Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.014
Year: 2021, Volume: 7, Issue: 3, Pages: 72-78
Original Article
Rinki Kumari1 , Divya Verma2 , Neetu Gautam3 , Ajay Kumar Sahi4 , Akansha2 , Sisodia Sunil Kumar Rai5 , G P Dubey6
1Department of Microbiology, Hind Institute of Medical Sciences, Mau Ataria, Sitapur Rd, Uttar Pradesh, India261303,
2Department of Paediatric, Hind Institute of Medical Sciences, Mau Ataria, Sitapur Rd, Uttar Pradesh, India-261303, 3Department of Paediatric, Government Medical College, Badaun, Uttar Pradesh, India- 243601 ,
4School of Biomedical Engineering, Indian Institute of Technology (Banaras Hindu University), Varanasi, 221005, Uttar Pradesh, India,
5Department of Cell and Molecular Biology, Medical University of the Americas, Nevis, Saint Kitts and Nevis, West Indies KN 1101,
6Department of Advanced Centre for Traditional and Genomic Medicine, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India- 221005
Address for correspondence:
Rinki Kumari, Department of Microbiology, Hind Institute of Medical Sciences, Mau Ataria, Sitapur Rd, Uttar Pradesh, India261303. E-mail: [email protected]
Purpose: The primary goal of this research study was to determine the plasma levels of folate, vitamin B, and homocysteine in malnourished children in Uttar Pradesh-India, and also to evaluate the 5, 10-methylenetetrahydrofolate reductase (MTHFR) 677C>T mutation in the MTHFR gene as nutrigenetic factors in the children with malnutrition. Methods: 345 samples were collected to assess the fasting plasma levels of folate, vitamin B, and homocysteine using an ELISA. A polymerase chain reaction (PCR) with specific primers was used to analyze the MTHFR 677C>T polymorphism, followed by amplicon digestion with the Hinf I restriction enzyme (C677T genotypes were determined by PCR–RFLP). Results: Compared to controls, the malnourished group had higher plasma homocysteine levels and lowered folate and vitamin B12 levels (P<0.001). The CC genotype was present in 26 out of the 167 malnourished children, followed by CT in 52 and TT in 89. CC, CT, and TT genotype frequencies were 15.56%, 31.13%, and 53.29% respectively. In the malnourished group, the frequency of C allele was 0.31, and T allele was 0.68. Genotype frequencies in the control group: CC was observed in 162 (91.01%), CT in 14 (7.86%), and TT in 2 (1.12 %). In control, the C allele was found to have a frequency of 0.94, while the T allele had a frequency of 0.05. Conclusion: In short, the percentage of homozygous genotype (TT) is highest in malnourished children associated with a high level of homocysteine which shown the deficiency of folate and vitamin –B. However, childhood malnutrition may be caused by gene-environment interactions as well as nutrient deficiencies. Nutrient absorption and metabolism may be affected by genetic polymorphisms in host genes. Therefore, it is important to investigate the genetic predisposition to malnutrition, identify genetic markers and biomarkers that can aid in the identification of children at risk of malnutrition, and investigate new treatment modalities that can help in the clinical management and treatment of malnourished children.
Nutrigenomics and nutrigenetics explore the interaction between nutrients & genes through the specific mode of action.[1,2] This mode of action is involved in determining the risk of developing numerous diseases. Nutrigenomics also describes the effect of all forms of nutrients on gene expression, including food-based, dietary restriction, and supplementary nutritional agents.
This study will focus on the impact of nutrients around the genome on the transcriptome, proteome, and metabolome in cells, tissues, and species. Furthermore, it can identify and validate genes that affect[3–5] the risk of diet-related diseases.[1–3] Therefore, nutrients are essential for cellular function and the balance of the internal environment tissues in the entire body, but their deficiency is linked to malnutrition.[3]
Malnutrition has been related to an increased susceptibility to diseases or infection and a negative impact on children’s behavior and cognitive performance.[1,4,5] It is in school-aged children described as a public-child health problem in the developing world.[5,6] Environmental, lifestyle, and genetic factors have all been established as significant contributors to the development of malnutrition; it has inheritability traits.[6–8]
As a result, healthy living, including good dietary habits, can help to prevent malnutrition through epigenetic mechanisms.[1] According to current clinical research, malnutrition and various diseases such as mental retardation, depression, stroke, Parkinson’s, Alzheimer’s, and dementia, including neural tube defect, have linked gene-environment interactions also through oxidative stress pathways.[8–12] Homocysteine, Vitamin B, folate, and methylenetetrahydrofolate reductase (MTHFR) are linked together and play various biological ways.[6,8]
Folic acid and vitamin B-12 metabolism are interconnected, and both vitamins, together with the flavoprotein methylenetetrahydrofolate reductase (MTHFR), are needed for methionine synthesis from homocysteine.[10,11] MTHFR is a critical enzyme in folate-dependent metabolism. It is involved in catalyzes the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate in the presence of methionine synthase and cofactors-Vit-B12, which is used to synthesize methionine from homocysteine (Hcy). Methionine is the precursor of S-adenosylmethionine (the methyl group donor), which is used for DNA synthesis and DNA methylation (essential for gene expression in the body), cell division, and tissue growth and development.[9]
Deficiency of the MTHFR enzyme increased the rise of homocysteine levels and, known as hyperhomocysteinemia, can disrupt the one-carbon metabolism pathway, resulting in malnutrition.[10–12] This deficiency is passed down through the generations as an autosomal recessive trait. Hyperhomocysteinemia has been attributed to several disorders, including heart disease, Alzheimer’s disease, and cognitive dysfunction. As a result, it’s essential to look into the genes, diet, and other factors that play a role in malnutrition, mainly when a deficient diet is associated with excessive consumption of calories and lack of physical activity, occupational, and unhealthy activities.[13–16] Hyperhomocysteinemia and low folate levels in plasma and red blood cells are more common in people who have TT genotype.[17–21]
Only a little information is available on MTHFR C677T mutation frequency in Indian malnourished children. Therefore, the purpose of the current study had two targets: first, to determine plasma levels of homocysteine, vitamin B12, and folate, which have been linked to malnutrition, and second, to investigated the associations between MTHFR C677T and malnourished children.
The Institutional Ethics Committee of Banaras Hindu University’s Institute of Medical Sciences, Varanasi, approved this study (vide Ref. no. Dean/2012-13/376, dated 17-12-2012). Children of various age groups were selected from different regions of Sonbhadra, Chandowali, and Varanasi, and their parents were contacted through their children’s respective school teachers. Informed consent was obtained from the parents before they participated in the study and 2012-2016.
A total of three hundred forty-five children aged five to twelve years old were enrolled and initially screened for malnutrition using the body mass index (BMI) [weight(kg)/height2 (m2 )] according to WHO guidelines, which describe normal values for five to twelve-year-olds as 15.26 to 17.53 for boys and 15.24 to 18.00 for girls. The standard deviation of the malnourished children’s BMI values was twice as low as the standard deviation of the reference values. Following the screening protocols, the sample included 167 malnourished children, and 178 healthy children with good nutritional status were also included in the study as controls.
4 ml venous blood samples were collected on Ethylene diamine tetra acetic acid (EDTA) coated vials from all enrolled subjects and preserved at 4 ◦C until assayed. 2 ml blood was stored for total genomic DNA extraction, and Miller et al. protocol was employed to extract the DNA as described previously.[22] The rest of the blood was centrifuged at 4◦C for 20 minutes at 2000 rpm. Plasma was collected after centrifugation and dispensed into 1.5 mL Eppendorf tubes held at –80◦C until the assay. The levels of folic acid, vitamin B12, and total homocysteine in the blood were measured using commercially available ELISA kits (Enzyme-linked immunosorbent assay) (ENZO Life sciences).
1. Polymerase Chain Reaction (PCR) Amplification: A 25-ul reaction mixture containing approximately 100 ng genomic DNA, 200 uM dNTPs, 50 picomoles of forward and reverse primers, and 2 units of Taq DNA polymerase (Quia gene, Frankfurt, Germany) in a 1X buffer containing 1.5 mM MgCl2 supplied with the enzyme was used for PCR amplification. PCR was performed in a Mini thermocycler (Bio-Rad, USA). 2. According to Frosst et al.[19] primer sequences for the polymorphic site or mutation analysis (CT) at 677 bp were derived from intron sequence bracketing exon (4).
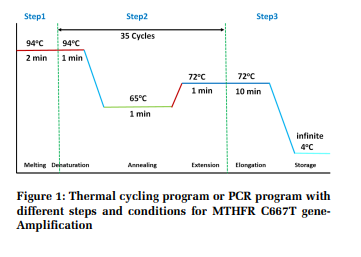
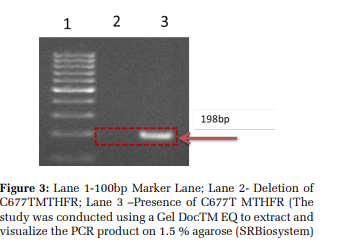
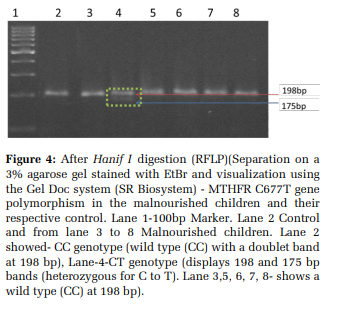
Figure 1 was showing -An initial 2-minute melting stage at 94◦C was followed by 35 cycles of 1-minute denaturation at 94◦C, 1-minute annealing at 65◦C, 1-minute extension at 72◦C, and a final 10-minute elongation step at 72◦C and 198bp PCR products have been separated 1.5% agarose (polysaccharideFermentas). For RFLP analysis, the Hinf I restriction enzyme (Genei, India) was used to digesting the amplified product, which cleaves only the mutant MTHFR allele into 175- and 23-bp fragments. Electrophoresis in 3 percent agarose (Fermentas) gels was used to examine the amplification and restriction materials.
The statistical analyses were conducted using the automated Statistical Package for Social Sciences version 16. All data were analyzed using the mean and standard deviation (SEM). The Hardy-Weinberg equilibrium equation was used to evaluate genotype and allele frequencies in malnourished children and controls. The chi scale (X2 – test) was used to assess the classes in the statistical study. The risk factor for malnutrition was calculated using the odds ratio with a 95 percent trust interval between malnourished children and their respective monitors.
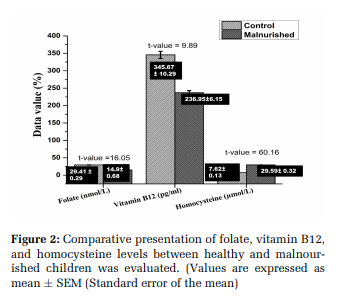
345 children of both genders (male & female) were studied for malnutrition, out of which 167 children were malnourished with an average age group of 8.65 ± 0.23 years, and 178 healthy children of average age 8.78 ± 0.29 years were considered as control. Results have linked folate and vitamin B12 deficiency to cognitive impairment in malnourished infants[1,6,13,14] ; as per our study, their plasma levels of folate and Vit-B12 were found to be significantly lower in malnourished children and the results obtained (figure-2; P <0.05) were found almost similar to the previously reported results. Hyperhomocysteinemia, a condition linked to various cardiovascular and neurological disorders, may also be caused by a lack of folate and Vit-B12.[1,6,13,14] The findings showed significantly higher homocysteine levels when comparing the malnourished children to the control group (>4 fold).
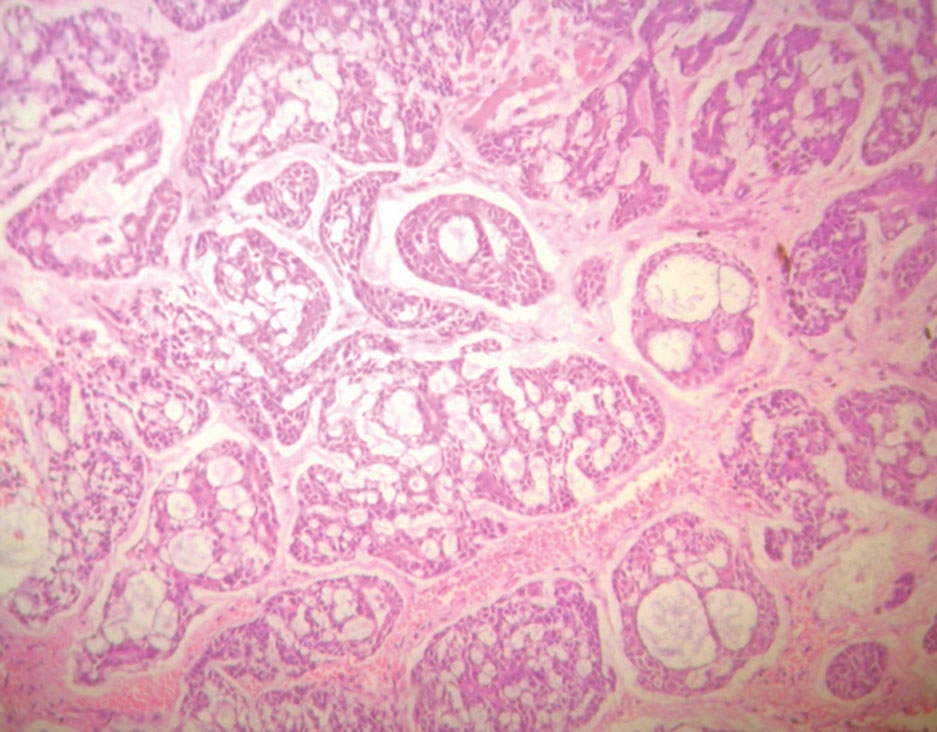
Figure 3 shows a 198-bp amplicon generated by MTHFR C677T specific primers after amplification. Wild homozygous (CC) genotype - developed 198- bp band, homozygous mutant genotype produced two bands (175 bp and 23 bp), and heterozygous (CT) genotype generated three bands in agarose gel electrophoresis (198 bp, 175 bp, and 23 bp). The MTHFR 677C/T genotype CC frequency was significantly higher among control than test subjects (91.01% and 6.58%, respectively) (Figure 4). The frequencies of MTHFR 677C/T heterozygous and homozygous genotypes (CT and TT) were higher among subjects (31.13% and 53.29%, respectively) than control (7.86% and 1.12%, respectively) with an odds ratios of 0.11 (95% confidence interval [CI] 0.06 - 0.20) and 5.29 (95% CI 2.8029 -10.01), respectively (Table 1).
Using the X2 analysis, the consistency of the genotype frequency distribution to the Hardy–Weinberg proportion was investigated. In the control group, the frequency of the C allele was 0.94, and the frequency of the T allele was 0.05, whereas in the malnourished children, the frequency of the C allele was 0.31, and the frequency of the T allele was 0.68. According to the findings of this research, the percentage of homozygous genotype (TT) is highest gene” & “gene-environment”. Several genes have been linked to the regulation of folate or homocysteine metabolism and the risk of malnutrition.
Multiple candidate genes, racial variability, and population diversity all lead to the polymorphic heterogeneity of MTHFR enzymes involved in the folate-dependent homocysteine metabolism pathway having a distinct allele frequency. As a result, environmental factors and genetic factors play a role in the development of malnutrition.[3,6,8]
Several studies have shown that folate and vitamin B play essential roles in nearly all aspects of brain function. Their deficiencies are linked to cognitive dysfunction and hyper-homocysteinemia.[5,6,8] Compared to the control group, malnourished children had lower levels of vitamin B and folate in our current study. The extent to which malnourished children’s homocysteine levels were elevated (>4 fold) relative to the control group was of particular concern. Numerous clinical trials have established a connection between hyperhomocysteinemia and cardiovascular and neurological conditions, including dementia.[8] While the causal function of homocysteine in the onset of dementia is still disputed,[10,13,15] multiple significant reports have highlighted the dangers associated with elevated amounts of this non-protein amino acid.[23–27] Homocysteine levels are associated with a higher rate of cognitive loss, which can be slowed with the use of homocysteinelowering B vitamins.[5] Consequently, increasing vitamin B and folate intake results in a decrease in homocysteine levels in these malnourished children through interventions (dietary management or supplementation).[18] DNA synthesis and methylation, MTHFR enzymes are essential in the folate metabolic pathway. Intriguingly, the genetic vulnerability in different types of clinical issues in the last year, which has led to an increasing focus on the MTHFR C677T gene polymorphisms and the possibility of cognitive disability in malnourished children. A substitution mutation at nucleotide 677 (C677T) in the gene encoding the enzyme 5,10-methylenetetrahydrofolate reductase (MTHFR), which results in a 70 percent reduction in enzyme activity, is the most common genetic abnormality linked to homocysteine metabolism. According to the findings, there is a 20% increased risk of degenerative vascular disease.[16]
Epigenetic alteration and genetic polymorphism have been linked to disease and are closely correlated with methylation. Environmental factors can also affect subsequent risks for cardiovascular, behavioral, and metabolic disorders, even if they interfere with genomic DNA during crucial early life periods. Additionally, hereditary variations influence a variety of components of folate synthesis and the methionine cycle, including hydroxylysine, methionine, cysteine, and glutathione, as well as numerous enzymes, diet, and DNA methylation.[24–28]
Through these variances, it is possible to determine the Hcy content in plasma, which is a sensitive indication of vitamin B and folic acid insufficiency and also indicates the presence of a pathogenic mechanism.[13]
As a result, it has been suggested that these almost limitless variations arise early in life in response to epigenetically controlled gene expression alterations. Chronic deficits in folate, vitamin B-6, vitamin B-12, and methionine, on the other hand, will interrupt the usual metabolic cycle and raise Hcy levels, leading in cell damage. Several studies have been supported that Insufficient folate and cobalamin may trigger malnutrition in the fetus, according to several reports, since its deficiency impairs the function of an enzyme involved in folate metabolism and, at the same time, raises homocysteine levels and lowers vitamin B12 levels in comparison to normal children.[25–27] Homocysteine and cobalamin levels are therefore independent markers of malnutrition.
The MTHFR C677T gene can be mutated as a result of these conditions. However, the amounts of RBC folate and plasma homocysteine affect MTHFR gene polymorphism. As a result, malnutrition is a multifactor cause of metabolic disorders with a common variant in multiple genes.[12,15,24–28] Because folic acid, vitamin B12, and vitamin B6 are precursors of neurotransmitters, the connection between malnourished children and their deficiency results in elevated homocysteine levels in the blood.[24,25]
In malnourished children with increased total plasma homocysteine levels, serum, RBCs, and CSF folate levels were significantly lower. High homocysteine levels were associated with a high rate of C677T MHTFR mutation, according to[5,13,24,25] Therefore, understanding the genetic risks of malnutrition may aid in the identification of ideal targets for malnutrition intervention and treatment.
Malnutrition’s etiology and pathogenesis is a complex interplay of genetic and environmental factors. Since dietary intake and nutrient supplements are considered critical environmental factors, scientists have speculated that they may play a role in cancer growth. Furthermore, numerous studies have found a strong correlation between dietary nutrient quantity and quality and cancer incidence and pathogenesis.
In conclusion, the elevated plasma homocysteine levels observed in the malnourished children studied here, combined with lower folate and vitaminB12 levels, support pilot studies in these children involving homocysteine-lowering therapies are also related to disrupted MTHFR gene enzymatic activity.
Furthermore, iron, which is the essential nutrient for maintaining normal hemoglobin levels, appears to connect to cognitive ability. As a result, iron supplements appear to benefit malnourished children. Not only could such therapies enhance behavior and mental efficiency, but they could also reduce the likelihood of neurological and cardiovascular conditions later in life.
Individuals with the same dietary intake show significant differences in malnutrition growth. The difference in MTHFR polymorphisms may explain this, leading to the development of the concepts of nutrigenomics and nutrigenetics. The connection between specific nutrient intake and genetic variations in malnutrition pathogenesis could be explained by nutrigenomics and nutrigenetics. Nutrigenomics is often used to treat the development of cancer and pathogenesis, exposure to medication, and diet-related or underlying diseases. Following that, nutrigenomics could be used in an individualized nutritional consultation focused on the genetic profiles of the individuals to aid in the effective treatment of cancer. However, identifying risk factors and genetic and biochemical biomarkers for malnutrition can be used to develop optimized strategies for childhood malnutrition measures, testing, evaluation, and surveillance.
Funding: The present research was supported by the Department of Science and Technology and the Ministry of Health of the Government of India.
Conflict of Interest: Authors declared no conflict of interest.

Subscribe now for latest articles and news.