Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i01.001
Year: 2021, Volume: 7, Issue: 1, Pages: 1-8
Original Article
M Sangeeta1, M Khizer Hussain Afroze2, K L Varalakshmi3
1Professor and Head, Department of Anatomy, MVJ Medical College and Research Hospital, Bengaluru, Karnataka, India,
2Assistant Professor, Department of Anatomy, MVJ Medical College and Research Hospital, Bengaluru, Karnataka, India,
3Associate Professor, Department of Anatomy, MVJ Medical College and Research Hospital, Bengaluru, Karnataka, India
Address for correspondence:
Dr. K L Varalakshmi, Department of Anatomy, MVJ Medical College and Research Hospital, Bengaluru, Karnataka. Phone: 9980902559. E-mail: [email protected]
Introduction: Injuries to the anterior cruciate ligament (ACL) are commonly encountered in day-to-day practice. The morphology of the intercondylar notch (ICN), in particular, the width, and shape of the notch are of anatomic interest predisposing to ligament injuries. The previous literature points to contradicting views on the association between ICN dimensions and cruciate ligament injuries.
Aim of the study: This study aims to study the morphometry of the ACL and ICN in 32 prosected lower limbs and to see if any association exists between the two.
Objectives The objectives of the study were to estimate the dimensions of ACL (maximum length and width) in 32 prosected lower limbs, estimate the dimensions of ICN (ICN width and depth) along with intercondylar (IC) width in 32 prosected lower limbs, and test the strength of association between the dimensions of ICN with the dimensions of ACL.
Materials and Methods: The study was done in the Department of Anatomy of MVJ Medical College and Research Hospital, Bengaluru. Thirty-two prosected lower limbs from the department of anatomy were used for the study.
Results: It was observed that IC width correlated positively with ACL length as well as ACL width. A strong positive correlation was also observed between IC width with ICN width. Femoral notch width index also correlated positively with ACL width.
Conclusions: The above study provides valuable data on the morphometry of ACL and its association with all dimensions of IC fossa unlike previous studies which have correlated the dimensions of IC fossa only with the thickness of ACL.
KEY WORDS:Anterior cruciate ligament, dimensions, Femoral notch width index, intercondylar notch, intercondylar width, morphometry.
Among the various ligaments of the knee joint, the anterior cruciate ligament (ACL) is most prone to injury constituting 50% of the total knee injuries.[1] The cruciate ligaments share both functional and anatomic relationship to the intercondylar notch (ICN).[2] A narrow ICN has been suggested as one of the risk factors to ACL injury.[3] This theory was substantiated by Souryal et al. who postulated that notch width index (NWI) is one of the predictors for risk of ACL injury.[3] However, there are lot of differing views on this as per literature. This could be attributed to the differing methodology used for estimating the dimensions of ACL and ICN in the previous studies wherein some studies were cadaver based some magnetic resonance imaging (MRI) and others arthroscopic based.
Hence, the objectives of this paper were to –
• Estimate the dimensions of ACL (maximum length and width) in 32 prosected lower limbs.
• Study the morphometric data of the ICN in relation to ICN width and depth and intercondylar (IC) width.
• Study the strength association between the dimensions of ACL with the dimensions of ICN.
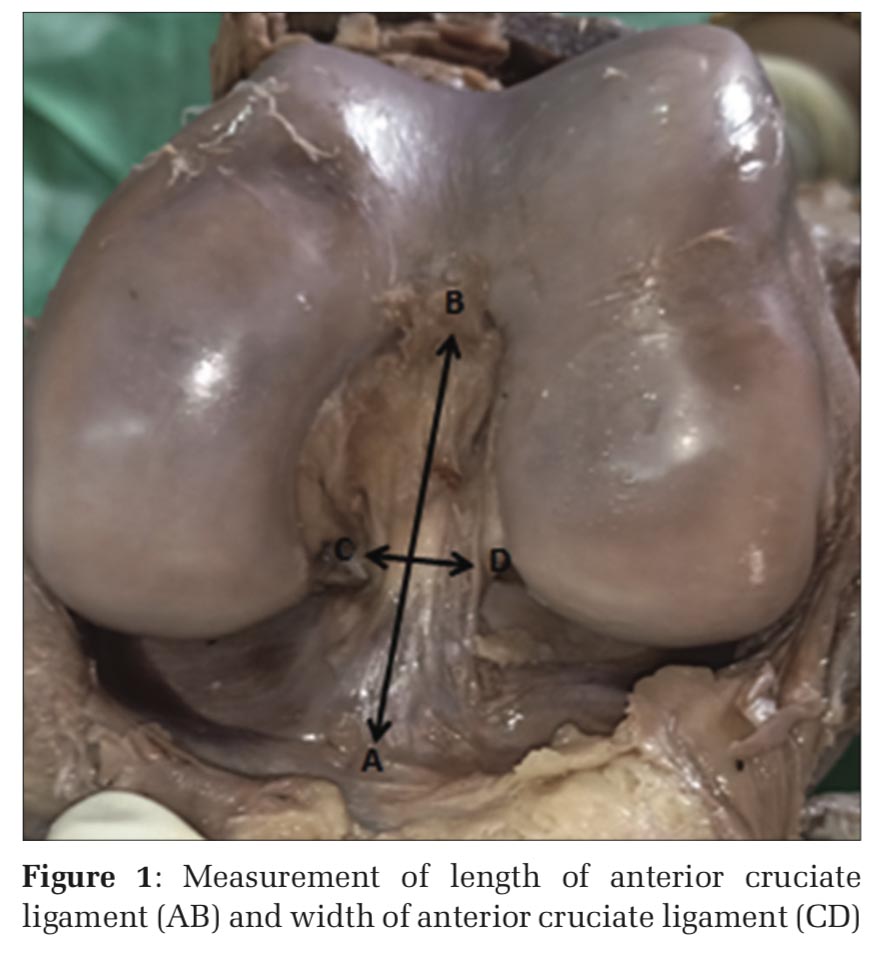
The study was done in the Department of Anatomy of MVJ Medical College and Research Hospital, Bengaluru. This was a descriptive pilot study conducted over a period of 1 month wherein 32 prosected lower limbs from the department of anatomy were used. Using a scalpel, the tendons of sartorius, gracilis, and semitendinosus were detached from their attachment on the tibia. The tendon of quadriceps was cut transversely just above the patella and the incision extended inferiorly around the patella passing 2–3 cm on either side of the ligamentum patellae. Patella along with the ligamentum patellae was turned downward to expose the cavity of knee joint. Infrapatellar folds and pads of fat were removed. The knee joint was flexed at 90° to examine the ACL. The ACL was measured for its length from its femoral to tibial attachments and width of ACL at middle third was estimated using digital Vernier calipers in mm (Figure 1).
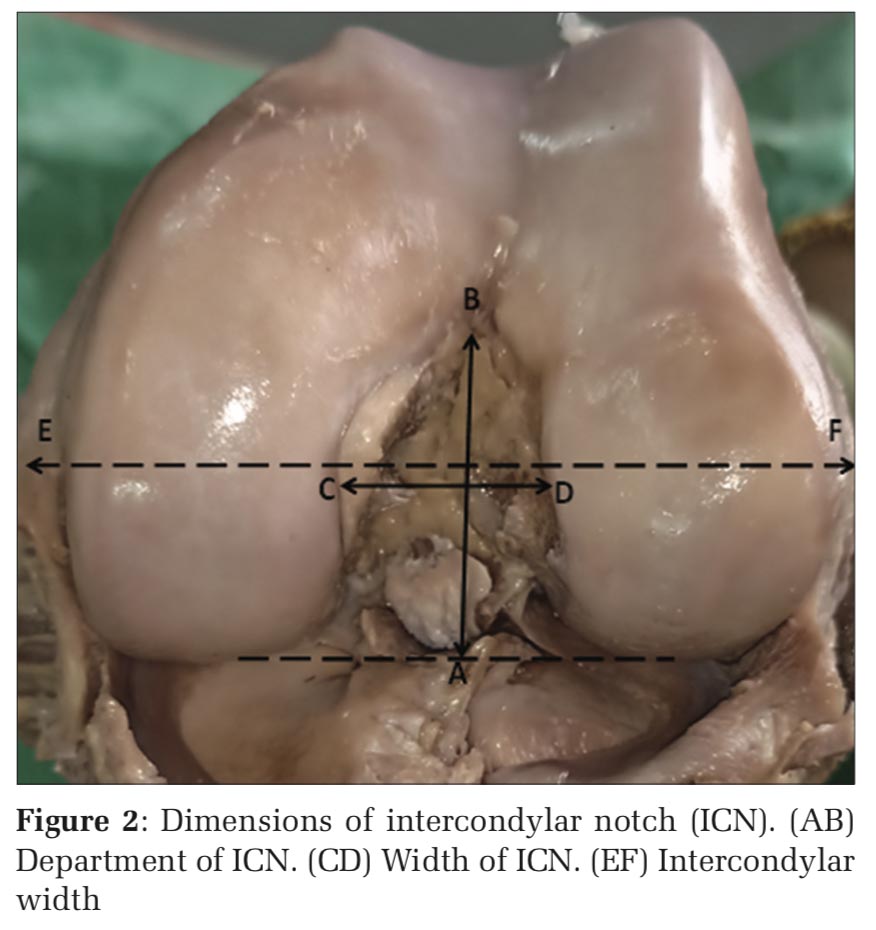
The femoral attachments of ACL and posterior cruciate ligament were cut and following dimensions of ICN were recorded using digital Vernier calipers, that is, ICN width which was measured as the distance from the medial articular cartilage margin of the lateral femoral condyle to the lateral articular margin of the medial femoral condyle, ICN depth was identified as its height at the maximum. In addition, IC width was measured as the distance between the medial and lateral epicondyles (Figure 2).
All the above parameters were measured in accordance with the guidelines of Anderson et al.[4]
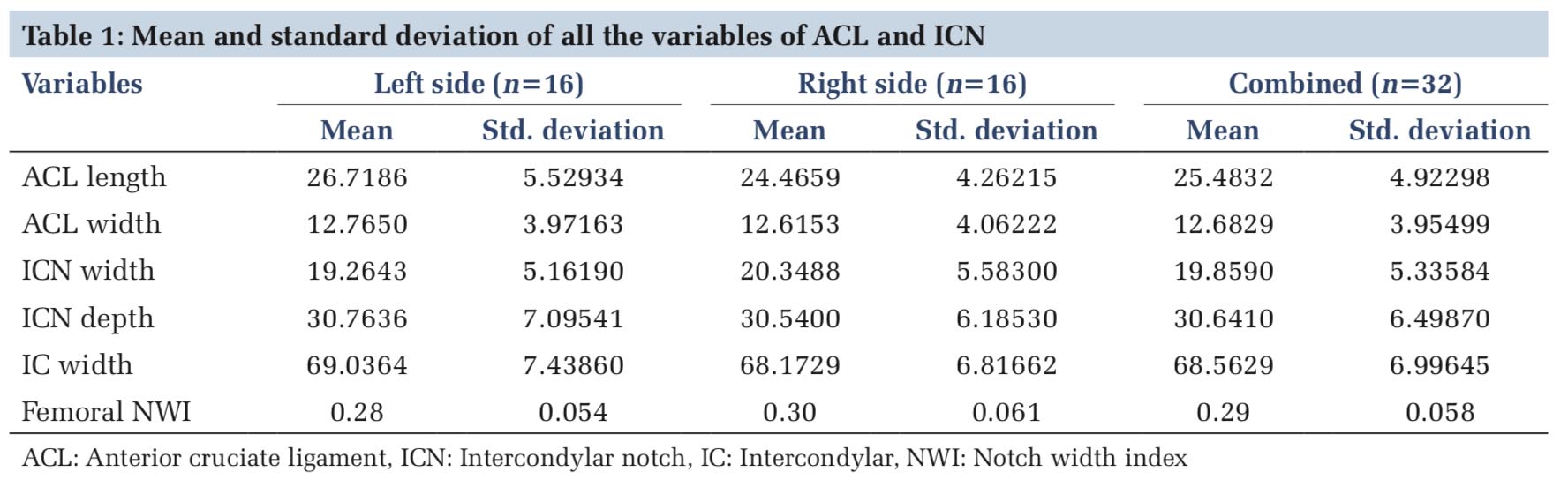
Table 1 shows the mean and standard deviation of all the variables of ACL and ICN.
The mean and standard deviations of all the variables of ACL, that is, length and width, ICN dimensions (ICN width and depth) along with IC width were computed with the help of SPSS software.
The combined mean length of the ACL of the right and left sides put together was 25.4832 ± 4.92298 mm. No statistical difference was observed between the mean length of ACL of the two sides.
The combined mean width of ACL of the right and left sides put together was 12.6829 ± 3.95499 mm. As evident from Table 1, the values did not differ statistically on the two sides. The combined mean width and depth of the ICN was 19.8590 ± 5.33584 mm and 30.6410±6.49870 mm, respectively. These variables also did not differ between the two sides.
The combined mean IC width was 68.5629 ± 6.99645 mm with no statistical difference between the two sides. Femoral NWI was calculated as ratio between ICN width to the IC width. The combined NWI was estimated as 0.29 ± 0.058, there being no statistical difference between the two sides.
The dimensions of ACL were compared with the dimensions of ICN along with IC width to see if any association existed between the two. Pearson’s correlation coefficient was used to test the association between the two.
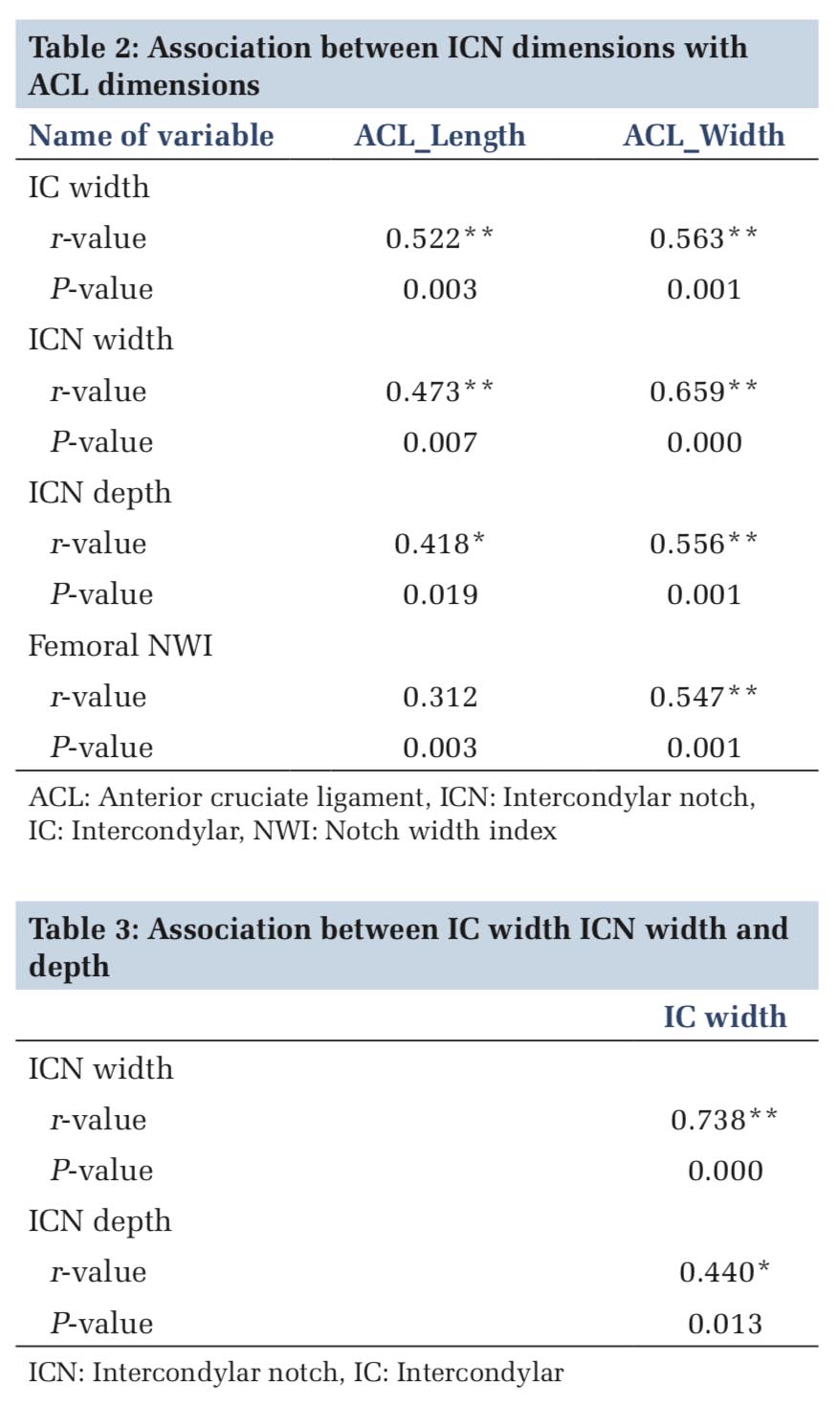
Table2 shows the association between ICN dimensions with ACL dimensions.
It was observed that IC width correlated positively with ACL length and ACL width.
A strong positive correlation was also observed between IC width with ICN width. NWI also correlated positively with ACL width.
Table 3 shows the association between IC width ICN width and depth.
IC width also correlated positively with ICN width and ICN depth, the association between the former being more strong. A strong positive correlation was also observed between ICN depth and ICN width.
Table 4 shows the relationship of ICN width with ICN depth.
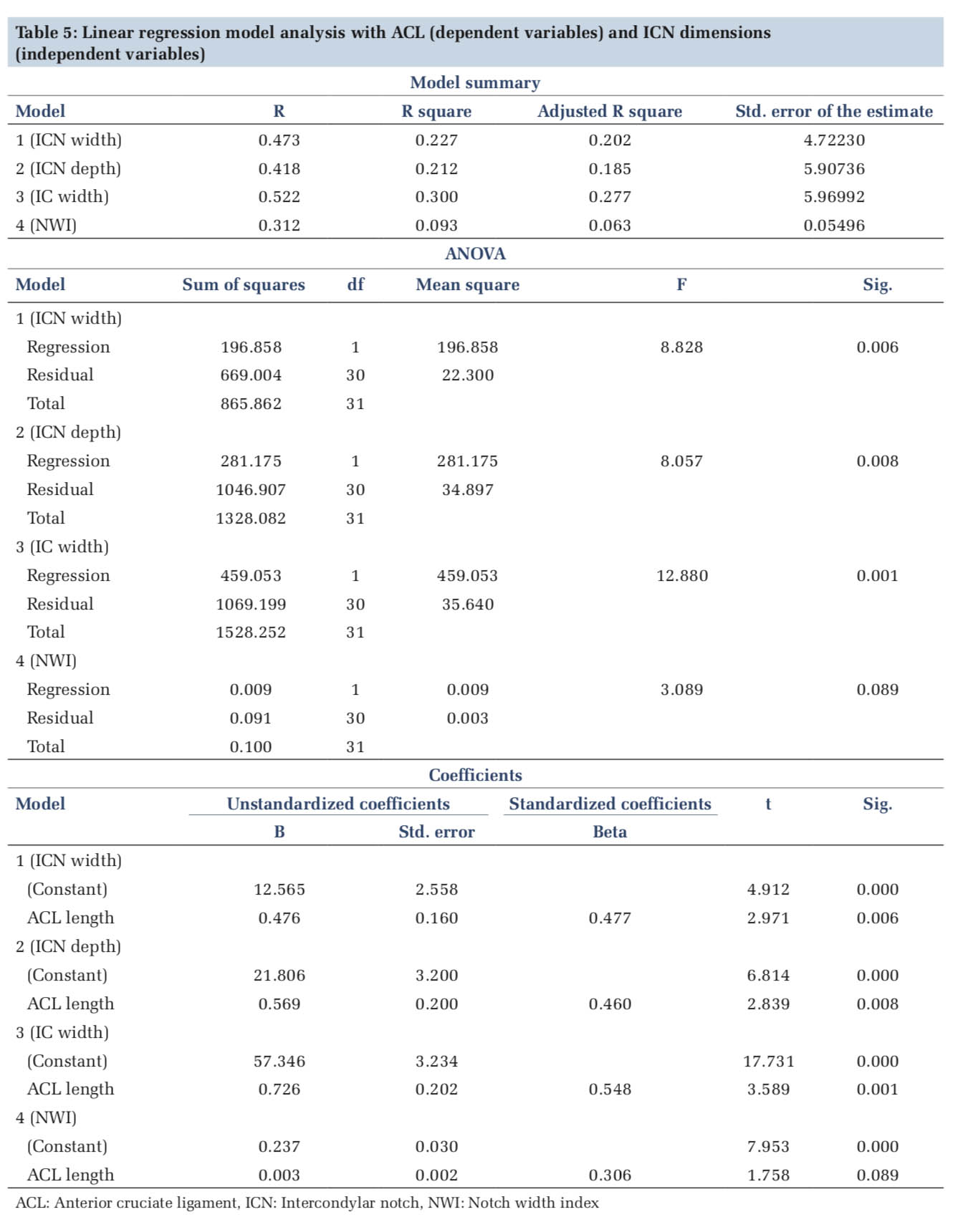
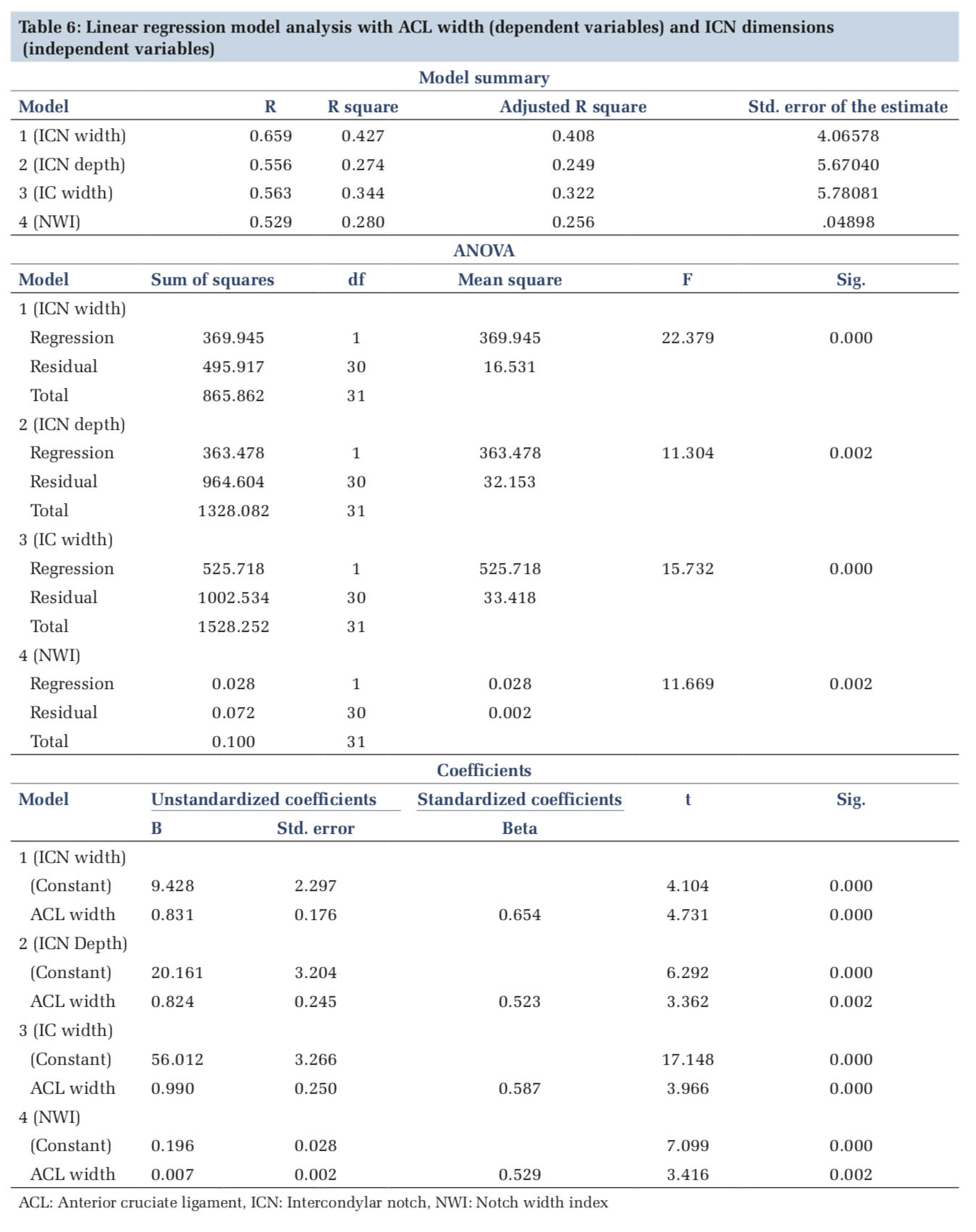
Tables 5 and 6 show the simple linear regression analysis between the ACL and ICN dimensions which was found to have a statistical difference.
As already mentioned, ACL injuries contribute to a major bulk of knee injuries. They are commonly observed as part of sports injuries (football, soccer, etc.). They usually present as a loud popping sensation in the knee along with swelling and restriction of motion and a feeling of giving away with weight-bearing. Knees with ACL injuries are more prone to osteoarthritis.[5] The previous studies have reported correlation between ICN width with ACL injury. There are, however, contradicting opinions in the literature regarding this. However, morphology of the ICN does affect the functioning of ACL.[6] This has an embryological basis wherein a well-developed ACL with two different bundles is observed at 20 weeks of gestational age, suggesting that early development of the knee joint is guided by the ACL. Cruciate ligaments present at this early stage of development could lead to the assumption that they interact with the resulting shape of the femoral condyles and the tibial plateau.[7]
Width of the ICN, in particular, correlates with the success of surgical reconstruction of ACL.[6] The previous studies have compared the dimensions of ICN in male and female and statistical significant difference in the width of the ICN between males and females was reported. This was cited as the reason for females more prone to ACL injuries due to narrow ICN dimensions.[8,9] NWI is used as an indicator for predicting notch stenosis.[10] Few studies have reported critical NWI ranging from 19 to 0.26. In our study, we observed the mean notch width index to be much higher than the critical value observed for knee injury.
Lombardo et al. studied the notch width radiographically in 615 male basketball players and observed no difference in critical notch stenosis in ACL injured versus non-injured patients.[5]
The mean width of the ICN observed in our study was comparable to the study by Ameet and Murlimanju; however, mean depth of ICN was slightly more in our study compared to theirs. The mean IC width was slightly less in our study in comparison to the values reported by Ameet and Murlimanju.[2].The mean femoral NWI was also slightly more in our study compared to theirs. This could possibly be attributed to the fact that their study was done on dry bones whereas we performed the measurements in prosected limbs.
Magnussen et al. studied the relationship between ACL graft thickness with incidence of ACL tears and concluded that as the thickness of the graft increased, reduced incidence of tears was reported.[11]
Oliveira et al. studied the relationship between the thickness of ACL with the anthropometric measurements of knee notably IC and interepicondylar distance using MRI scans. He observed that the mediolateral thickness of ACL in the middle third correlated positively with the IC distance in the axial plane. In our study also, IC width correlated positively with both ACL length and width.[12]
Contrary to the findings of Oliveira et al., a study by Muneta did not reveal any correlation between ACL dimensions and IC fossa dimensions.[13]
MRI studies by Charlton et al. have shown a positive correlation between volume of ACL and volume of IC fossa.[14]
Stijak et al. observed a positive correlation of ACL thickness with the IC width in male cadavers. He also compared the width of ACL in male and female cadavers and observed a statistically significant difference between the two accounting for higher rates of ACL tear in women.[14] Our study suffers from the limitation that we could not study gender differences as the study was done on prosected limbs. A study by Khodair et al. showed significant differences in distal femur morphology, in particular notch width and NWI in ACL injured and non- injured in both males and females.[15]
NWI in injured knees was observed to be 0.22 ± 0.008 by Görmeli et al.[16] Our study showed a much higher mean NWI.
The dimensions of ACL, that is, length and width observed in our study were compared with the previous studies. In our study, we have measured length of ACL as a whole without splitting it into anteromedial and posterolateral bundles. The mean length of ACL observed in our study was comparable to the results obtained by Kumar and Manimekalai, whereas the mean width of ACL was slightly more in our study compared to theirs.[17] Morphometric study of ACL by Dutta et al. has shown comparatively lower values than observed in our study.[18]
Yelicherla et al. studied the dimensions of ACL in male and female cadavers and reported higher values (statistically significant) in males.[19] However, the mean values of length and width of ACL observed in their study were significantly higher compared to our study.
Jayagandhi et al. have measured the length and width of ACL by bluntly separating them into anteromedial and posterolateral bundles in different positions of knee flexion, that is, 30, 60, and 90°.[20] However, as already stated, we have measured the length of ACL as a whole in 90° flexion.
The present study has limitations in terms of sample size due to the fact that it was done on prosected limbs hence gender comparisons also could not be established. We have not analyzed the dimensions of ACL by splitting into anteromedial and posterolateral bundles. Since this is a pilot study, the same data need to be validated by MRI and 3D imaging systems for more detailed assessment using a bigger sample size.

The above study provides valuable data on the morphometry of ACL and its association with dimensions of IC fossa. Our study is also the first of its kind to correlate all the dimensions of IC fossa with each other as well as with ACL dimensions as most of the previous studies have correlated the dimensions of IC fossa only with the thickness of ACL. This study shows that the dimensions of ACL are much less in Indian population compared to the Western population. It also showed IC width correlated positively with ACL length and ACL width. A strong positive correlation was also observed between IC width with ICN width. Femoral NWI also correlated positively with ACL width.
Subscribe now for latest articles and news.