Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.424
Year: 2026, Volume: 12, Issue: 2, Pages: 155-158
Original Article
Ranjan Agrawal 1, Sagar Rawat 2, Vindhya Prabhakar 2, Shashwat Verma 3
1Professor & Head, Department of Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India.
2Postgraduate student, Department of Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India.
3Assistant Professor, Department of Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India.
Address for correspondence: Ranjan Agrawal, Professor & Head, Department of Pathology, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, India.
E-mail: [email protected]
Received Date:27 December 2025, Accepted Date:25 April 2026, Published Date:18 May 2026
Background: Granulomatous lesions of skin pose a diagnostic challenge to pathologists due to their diverse clinical and histopathological presentations. Both infective and non- infective etiologies can result in cutaneous granuloma formation. Histopathological examination is mandatory in confirming the clinical diagnosis and to classify granulomatous skin lesions accurately.
Aim: To analyse the spectrum of different granulomatous lesions of skin diseases in patients presenting to the Dermatology department of a tertiary care teaching hospital.
Materials and Methods: This cross-sectional observational study was conducted in the Pathology Department, Rajshree Medical Research Institute, Bareilly, Uttar Pradesh, over a period of one year (November 2024 to October 2025). Punch biopsy specimens were obtained, fixed, grossed, processed using standard protocols, and stained with routine H&E stain. All sections were examined microscopically, and cases showing granulomatous pathology were included. Special stains were applied as and when indicated.
Statistical Analysis: Data were compiled in Microsoft Excel sheet and later analyzed using SPSS version 25.0.
Results: A total of 80 cases were included, the majority belonging to the 21–40-year age group, with a slight male preponderance. Infectious etiologies were the most common type of granulomas, with leprosy being the predominant diagnosis.
Conclusion: Leprosy remains the most common cause of cutaneous granulomatous pathology in the present study. Skin biopsy from representative area plays an important role in the evaluation of granulomatous pathology. Histopathological examination, supplemented by special stains, remains the gold standard for arriving at a definitive diagnosis and accurate treatment.
Granulomatous skin lesions constitute a wide spectrum of diseases seen in the dermatology clinics and pose a great diagnostic dilemma for both the treating dermatologists as well as the diagnosing histopatho- logists. Cutaneous granulomas represent a mixed blend of disorders characterized by an inflammatory reaction in the skin, stimulated by a wide variety of factors including infections, foreign bodies, malignancies, metabolites, or certain chemicals[1].
The distribution of granuloma varies widely with the geographical location and depends on several factors, including the climatic variations, socio-economic status, cultural variations, educational status, and availability of
A cross-sectional prospective study was carried out in the Department of Pathology of a medical institute over a period of one year. The clinical findings and relevant information was recorded from patients using proper patient requisition forms.
Punch biopsies, including a small portion of adjacent normal skin were obtained and fixed in 10% neutral buffered formalin, grossed, processed by standard techniques, and stained with H&E stain. All the biopsies were examined microscopically, and those showing granulomatous pathology were included in this study.
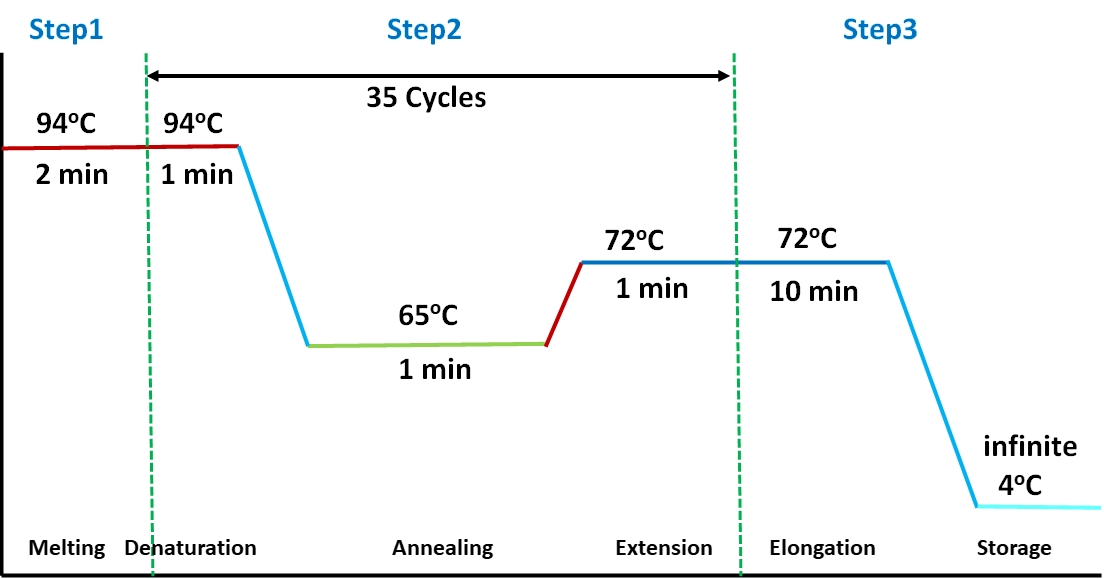
Special stains such as modified Ziehl–Neelsen (ZN) and Fite–Faraco (FF) stains were used wherever required to demonstrate acid-fast bacilli. The cases were analyzed and categorised according to the clinical and histopathological observations.
A total of 80 cases were included in the present study. Microscopic findings were observed, correlated, and the
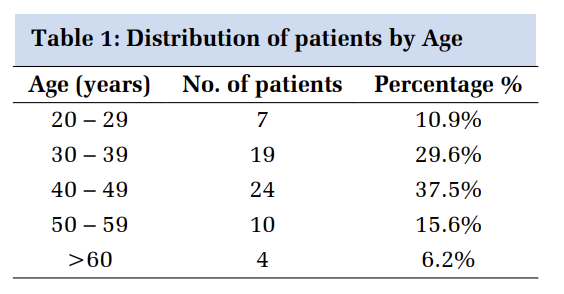
results were tabulated. The age distribution of the cases is shown in [Fig. 1]. Maximum cases were in the 21–40-year age group, followed by 41–60 years age group.

A slight male predominance was observed, with a male-to-female ratio of 1.16:1 [Table. 1]. In this study, males were affected more by infectious pathologies such as leprosy, whereas females were more affected by non-infectious conditions like granuloma annulare and fungal infections.
| Age | Male | Female | Total | Percentage % |
|---|---|---|---|---|
| 0-20 | 8 | 6 | 14 | 17.5 |
| 21-40 | 17 | 14 | 31 | 38.7 |
| 41-60 | 12 | 9 | 21 | 26.3 |
| 61-80 | 5 | 7 | 12 | 15.0 |
| >80 | 1 | 1 | 2 | 2.5 |
| Total | 43 | 37 | 80 | 100 |
| Diagnosis | Number (n) | Percentage (%) |
|---|---|---|
| Leprosy | 61.3 | |
| Indeterminate | 11 | |
| Tuberculoid | 5 | |
| BT | 6 | |
| BB | 6 | |
| BL | 4 | |
| Lepromatous | 16 | |
| Histioid | 1 | |
| Tuberculosis | 20 | |
| Lupus vulgaris | 9 | |
| Scrofuloderma | 3 | |
| TVC | 4 | |
| Fungal infection | 7.5 | |
| Actinomycosis | 4 | |
| Maduromycosis | 2 | |
| Cutaneous Leismaniasis | 1 | 1.2 |
| Sarcoidosis | 1 | 1.2 |
| Granuloma annulare | 3 | 3.8 |
| Foreign body granuloma | 5 | |
| Epidermal Cyst | 2 | |
| Xanthoma | 1 | |
| Rhinosporidiosis | 1 | |
| Total | 80 | 100 |
Histopathological diagnoses were classified into three broad categories: infectious, non-infectious, and miscellaneous [Table. 2]. Infectious pathology accounted for 72 cases (90%). The non-infectious category included 4 cases (5%), comprising three cases of granuloma annulare and one of sarcoidosis. Four cases (4.35%) were grouped under miscellaneous causes. The clinical presentations of some of the patients have been depicted in [Fig. 1].
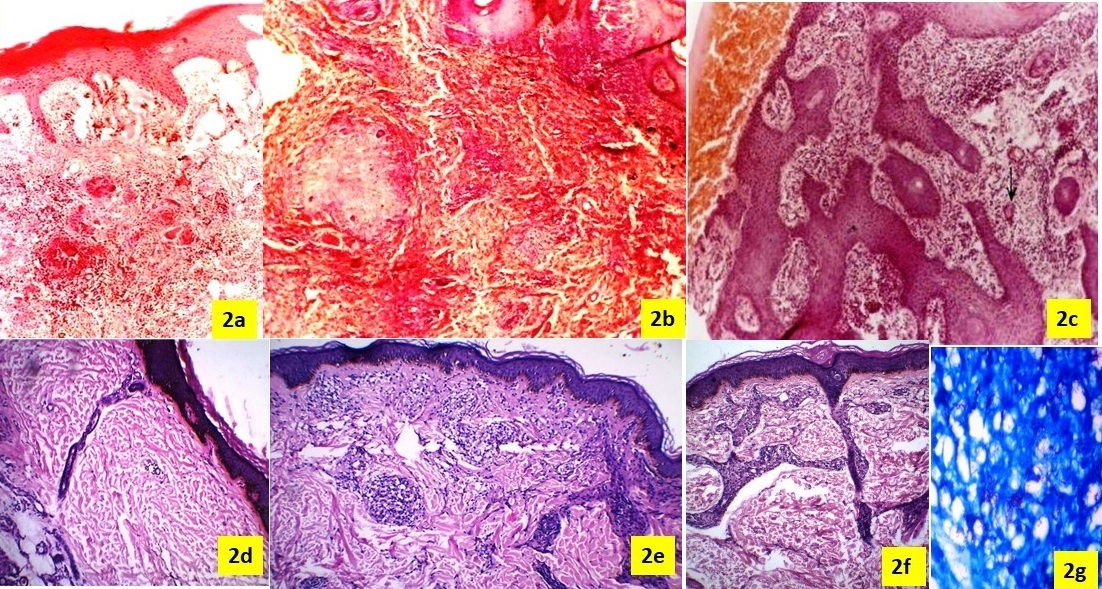
Leprosy was the predominant infectious type of granulomatous pathology (49/80 cases), with indeterminate leprosy subtype as the most common (16 cases; 32.7%). Leprosy was most commonly noted in the 21–40-year age group. Clinico-histopathological concordance was observed in 34 cases (42.5%). The photomicrograph showing the microscopic features in different granulomatous lesions is depicted in [Fig. 2].
Cutaneous granulomatous comprise a variety of disorders sharing the common histopathological observation of granuloma formation[4]. Nearly similar histological patterns may be observed due to diseases of different etiologies, even though a single etiology may produce variable histological picture[5]. Incidence and prevalence of different granulomatous dermatitis depends on the geographic location. Many skin granulomatous lesions show similar histomorphological findings and even a single disease can show variable histological features. Granulomatous inflammation is a type-IV hypersensitivity reaction to an antigen.
In the present study, most of the patients were in the 21–40-year age group (38.8%), followed by 41–60 years (26.3%). Similar findings were reported by previous authors, who observed the highest incidence in the 21–40-year age group[4, 6, 7]. Comparable results were also noted by Permi et al. and Potekar et al.[7, 8]. In contrast, Queirós et al reported 51–60 years as the most frequently affected age group[9].
Male predominance was noted in the present study (71.01%), consistent with the findings by some other authors[3, 4, 8, 10]. However, Zafar et al. and Kumbar et al. reported a female predominance[11, 12]. These differences could be attributed to the geographical distribution or the type of the set up.
Infectious causes constituted the most common aetiology of skin granulomas (90.0%), followed by equal proportion of non-infectious causes and miscellaneous lesions (5.0%) each. These findings are in concordance with the previous studies which also reported infectious etiology as the most common category[4, 10, 13, 14]. In contrast, Queirós et al found non-infectious lesions to be more common, probably due to their geographical and socioeconomic differences[9].
Leprosy (Hansen’s disease) comprised of the commonest infectious aetiology of cutaneous granuloma in our study, with indeterminate leprosy being the most frequent subtype. These findings are consistent with the earlier published reports[4, 15]. However, Ahmed et al. and Potekar et al. reported borderline tuberculoid leprosy as the most common variety[8, 14]. This difference could be due to difficulty in reporting of the Indeterminate subtype.
Cutaneous tuberculosis was the second most common infectious etiology, with lupus vulgaris being the predominant subtype. Clinico-histopathological concordance was observed in 63.4% of cases, which is comparable to the other studies that reported a concordance rate that ranged from 61% to 92%[3, 4, 7, 13, 16]. Lupus vulgaris was the most common subtype as reported previously by other authors as well[1, 5, 17, 18].
Special stains play a pivotal role in the diagnosis of cutaneous granulomas. Acid-fast bacilli were demonstrated in 34 cases using modified ZN stain and in 10 cases using Fite–Faraco stain. Similar observations have been reported in the earlier published reports[6, 16, 18].
Infections remain the most important cause of cutaneous granulomatous diseases, with leprosy as the commonest etiology. Despite great efforts and vigorous newly launched national health programs aimed at eradicating leprosy, it continues to pose as a major public health threat.
Histopathology has a major role in the classification and subtyping of cutaneous granulomas. A through and careful histopathology of skin biopsy, supported by relevant clinical details helps in arriving at a confirmatory diagnosis.
Judicious use of special stains is important, particularly in diagnosing overlapping or problematic cases. Such studies help in the diagnostic accuracy, guide effective treatment, and in reducing the disease burden besides supporting the regional healthcare programs.
1. Clinically suspected granulomatous skin lesions on the face: A prospective clinico-pathological correlation study of 77 cases. Indian Journal of Dermatology, Venereology and Leprology. 2025; 92 Available from: https://doi.org/10.25259/ijdvl_1167_2025
2. Histomorphological analysis and clinical correlation of neoplastic and non neoplastic skin lesions: a study in a tertiary care centre of Western Uttar Pradesh, India. International Journal of Research in Medical Sciences. 2020; 8 (8). Available from: https://doi.org/10.18203/2320-6012.ijrms20203093
3. Histopathological study of cutaneous granulomas. Journal of Pathology of Nepal. 2019; 9 (2). Available from: https://doi.org/10.3126/jpn.v9i2.25388
4. The histopathological approach to granulomatous skin lesions. IP Journal of Diagnostic Pathology and Oncology. 2020; 5 (1). Available from: https://doi.org/10.18231/j.jdpo.2020.012
5. Chakrabarti S, Pal S, Biswas BK, Bose K, Pal S, Pathak S. Clinico-Pathological Study of Cutaneous Granulomatous Lesions- a 5 yr Experience in a Tertiary Care Hospital in India. Iranian Journal of Pathology. 2016; 11(1):54-60
6. Histopathological study of dermal granuloma. Indian Journal of Medical Sciences. 2019; 71 (1). Available from: https://doi.org/10.25259/ijms_11_2019
7. A Histopathological Study of Granulomatous Inflammation. Journal of Health and Allied Sciences NU. 2012; 02 (01). Available from: https://doi.org/10.1055/s-0040-1703548
8. Histopathological Study of Infectious Granulomatous Skin Lesions. Annals of Pathology and Laboratory Medicine. 2018; 5 (7). Available from: https://doi.org/10.21276/apalm.1874
9. Granulomatous Skin Diseases in a Tertiary Care Portuguese Hospital: A 10-Year Retrospective Study. The American Journal of Dermatopathology. 2020; 42 (3). Available from: https://doi.org/10.1097/dad.0000000000001441
10. Infectious granulomatous dermatitis: A clinico pathological study. Indian Journal of Dermatology. 2006; 51 (3). Available from: https://doi.org/10.4103/0019-5154.27993
11. Zafar MNU, Sadiq S, Memon MA. Morphological study of different granulomatous lesions of the skin. Journal of Pakistan Association of Dermatologists. 2018;18:21–8.
12. Infectious Granulomatous Dermatitis at a Tertiary Care Centre in North Maharashtra: A Histopathological Study. Journal of Clinical and Diagnostic Research. 2016; 10 (11). Available from: https://doi.org/10.7860/jcdr/2016/15436.8891
13. Granulomatous lesions of the skin. Journal of Pathology of Nepal. 2011; 1 (2). Available from: https://doi.org/10.3126/jpn.v1i2.5397
14. Histopathological study of cutaneous granulomatous lesions. Indian Journal of Pathology and Oncology. 2019; 6 (4). Available from: https://doi.org/10.18231/j.ijpo.2019.102
15. Sharma S, Rai NN. Demographic profile and clinicopathologic concordance of leprosy in North-West Rajasthan, India: a 2-year prospective study. International Journal of Clinicopathological Correlation. 2018;2:1–5.
16. Makwana VR. Granuloma revisited: a prospective study of granulomatous skin lesions at a tertiary care centre in Gujarat. International Journal of Recent Scientific Research. 2018;9(8):28607–13.
17. A clinical and histopathological profile of patients with cutaneous tuberculosis. Indian Journal of Dermatology. 2011; 56 (5). Available from: https://doi.org/10.4103/0019-5154.87153
18. Pattern of granulomatous skin lesions in a tertiary care centre of western Uttar Pradesh. Indian Journal of Pathology and Oncology. 2021; 8 (1). Available from: https://doi.org/10.18231/j.ijpo.2021.005
Subscribe now for latest articles and news.