Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2018.v04i01.004
Year: 2018, Volume: 4, Issue: 1, Pages: 18-22
Original Article
Sanjib Kumar Das1, Ipsita Acharya2*, Sasmita Pariida3, Jayshree Mohanty4, Mamata Singh5, Basanta Manjari Swain6
1Resident, Department of Radiodiagnosis, SCB Medical College,Cuttack,
2Resident, Department of Radiodiagnosis, SCB Medical College,Cuttack,
3Professor, Department of Radiodiagnosis, PRM Medical College, Baripada,
4Professor, Department of Radiodiagnosis, SCB Medical College, Cuttack,
4Asst Professor, Department of Radiodiagnosis, SCB Medical College, Cuttack,
5Assoc. Professor, Department of Radiodiagnosis, SCB Medical College, Cuttack
Address for correspondence:
Dr. Ipsita Acharya, Resident ,Dept. of Radiodiagnosis, SCB Medical College,Cuttack - 753 007, Odisha, India. Phone: +91-9439961696. E-mail: [email protected]
Objectives: The objective of the study was to establish normative fetal kidney length (FKL) ranges in third- trimester pregnancy and comparing its accuracy with conventionally used biometric parameters.
Introduction: FKL was compared with conventional parameters such as biparietal diameter, head circumference, abdominal circumference (AC), and femur length using Pearson’s correlation coefficient in third-trimester pregnancy as an adjunct in the determination of gestational age (GA).
Materials and Methods: The study was conducted on 152 singleton uncomplicated pregnancies in their third trimester (28–40 weeks) who were sure of their last menstrual period. After measurement of conventional parameters, FKL was measured, and correlation was obtained with GA and its efficacy was compared with other parameters.
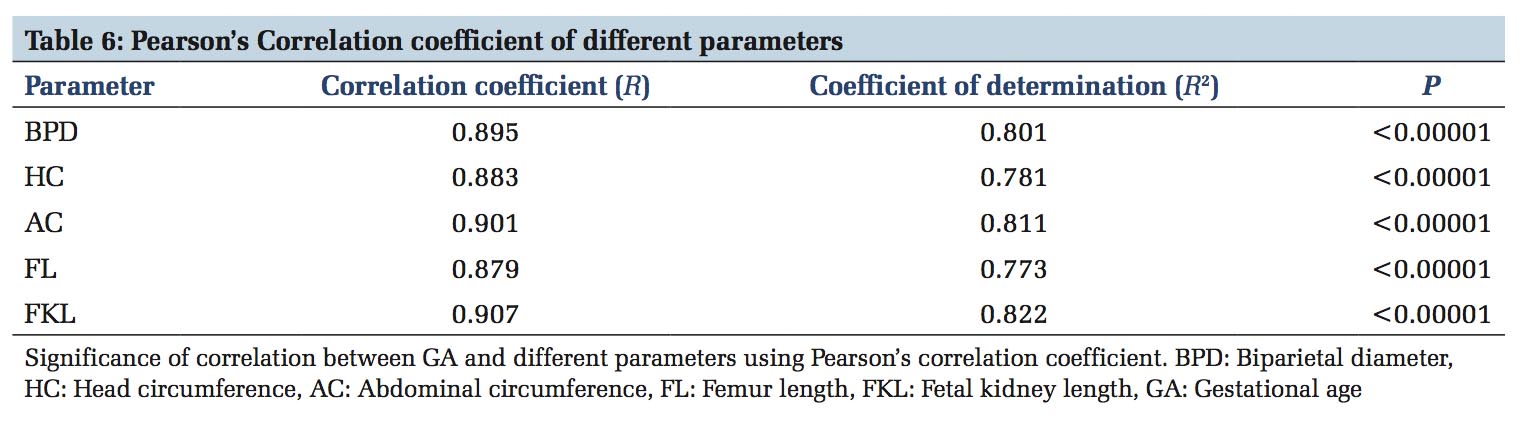
Results: FKL showed a Pearson’s correlation coefficient of 0.907 and a determination coefficient of 0.822 with GA. The test was significant at P < 0.05. It was followed by AC with a correlation coefficient of 0.901.
Conclusion: FKL showed a strong correlation with GA compared to other conventional parameters and can easily be included in routine obstetric scan to enhance the accuracy of GA measurement and in cases where conventional parameters are difficult to obtain, especially in third trimester due to head engagement, asynclitism, and in breech presentation.
KEY WORDS: Abdominal circumference, biparietal diameter, femur length, fetal kidney length, gestational age, head circumference.
For any obstetrician, it is of utmost importance the fetus in assessing the growth of the fetus and to determine the expected date of delivery. Fetal growth retardation and macrosomia may be missed if accurate GA is unknown. Previously, patient’s history and clinical signs were routinely utilized to determine the GA. In 1958, Sir Ian Donald took the landmark step in implementing ultrasound (USG) for obstetric scan. Biparietal diameter (BPD) was first used to determine the GA in third trimester. Since then many other parameters have been used, conventional ones being head circumference (HC), abdominal circumference (AC), and femur length (FL).
Fetal kidneys grow in a linear fashion with the GA. They are easy to identify after mid-trimester at around 18 weeks. Hence, this study was undertaken to correlate fetal kidney length (FKL) with GA and to compare its efficacy with other routine parameters that are currently used.
Aims and objectives
After informed consent, 152 pregnant mothers with uncomplicated singleton pregnancies who were sure of their GA were included in this study carried between September 1, 2015, and September 31, 2017,in the Department of Radiodiagnosis in collaboration with Department of Obstetrics and Gynaecology at SCB Medical College, Cuttack.
Patients with anomalous fetus, suspected intrauterine growth restriction, unknown last menstrual period (LMP), multiple gestations, and fetal hydroureteronephrosis were excluded from the study. Oligo/polyhydramnios, fetal death, and failure to visualize the kidneys were also included in the exclusion criteria.
Phillips HD 7 USG machine was used for measurement and all the data were collected using the same 2–5 MHz curvilinear probe. Average of three measurements was taken for all the parameters by the same observer and tabulated. The standard methods for obtaining the BPD, HC, AC, and FL as given in the textbook of USG by Rumack et al.
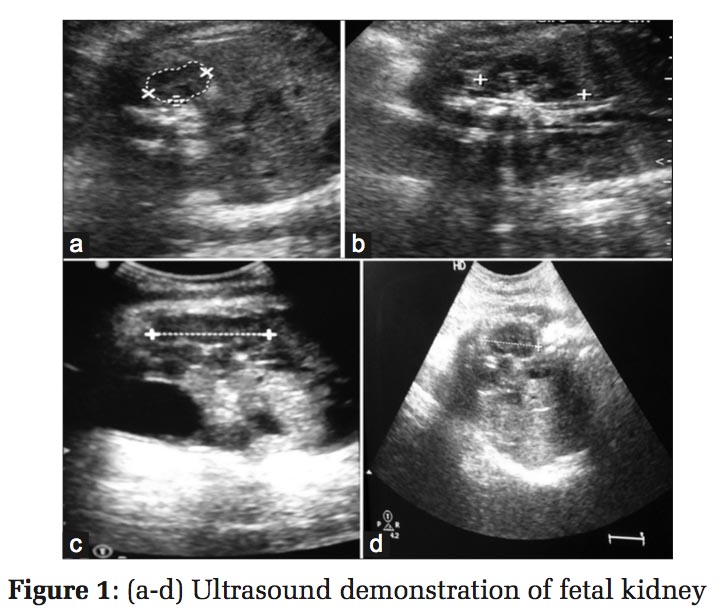
For fetal kidney, first, the transducer was placed in such a manner that the fetal spine was visible longitudinally. With slight angulation of the transducer, the paravertebral plane was obtained where the fetal kidney was visible in its whole length. Separate measurements were taken for both the kidneys and averages were taken [Figure 1].
Data were tabulated and all the statistical analyses were done using SPSS software. Pearson’s correlation coefficient was calculated for each parameter and P value was obtained from that. All the averages were presented as mean±standard deviation.
All the patients were grouped under three age groups; 57% were between 26 and 35 years, whereas 42% were between 15 and 25 years. Nearly 34% of all patients were nulliparous, while 44% were the mothers of one child. If consider the weight of the patients, more than half (54%) of the patients were between 50 and 60 kg. All the patients were more or less evenly distributed among different GA. Of 152 patients, 66 were between 28 and 32 weeks, 55 belonged to 33 to 36 weeks, and rest 34 were between 37 and 40 weeks.
With these demographic data, we started measuring the parameters and correlated them one by one with the GA calculated using LMP.
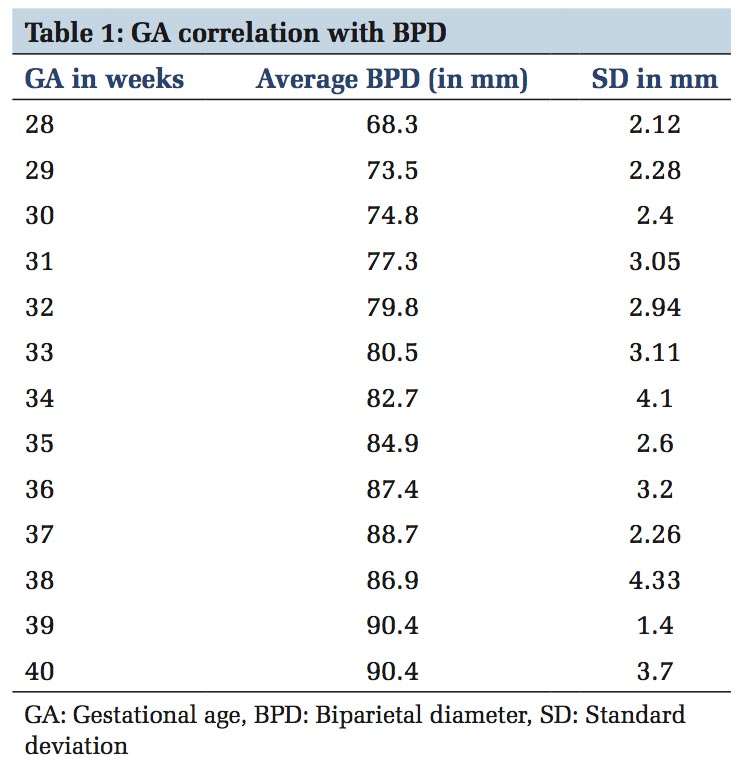
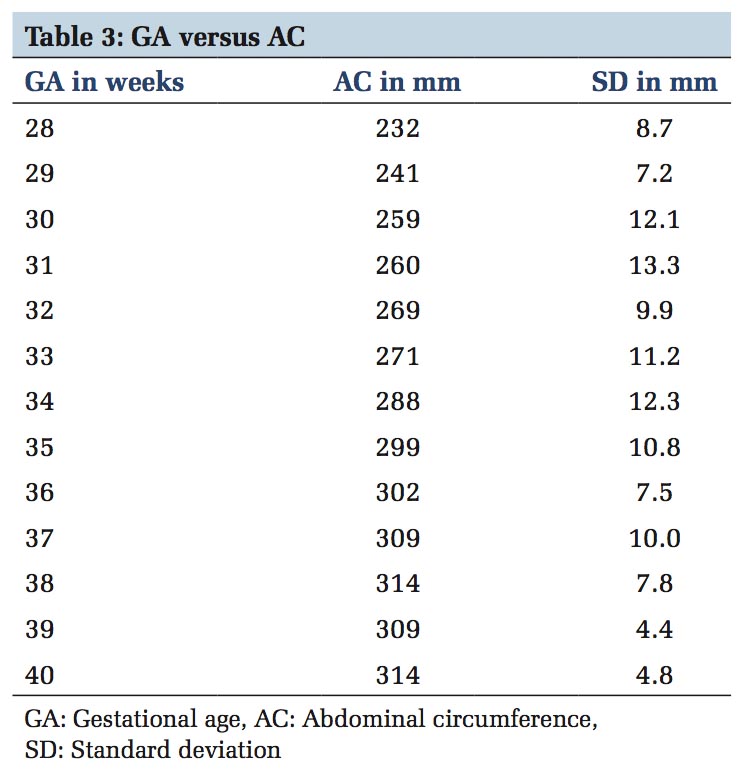
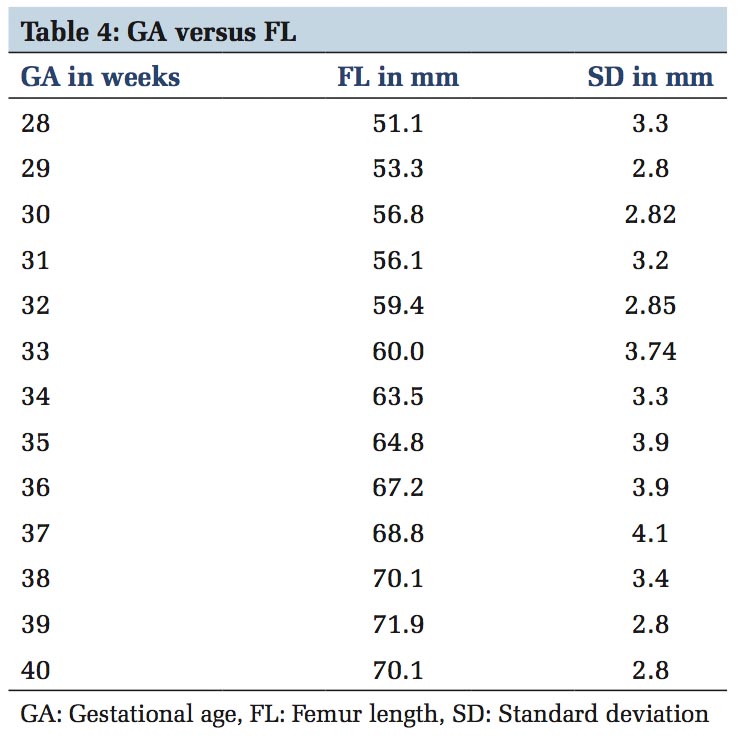
We first correlated BPD with GA using the Pearson’s correlation. Pearson’s correlation coefficient (R) came out to be 0.895 with a determination coefficient of 0.801 and the test was significant at P < 0.05 with a P < 0.00001 [Table 1]. Similarly, HC showed a Pearson’s correlation coefficient of 0.883 and AC showed the highest value among the conventional parameters with a R = 0.901 [Tables 2 and 3]. Finally, FL was correlated with a Pearson’s correlation coefficient of 0.879 [Table 4]. All the above tests were significant at P < 0.05.
In the present study, the FKL correlated with the GA with a correlation coefficient of 0.907 [Table 5] and a determination coefficient of 0.822 which was better than all the conventional parameters used [Table 6].
We found a very strong correlation between FKL and GA as compared to previous studies. The correlation coefficient (r = 0.907) observed in the present study was higher as compared to Cohen et al. (r = 0.82), Schlesinger et al. (r = 0.859), Gloor et al. (r = 0.90), Chiara et al. (for RK, r = 0.84, for LK, r = 0.87) and less than the studies performed by Konje et al. (r = 91) and Kaul et al. (r = 0.958).[1-6]
Finally, in the present study, an equation was found based on the regression coefficient; i.e., GA in weeks (Y) = 1.077*X (FKL in mm) −4.305
(Where slope m = 1.077 and constant = 4.305).


Sonographic measurement of fetal body parts is known as fetal biometry. There are three primary objectives for measuring fetal parts:[7]
The first trimester USG is a very useful and reproducible modality for the assessment of GA. Crown-rump length and mean gestational sac diameter are the two parameters for assessment of GA in the 1st trimester. Crown-rump length should never include the yolk sac and the extremities. It is useful from 8 weeks till 12 weeks of gestation.[7]
If GA has not already been established at a dating or first-trimester scan, it should be determined at the mid-trimester scan. Sonographic parameters that are used in the second and third-trimester pregnancy are as follows: BPD, HC, AC, or FL.[8,9] Combining measurements significantly improve accuracy compared with a prediction based on HC alone. However, the clinical significance of this improvement is marginal because the improved accuracy represents < 1 day.[10]
Rumack et al., in their textbook, mentioned that the kidneys grow throughout pregnancy and can provide a nomogram of renal lengths at 14–42weeks of gestation and the renal/AC ratio remains constant at 0.27–0.30 throughout pregnancy.[11]
USG is an accurate and useful modality for the assessment of GA in pregnancy and, as a routine part of prenatal care, can greatly impact obstetric management and improve antepartum care. From this study, we could find that the most accurate method for evaluation of GA was the KL followed by AC and BPD.
Kidneys are easy to identify and measure. Measuring KL can help in the determination of GA, especially in cases where the date of the mother’s last menstruation is unknown.
In addition to that, it could be a more valuable tool in cases where other established biometric indices are difficult to obtain and show gross discrepancies with each other or with GA.
Since classically the GA is still determined, in some places, by LMP, the chances of error increases, therefore the need for the use of USG investigation is highly recommended as the only measuring tools for GA determination. The present study emphasizes on the use of KL as the potentially accurate parameter for GA determination; we recommend, therefore, the use of KL to be included in the conventional methods for GA estimation.
Subscribe now for latest articles and news.