Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v8i3.22.276
Year: 2022, Volume: 8, Issue: 3, Pages: 264-270
Original Article
Debabrata Maiti1 , Tapobrata Mitra2 , Manisankar Nath3 , Swapnadeep Sengupta4
1Medical Officer, WBUHS, Kandi, West Bengal, India,
2Associate Professor, Department of Anaesthesiology and Critical Care, Murshidabad Medical College and Hospital, Berhampore, West Bengal, India,
3Assistant Professor, Department of Anaesthesiology and Critical Care, Jalpaiguri Government Medical College, Jalpaiguri, West Bengal, India,
4Assistant Professor, Department of Anaesthesiology and Critical Care, Calcutta National Medical College and Hospital, Kolkata, West Bengal, India
Address for correspondence:
Swapnadeep Sengupta, Assistant Professor, Department of Anaesthesiology and Critical Care, Calcutta National Medical College and Hospital, Kolkata, West Bengal, India.
E-mail: [email protected]
Received Date:24 May 2022, Accepted Date:28 September 2022, Published Date:03 December 2022
Background and aims: Epidural analgesia has been considerably used for postoperative analgesia in Orthopaedic surgeries, however, combination of opioid and non-opioid medications in the perioperative period seems to provide an effective alternative. Objectives: To compare the efficacy of pre-emptive multimodal analgesia with combined spinal epidural for postoperative analgesia in lower limb arthroplasties. Materials and methods: 50 patients scheduled for elective lower limb Arthroplasties were randomly divided into two groups. Spinal anaesthesia with 2.5ml of 0.5% Bupivacaine (heavy) plus 0.5ml (25µg) Fentanyl was given in both the groups for procedure. Group I received Cap. Pregabalin 150mg and Inj Paracetamol 1000mg IV 1 hour before surgery and 75mg 12 hourly and 1000mg IV 8 hourly respectively, while Group II received epidural top up with 10 ml of 0.125% bupivacaine 8 hourly, both for 3 days postoperatively. Perioperative haemodynamics, postoperative VAS, rescue analgesics requirement, and Patient satisfaction level were monitored for 72 hours. Results: Postoperative VAS score was significantly higher in Group II from 4th hour postoperatively, and, accordingly, more patients in this group required rescue analgesia (21 and 20 in Group II vs 10 and 1 in group I in 12-24 hrs and 24-36 hrs respectively with p value <0.001). Modified Bromage score, haemodynamics and side effect profiles were comparable in the groups, however, patient satisfaction level was more in Group I (p value <0.001) after 72 hours. Conclusion: Pre-emptive multimodal analgesia can be used as an effective alternative to epidural for postoperative analgesia in patients undergoing lower limb joint replacement surgeries.
Keywords: Pre-emptive multimodal analgesia, Combined spinal epidural analgesia, Lower limb arthroplasties, Postoperative analgesia
Perioperative pain management has always been an issue of immense importance, particularly to the anaesthesiologists. Inadequate perioperative analgesia can lead to several significant deleterious effects, including myocardial ischemia, infarction, pulmonary infections, paralytic ileus, urinary retention, thrombo-embolism, impaired immune functions and anxiety, thereby, resulting in patient dissatisfaction, impaired patient rehabilitation and prolonged hospitalizations. 1, 2, 3
Orthopaedic surgeries with extensive bone handling, in the likes of hip or knee arthroplasty, 4 demand even more intense pain control strategies as the pain in these cases are much more than usual.
The domain of pain management has, traditionally, been dealt with intravenous or oral analgesics of various groups, with opioids being considered as the cornerstone, 5 along with non-steroidal anti-inflammatory drugs (NSAIDS). However, both the groups of drugs are associated with several adverse effects, including respiratory depression, postoperative nausea and vomiting (PONV), over-sedation, confusion, dizziness, puritus, urinary retention, ileus and constipation (opioids) and gastritis, gastric ulcers, increased bleeding, and renal impairments (NSAIDS).
The emergence of regional analgesia and anaesthesia has brought a drastic change in the outlook and methods of perioperative analgesia, central neuraxial block being the most commonly practiced procedure. Though it has the advantages of better postoperative analgesia with decreased consumption of narcotic, the procedure is also not devoid of any complications and the incidences of epidural bleeding (with prophylactic anticoagulation therapy), diminished muscle control, urinary retention, and nerve damage, 5 pose serious limitation to its use in various situations.
Multimodal analgesia technique, as introduced and refined by Kehlet and Dahl 6 and Wall, 7 involves administration of combination of multiple analgesics or modalities at various time points during the perioperative period. This technique of combining multiple analgesic drugs with different mechanisms and pathways of action is also being considered by many as the best way to achieve maximal control of pain after hip and knee arthroplasty. 8
Adequate pain control after knee and hip arthroplasty has been found to be achieved with a combination of drugs used during the preoperative (NSAIDS, COX-2 inhibitors, anticonvulsants), intra-operative (opioids, local anaesthetics), and the postoperative periods (opioids, NSAIDS, COX-2 inhibitors, α2-Agonists, NMDA antagonists, anticonvulsants, and centrally acting analgesics as acetaminophen / paracetamol).
The rationale for this strategy is the achievement of sufficient analgesia due to the additive or synergistic effects between these different classes of analgesics. This also allows a reduction in the doses of individual drugs and thus, lowering the incidences of adverse effects from any particular medication used for peri-operative pain management, thereby, providing shorter hospitalization time, improved recovery and function 9 and possibly decreased healthcare costs. 10
With this background, this study was designed and conducted to assess the efficacy and safety of Pre-emptive Multimodal analgesia in comparison with Combine Spinal Epidural analgesia (CSEA) for postoperative analgesia in Total Knee Arthroplasty (TKA) and Total Hip Arthroplasty (THA).
After receiving Institutional Ethics Committee approval, this study was conducted for a period two years at the Department of Anaesthesiology and Critical Care and Orthopaedics wards of Command Hospital (Eastern Command). Fifty (50) patients of either sex in the age group of 30 to 75 years belonging to ASA I or II, admitted for elective Joint Arthoplasty Surgeries of Lower Limbs were included in this study, whereas patients having contraindication for spinal anaesthesia and those with significant cardio respiratory, metabolic, renal and hepatic disorders were excluded from the same.
After taking a written informed consent and doing a meticulous preanaesthetic check-up, the patients were allocated randomly, by opening sealed envelopes in either of two groups, comprising of 25 patients each. Tablet Alprazolam 0.25mg were given orally to each patient overnight on the day before surgery.
After receiving the patients in the operation theatre, all were administered 10ml/kg of Ringers Lactate solution as preload. Baseline pulse rate, blood pressure, respiratory rate, SpO2 and ECG were recorded.
Patients of Group I received Cap. Pregabalin 150mg and Inj Paracetamol 1000mg IV 1 hour before surgery. Then, spinal anaesthesia was provided, in sitting position, at L3-L4 interspace with 2.5ml of 0.5% Bupivacaine (heavy) plus 0.5ml (25µg) Fentanyl following standard procedure. Thereafter, just before the prosthesis was implanted, the deep tissues (like collateral ligaments, posterior aspect of the capsule, tendons, fat pad, periosteum, and synovium) and just before the wound closure the subcutaneous tissues were infiltrated with 150ml of 0.1% Bupivacaine plus 1mg Adrenaline. Postoperatively, patients received Cap Pregabalin 75mg 12 hourly and Inj Paracetamol 1gm (100ml IV infusion) 8 hourly for 3 days.
Patients of Group II, were placed on the operating table in sitting position and epidural catheter was placed first at L2-L3 interspace with a 16G Tuohy needle; epidural space being identified by ‘Loss of Resistance’ technique using a LOR syringe. After reaching the space, test dose of 2% xylocaine with adrenaline was injected and observed for any motor block or rise in heart rate. Epidural catheter was finally placed 3 to 5 cm in the epidural space through the Tuohy needle and the needle was withdrawn. Next, a spinal needle was introduced through the lower interspace for subarachnoid block and after return of clear cerebrospinal fluid, patients received a single intrathecal injection of 2.5ml of 0.5% Bupivacaine (heavy) with 0.5ml (25µg) Fentanyl. After the intrathecal injection, the spinal needle was withdrawn and the epidural catheter was adequately secured and fixed in proper position with Elastoplast. The patients were quickly positioned supine and then appropriately for the surgery. Postoperative analgesia was maintained with epidural top up with 10 ml of 0.125% bupivacaine 8 hourly for 3 days.
Intraoperatively, any episode of hypotension was managed with Inj. Phenylephrine 100 µg iv bolus and severe bradycardia with Inj. Atropine 0.6 mg iv.
All vital parameters were studied at regular intervals intraoperatively till shifting the patients to the ward. Assessment of pain was done by patients themselves, and for this assessment visual analogue scale (VAS) was used, the criterion of which was explained to them during the preanaesthetic visit. Injection Tramadol 100mg was used as rescue analgesic and was given at a VAS score of more than 40.
During the postoperative period, Number of Rescue Analgesia, Ramsay Sedation Scale, Modified Bromage Scale and Satisfaction Level were monitored for analgesia, sedation, return of motor functions along with Heart Rate, BP, SpO2, Respiratory Rate and any other side effects like nausea, vomiting, headache, pruritis, urinary retention, in each group, initially 2 hourly for 6 hours, then 6 hourly for 24 hours and then 12 hourly for a period of 72 hours.
Statistical Package for Social Sciences software version 20 (IBM) was used for statistical analysis and PS Power and Sample Size Calculations Version 2.1.30 (William Dupont and Walton D Plummer), February 2003, for sample size calculation. The sample size required was calculated considering an α-error of 0.05, power 0.90 or 90%, thus a p value is less than 0.05 it has been considered as significant. Continuous variables were expressed as Mean ± Standard Deviation and compared across the 2 groups using unpaired t test, whereas Categorical variables were compared across the 2 groups using Pearson’s Chi Square test for Independence of Attributes.
The two groups in this study were comparable in terms of demography, ASA status and types of surgery. (Table 1)
|
Criteria |
Group |
P value |
Significance |
||
|
I |
II |
||||
|
Age (Mean ± SD) |
57.8 ± 11.16 |
58.04 ± 10.97 |
0.939 |
Not Significant |
|
|
Sex (No. of patients) |
Female |
8 |
11 |
0.382 |
Not Significant |
|
Male |
17 |
14 |
|||
|
ASA (No. of patients) |
I |
14 |
11 |
0.396 |
Not Significant |
|
II |
11 |
14 |
|||
|
Surgery (No. of patients) |
THA |
11 |
10 |
0.774 |
Not Significant |
|
TKA |
14 |
15 |
|||
In terms of Postoperative VAS score, Group II had a significantly higher VAS score from the 4th hours postoperatively and it persisted likewise till the whole study period as evident from Table 2.
|
Time |
Group |
P Value |
Significance |
|
|
I |
II |
|||
|
Mean ± Std. Deviation |
Mean ± Std. Deviation |
|||
|
1 hour |
10 ± 2.5 |
10 ± 3.2 |
0.625 |
Not Significant |
|
2 hours |
23.8 ± 4.4 |
24.4 ± 3.91 |
0.612 |
Not Significant |
|
4 hours |
42.4 ± 7.23 |
53.6 ± 5.69 |
<0.001 |
Significant |
|
6 hours |
48 ± 7.07 |
60 ± 9.13 |
<0.001 |
Significant |
|
12 hours |
49.2 ± 6.4 |
61.2 ± 7.26 |
<0.001 |
Significant |
|
18 hours |
43.8 ± 6.96 |
54.4 ± 5.07 |
<0.001 |
Significant |
|
24 hours |
34.4 ± 6.51 |
53.2 ± 6.27 |
<0.001 |
Significant |
|
36 hours |
33.2 ± 5.38 |
44.4 ± 6.51 |
<0.001 |
Significant |
|
48 hours |
26 ± 4.33 |
35.4 ± 4.77 |
<0.001 |
Significant |
|
72 hours |
15.2 ± 4.2 |
24 ± 4.08 |
<0.001 |
Significant |
Accordingly, patients in Group II required more number, thus amount of rescue analgesic dose. (Table 3).
|
Time |
Group |
P value |
Significance |
|
|
I |
II |
|||
|
0-12 hours |
13 (52%) |
20 (80%) |
0.037 |
Significant |
|
12-24 hours |
10 (40%) |
21 (84%) |
<0.001 |
Significant |
|
24-36 hours |
1 (4%) |
20 (80%) |
<0.001 |
Significant |
|
36-48 hours |
0 (0%) |
9 (36%) |
0.001 |
Significant |
|
48-72 hours |
0 (0%) |
0 (0%) |
NA |
NA |
Patients in Group II also demonstrated statistically significant higher Modified Bromage Score in the 4th hour of study as shown in Table 4.
|
Time |
Group |
P value |
Significance |
|
|
I |
II |
|||
|
4 hours |
20 (80%) |
25 (100%) |
0.018 |
Significant |
|
24 hours |
8 (32%) |
9 (36%) |
0.765 |
Not Significant |
|
48 hours |
0 (0%) |
0 (0%) |
NA |
NA |
|
72 hours |
0 (0%) |
0 (0%) |
NA |
NA |
Ramsay Sedation Score also differed significantly during 1st 24 hours (Table 5).
|
Time |
Score |
Group |
P value |
Significance |
|
|
I |
II |
||||
|
4 hours |
1 |
0 (0%) |
10 (40%) |
<0.001 |
Significant |
|
2 |
25 (100%) |
15 (60%) |
|||
|
24 hours |
1 |
0 (0%) |
10 (40%) |
<0.001 |
Significant |
|
2 |
25 (100%) |
15 (60%) |
|||
|
48 hours |
1 |
0 (0%) |
0 (0%) |
NA |
NA |
|
2 |
25 (100%) |
25 (100%) |
|||
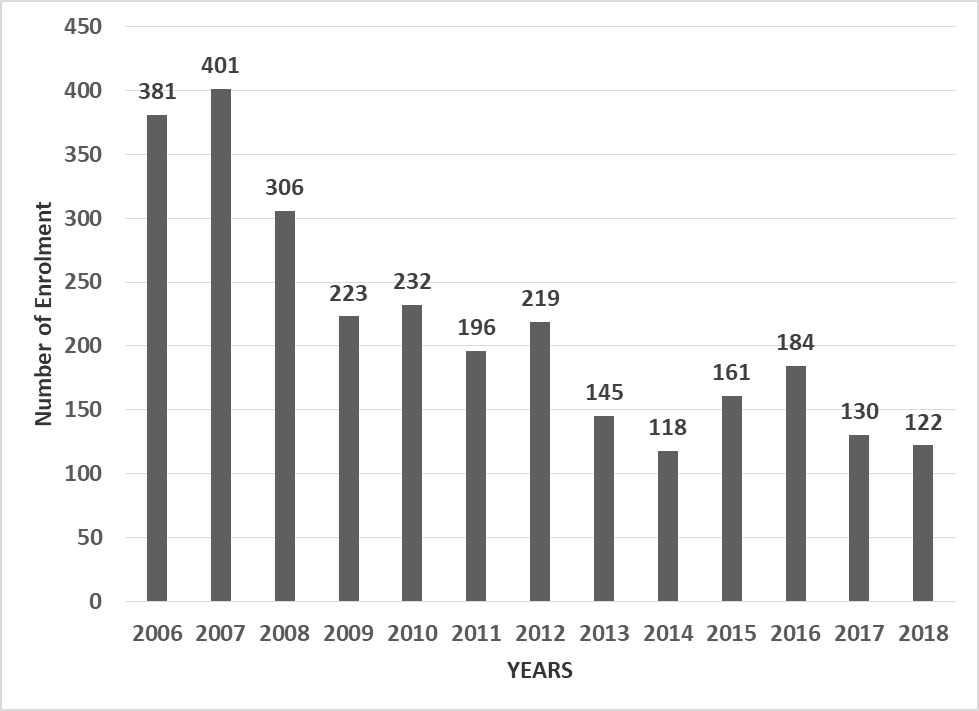
Figure 1 shows that the satisfaction of the patients with the measures taken to control pain, reveal a significant difference between the two groups at the end of 72 hour after the surgery (P-value = 0.001).

The hemodynamic parameters and side effect profiles were comparable in both the groups.
Pain is a subjective and multidimensional experience as described by McCaffery as "pain is whatever the experiencing person says it is and exists whenever he/she says it does". 11 It causes significant distress to patients and has adverse effects on the endocrine and immune function 12 which can affect wound healing 13 and cardiopulmonary and thromboembolic diseases. 14 Postoperative pain is one of the most frequently reported symptoms. 15
Effective pain control is a major concern in the postoperative management of knee / hip surgeries. The emphasis is also on shorter hospital stay, cost-effective use of resources, and early mobilization of the patient.
As the postoperative pain management has evolved over the decades from intramuscular and intravenous routes to epidural infusions, the last one remains the "gold standard" of pain relief after TKA/THA. However, this technique is also not devoid of adverse effects, hence an effective alternative has always been on the cards. Multimodal Analgesia, involving administering a combination of opioid and nonopioid analgesics (and adjuvant agents) that act at different sites within the central and peripheral nervous systems in an effort to improve pain control, represents an increasingly popular approach to preventing postoperative pain. 16, 17
With this perspective, this study was designed with an aim of comparing the postoperative analgesic efficacy and safety of Pre-emptive Multimodal Analgesia and Combine Spinal Epidural Analgesia (CSEA) for postoperative pain management in Total Knee Arthoplasty (TKA) and Total Hip Arthoplasty (THA).
The results of this study confirm that multimodal analgesia protocol offers significantly better pain relief compared to epidural technique after knee and hip arthoplasty surgeries as reflected by the VAS scores, that was significantly lower at 4, 6,12, 18, 24, 36, 48 and 72 hours in Group I compared with values in Group II (P < 0.05). Similar results were found by Andersen et al 18 who compared wound infiltration combined with intra articular injection of local anaesthetics for pain relief after total hip arthroplasty (THA) with the well-established practice of epidural infusion. Though pain levels at rest and during mobilization were similar in both groups but significantly reduced in the first one after cessation of treatment. However, Barrington et al 19 and Singelyn et al 20 in their respective studies found either continuous femoral nerve block or intravenous patient-controlled analgesia equally efficacious with epidural analgesic technique.
Regarding the use of rescue analgesics, in the present study, lesser number of patients in Group I required Inj Tramadol as against those in Group II throughout the whole period of initial 48 hours, which was also found to be statistically significant (p < 0.05). Chelly et al 21 in their study to determine the effects of continuous femoral infusion (CFI) on total knee arthroplasty recovery compared patient-controlled analgesia (PCA) with morphine with patients receiving sciatic blocks followed by CFI, and another group receiving epidural analgesia alone. They found blocks reduced postoperative morphine requirement by 74% in the 1st two groups in comparison to 35% in 3rd group (p<.05). Similarly, Andersen et al 18 in their study comparing continuous epidural infusion with local hip infiltration in patients undergoing elective THA under spinal block found that narcotic consumption was significantly reduced in the infiltration group A compared to the epidural group E (p = 0.004). These studies were at par with the results of the present study. In another study, however, Dushanka Zaric et al 22 found no difference in amount of morphine consumption on POD1 and POD2 between epidural (32.6±26 & 30.2±26.3) and femoral nerve block groups (31±26 & 32.3±25.7), though the addition of fentanyl to ropivacaine 0.2% for epidural infusion might have resulted in a better analgesia, reducing the need for rescue analgesic, in it.
Motor blockade as assessed with modified Bromage scale at 4, 24 and 48 hours in Group I and Group II patients were almost similar and not statistically significant, except for the 4th hour in this study. Motor blockade was more intense in the operated limb in Group I whereas the non-operated limb was more blocked in Group II. Similar findings were found by Dushanka Zaric et al 22 in their study where they compared epidural analgesia with continuous femoral-sciatic nerve blocks after TKA and deduced that motor blockade was more intense in the operated limb on the day of surgery and the first postoperative day in the peripheral nerve block group (P = 0.001), whereas the motor block was more intense in the non-operated limb in the epidural group on the day of surgery (P = 0.0003).
The satisfaction of the patients with the measures taken to control pain in this study, reveal a significant difference between the two groups at the end of 72 hour after the surgery (P-value =0.001). In group I the results were as follows; “very good” (4), “good” (16), “satisfactory” (5) and “poor” (0) and group II reported 6 patients as “good”, 15 patients as “satisfactory” and 4 patients as “poor”. In similar previous studies, Thorsell et al 23 compared the local infiltration anaesthesia technique with epidural anaesthesia and found seventy-six percent of the local infiltration anaesthesia patients were "very satisfied" with their postoperative pain control method, compared to 40% of the epidural anaesthesia patients. However, Davies at al 24 in their study found combined femoral (3-in-1) and sciatic nerve block equally satisfactory with epidural blockade for postoperative knee arthroplasty analgesia.
The side effect profile in both the groups in this study was comparable and statistically insignificant. Similar findings regarding the side effects were found in several other similar studies, like those of Capdevila et al 25 and Singelyn et al. 20
Thus, from this study, we can conclude that Pre-emptive Multimodal analgesia can be used as an effective postoperative analgesic technique in patients undergoing joint replacement surgeries of lower limbs, as it offers a practical alternative to epidural analgesia, representing the optimal analgesia during rest and during activity with fewer side effects and greater patient satisfaction.
Subscribe now for latest articles and news.