Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i03.010
Year: 2015, Volume: 1, Issue: 3, Pages: 33-34
Review Article
Dharitri M Bhat, Sanjay N Parate
Associate Professor, Department of Pathology, Government Medical College, Nagpur, Maharashtra, India
Address for correspondence:
Dr. Dharitri M Bhat, Associate Professor, Department of Pathology, Government Medical College, Nagpur, Maharashtra, India.
E-mail: [email protected]
A 50 years female presented with recurrent diarrhea and abdominal pain since last 6 months. History of weight loss present, no other complaints, general examination revealed only pallor.

Figure 1: Hematoxylin and Eosin, ×100

Figure 2: Hematoxylin and Eosin, ×100

|
Figure 1: Hematoxylin and Eosin, ×100
Figure 2: Hematoxylin and Eosin, ×100
Figure 3: Hematoxylin and Eosin, ×400 |
|
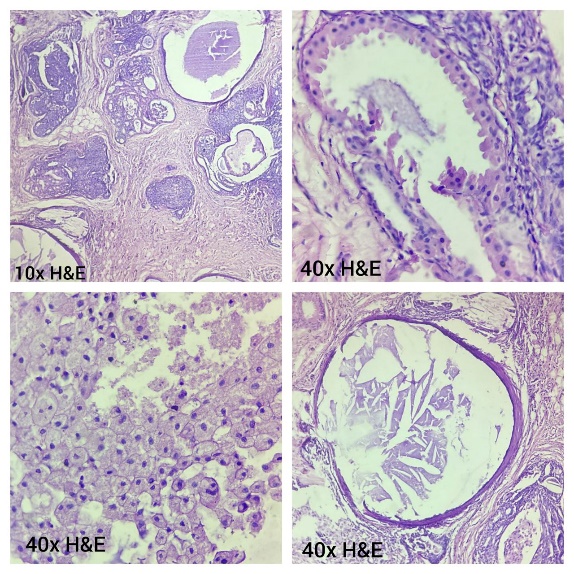
A 50 years female presented with recurrent diarrhea and abdominal pain since last 6 months. History of weight loss present, no other complaints, general examination revealed only pallor. USG abdomen: WNL Sections showing multiple mucosal tissue bits with lamina propria and focal ulceration. High power view is showing necrotic debris, blood, and few inflammatory cells and scattered large round to polygonal structures with the small pale nucleus. Engulfed RBCs can also be seen in oil immersion lens. Low power view of colonic biopsy, showing tissue bits. High power view showing large round to polygonal structures in necrotic tissue. Answer: Amoebic Colitis/Amoebic Ulcer Amoebic ulcers are quite common in developing countries like India. These are usually associated with poor socio-economic condition and poor hygiene. The most common affected organs are gastrointestinal tract, specially colon where it forms multiple ulcers. They often are the cause for recurrent abdominal pain and diarrhea, which may be blood mixed at times. Clinically, these lesions may mimic malignancy specially when accompanied by weight loss in elderly patients.[1] The diagnosis depends on recognition of trophozoite forms in stool or biopsy specimen or on serologic tests. Biopsy from typical amoebic ulcers show necrotic material, cellular debris with many acute inflammatory cells, predominantly neutrophils, admixed with a few histiocytes, lymphocytes, occasional eosinophils with fibrin strands and mucus in the background.[2] In between these cells, large, round structures with abundant, foamy, vacuolated cytoplasm and showing ingested red blood cells (Figure 3) are also seen. They have round nucleus with a small, deeperstaining center identified as kayosome. This helps in differentiating trophozoites from histiocytes with that they can be confused. These trophozoites are periodic acid-Schiff positive. Identification of these trophozoites of entamoeba histolytica is most crucial in the diagnosis of amoebic lesions such as amoebic liver abscess, amoeboma, and amoebic ulcers since these lesions show dramatic response to anti-amoebics.[3,4] |
Figure 3: Hematoxylin and Eosin, ×400
Subscribe now for latest articles and news.