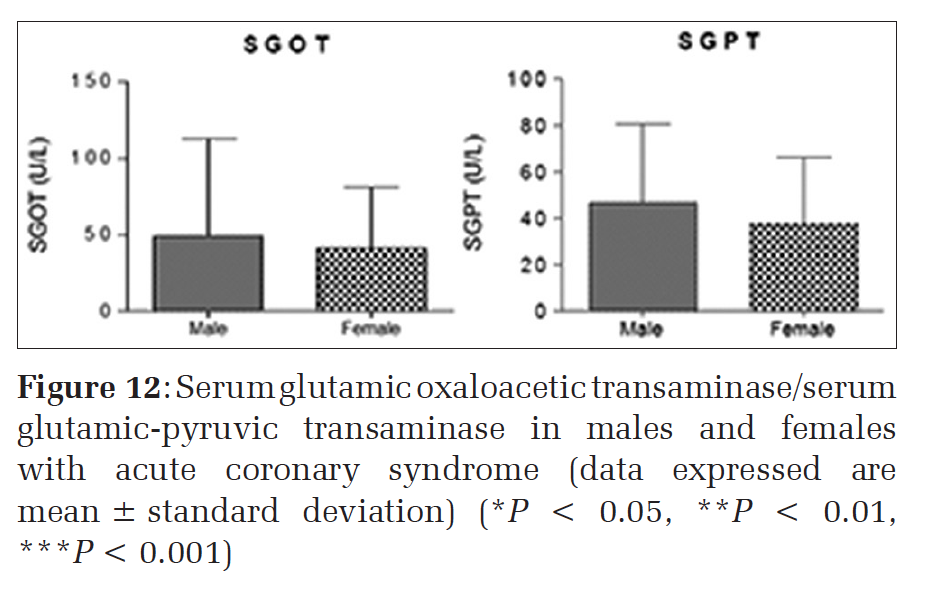
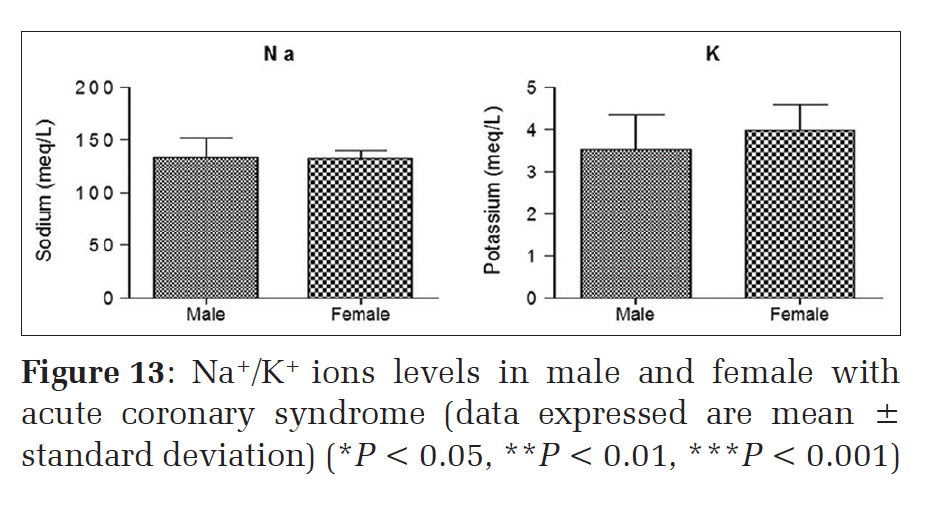
Results: Female’s age group is significantly different than males. Body mass index (BMI) is not significantly different in males and female participants. NSTEMI and UA incidence are significantly higher in females (P < 0.001). While significantly higher incidence rate of STEMI ACS was observed in males (P < 0.001). 48.65% of male patients had dyslipidemia (DLP), while only 38.46% of female patients had DLP. The incidence rate of DLP was significantly (P = 0.0067) higher in male patients. Significantly greater number of male patients presented symptoms of chest pain, while female patients presented with symptoms of chest pain or chest discomfort. The symptoms chest discomfort was significantly lower in male patients. While 7.69% of female patients presented with chest heaviness or abdominal pain, these symptoms were not observed among male patients. A symptom of sweating was prominently observed in male patients, while symptoms of retrosternal pain and tiredness were exclusive to male patients. A symptom of vomiting was equally reported by both male and female patients. Furthermore, the observation of multiple symptoms was significantly (P < 0.01) higher among male patients. As the r2 value is positive, the correlation between the parameters, although very low its positive. Female’s age group is significantly different than males. BMI is not significantly different in males and female participants. Both systolic and diastolic pressures were not significantly different in the participants. High-density lipoproteins, fasting blood sugar, low-density lipoproteins cholesterol is slightly higher in females; however, it is not statistically significant. Triglycerides and troponin I were lower in females than males. However, it is not statistically significant. Blood urea and serum creatinine were slightly lower in females than males; however, it is not statistically significant. No difference in uric acid levels was observed. Serum glutamic oxaloacetic transaminase and serum glutamic-pyruvic transaminase enzyme levels are lower in females when compared with males; however, it is not statistically significant. Sodium levels are slightly lower in females, and potassium levels are slightly higher in females when compared with males; however, it is not statistically significant.
Conclusion: The present study indicates NSTEMI and UA incidence was higher in females, and STEMI incidence was higher in males. We recommend further detailed multicenter study in this area with higher sample size to confirm the results and implement preventive measures for the benefit of the society in general.
KEY WORDS:Acute coronary syndrome, non-ST elevated myocardial infarction, ST-elevated myocardial infarction, risk factors, unstable angina.
IntroductionAcute coronary syndrome (ACS) is an umbrella term representing a common end result, acute myocardial ischemia: Including ST-segment elevation myocardial infarction (STEMI), non-ST-STEMI (NSTEMI), and unstable angina (UA).[1] In simple terms, ACS is the situation where the blood supplied to the heart muscle is suddenly blocked. Cardiovascular diseases have become one of the major health problem reaching epidemic proportions. Previous studies have reported that there is a rising incidence of ACS in the young. The currently available evidence, young patients represent 0.4-19% of all ACS cases, depending on the cut-off age used.[2-5] A significant proportion of the burden of coronary heart disease is attributed to behavioral or lifestyle factors including poor diet, obesity, and tobacco use. Biomedical risk factors such as hypercholesterolemia, hypertension, obesity, and diabetes are also known to contribute to the development of the disease. The presence of multiple risk factors in patients further accelerates the incidence of ACS and for people who already have coronary heart disease and these additional risk factors can affect their recovery and future health. Hence, it is important to identify the major risk factors and clinical profile of ACS in young adults so that future preventive measures can be taken in the form of lifestyle modification and pharmacotherapy. According to recent epidemiological studies, more than half of the worldwide cardiovascular disease burden will be borne by the Indian subcontinent in the next decade.[6] Cardiovascular risk factors for ACS are on the rise in people of Indian origin, and ACS is now the leading cause of death.[6-10] The present study was undertaken to observe and compare the clinical profile of ACS in male and female young adults. Materials and MethodsStudy designCross-sectional study. ParticipantsThe study was approved by the Institutional Ethics committee of Little Flower Hospital and Research Center, and informed consent was obtained from all the participants. 50 patients of either sex fulfilling the inclusion criteria admitted with ACS in Cardiac unit of Little Flower Hospital, Angamaly were recruited by purposive sampling. Inclusion criteria
Exclusion criteria
MethodsHistory collection, clinical examination, ECG, echocardiography, laboratory investigations such as complete blood count, lipid profile, blood sugar level, cardiac markers, urine analysis, and other routine investigations done as a part of routine diagnosis and treatment.
Data analysisData were analyzed using SPSS 20.0. The statistical test used is regression analysis and Student’s t-test.
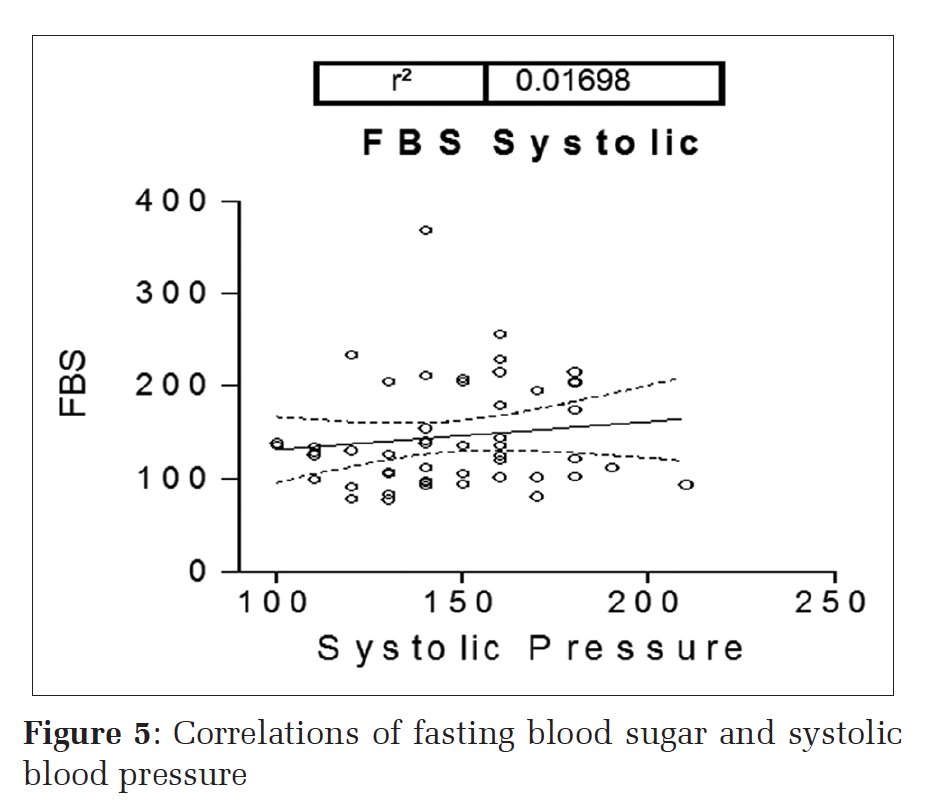
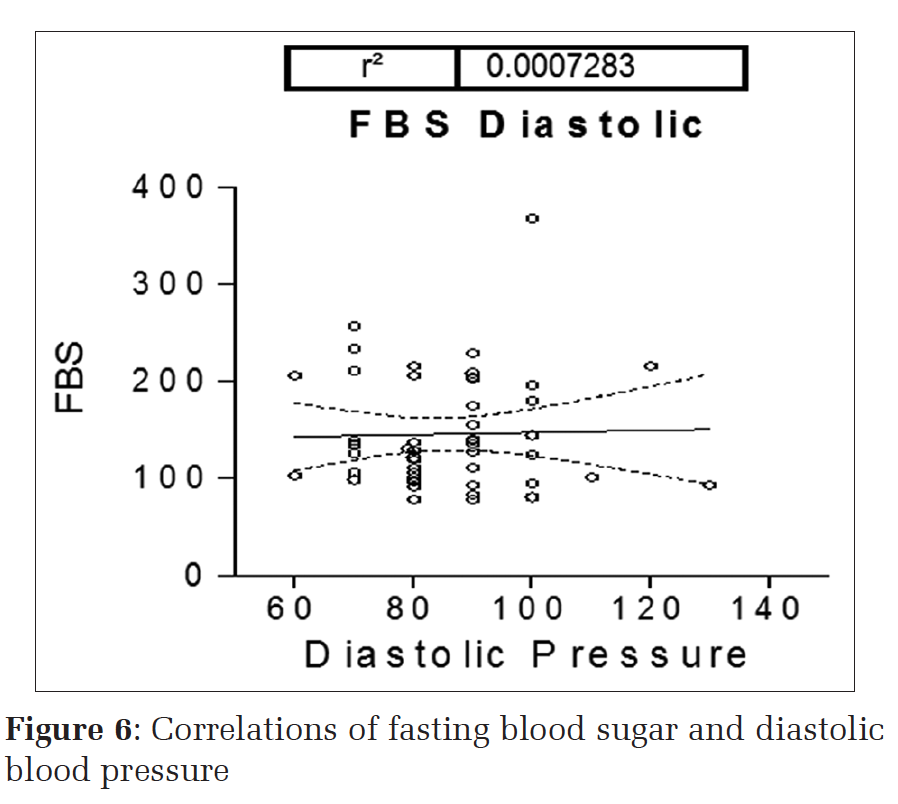
ResultsFemale’s age group is significantly different than males. Body mass index (BMI) (Figure 1) is not significantly different in males and female participants. NSTEMI incidence is significantly higher in females (P < 0.001) (Table 1). UA incidence is significantly higher in females (P < 0.001) (Table 1). While significantly higher incidence rate of STEMI ACS was observed in males (P < 0.001). 48.65% of male patients had dyslipidemia (DLP) (Table 2), while only 38.46% of female patients had DLP. The incidence rate of DLP was significantly (P = 0.0067) higher in male patients. Significantly greater number of male patients presented symptoms of chest pain/while female patients presented with symptoms of chest pain or chest discomfort (Table 3). The symptoms chest discomfort was significantly lower in male patients. While 7.69% of female patients presented with chest heaviness or abdominal pain, these symptoms were not observed among male patients (Table 3). A symptom of sweating was prominently observed in male patients, while symptoms of retrosternal pain and tiredness were exclusive to male patients. A symptom of vomiting was equally reported by both male and female patients. Furthermore, the observation of multiple symptoms was significantly (P < 0.01) higher among male patients. The weak positive correlation was observed between age and BMI; BMI and systolic blood pressure (SBP); BMI and diastolic blood pressure (DBP); fasting blood sugar (FBS) and SBP; FBS and DBP; FBS and
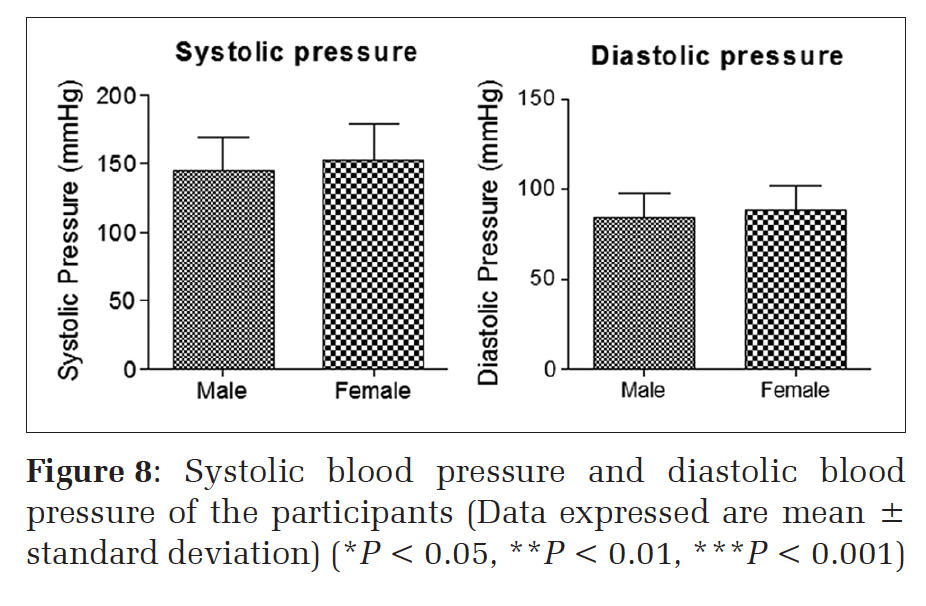
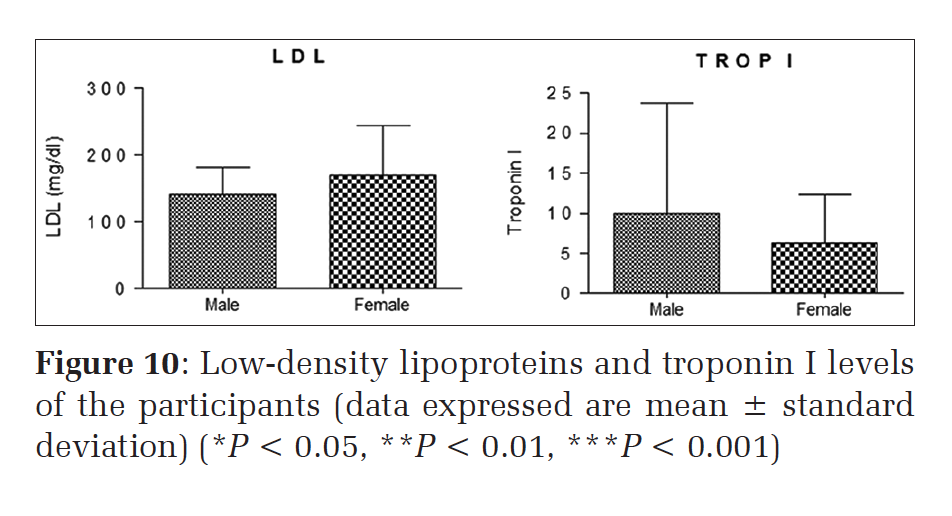
triglycerides (Figures 2-7). Female’s age group is significantly different than males (Figure 1). BMI is not significantly different in males and female participants (Figure 1). Both systolic and diastolic pressures were not significantly different in the participants (Figure 8) high-density lipoproteins, FBS, low-density lipoproteins cholesterol are slightly higher in females; however, it is not statistically significant. Triglycerides and Troponin I were lower in females than males. However, it is not statistically significant (Figures 9 and 10). Blood urea and serum creatinine were slightly lower in females than males; however, it is not statistically significant. No difference in uric acid levels was observed (Figure 11). Serum glutamic oxaloacetic transaminase (SGOT) and serum glutamic-pyruvic transaminase enzyme levels are lower in females when compared with males; however, it is not statistically significant (Figure 12). Sodium levels are slightly lower in females, and potassium levels are slightly higher in females when compared with males; however, it is not statistically significant (Figure 13).
|
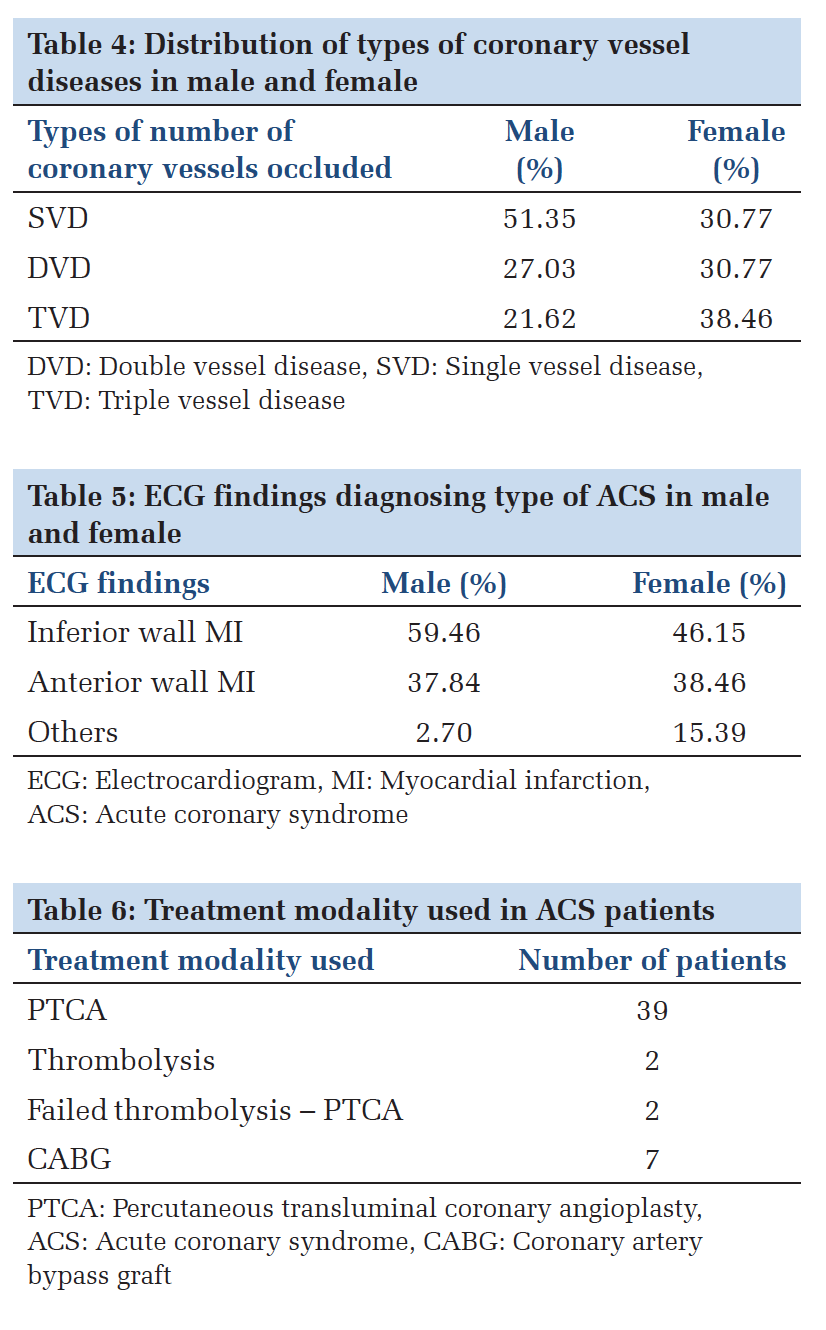
DiscussionIt was reported that[11] the gender wise distribution of male and female shows 72% males and 28% females, 79% males, and 21% females, respectively. Earlier studies reported that that ACS in young is a disease of men. In the present study, it was observed that 74% male and 26% females are noticed with ACS. The mean age of patients in earlier studies was 37.03 and 32 years.[12,13] In the present study, the mean age of the patients was 42.06 years. Most of the patients were in the age group between 25 and 54 years. About 25% of ACS in India occurs under the age group of 40 years and 50% under the age group of 50 years. In this study, the chest pain was the most common presenting symptom found in patients with ACS, which is followed by sweating in most cases. A similar finding was reported in earlier studies.[12] In the study, smoking was the most common risk factor presenting in males (64.86%), whereas it remains 0% in females. It was reported that[13] smoking is 76.9% and 75%, respectively. Many studies have shown that smoking is a major risk factor for MI. Hypertension was present in 69.23% of the female cases in the study, whereas male cases show 32.43% only. This shows females are at a high risk of getting hypertension which is a major risk factor of ACS. Wander et al.[14] observed hypertension in 47% of the patients. The family history of coronary artery disease was present in 54.05% male patients and 23.07% female patients in the present study. Studies made by Bharani et al.[15] noted the family history of coronary artery disease in 40% and 38%, respectively, in the patients. The present study shows DLP in 48.64% males and 38.46% females. It was reported that 42% of patients had hypercholesterolemia. Diabetes mellitus was noticed in 40.54% in males and 46.15% in females.[15] Earlier studies reported that diabetes in 22% of their patients including male and female.[16] Obesity is an independent coronary risk factor. In the study, it has been observed that 38% were having BMI above 25%, and 6% were obese having BMI above 30. Similar observations were made by Kaur et al. who reported obesity in 7% and 11%, respectively. In this study anterior wall, MI was the most frequent location of MI on the ECG. This study notices 56% of anterior wall MI in patients with ACS. 38% of inferior wall MI in patients and 6% of patients with no ECG changes with the ACS (Tables 4-6). Earlier studies reported that 60.3% anterior wall MI and 39.6% inferior wall MI, 68% anterior wall MI and 29% inferior wall MI, respectively.[17]
LimitationsThe sample size was small in the present study, and the study was conducted at a single center.
ConclusionThe present study indicates NSTEMI and UA incidence was higher in females and STEMI incidence was higher in males. We recommend further detailed multicenter study in this area with higher sample size to confirm the results and implement preventive measures for the benefit of the society in general. |
Subscribe now for latest articles and news.