Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 1, Pages: 93-96
Case Report
Snehal Patil1 , Manoj Vedpathak2 , Sujata Dharmshale3 , Nasira Shaikh4
1Post Graduate Student, Department of Microbiology, Dr, V.M. Government Medical College, Solapur - 413003, India,
2Assistant Professor, Department of Microbiology, Dr, V.M. Government Medical College, Solapur - 413003, India,
3Associate Professor, Department of Microbiology, Dr, V.M. Government Medical College, Solapur - 413003, India,
4Associate Professor and Head, Department of Microbiology, Dr, V.M. Government Medical College, Solapur – 413003, India
Address for correspondence: Manoj Vedpathak, Assistant Professor, Department of Microbiology, Dr, V.M. Government Medical College, Solapur - 413003, India.
E-mail: [email protected]
Diphtheria is an acute infectious toxin mediated disease caused by Corynebacterium diphtheriae. Effective vaccination has decreased the incidence of disease globally. However, despite of a full-fledged Universal Immunization Programme, the cases are still seen in children and adolescents in many states in India. Here, we report three recent cases of diphtheria from Solapur district of Maharashtra to flag the awareness of the disease and importance of vaccination.
Keywords: Corynebacterium diphtheria, immunization, Diphtheria antitoxin
Diphtheria is a life threatening infectious disease caused by gram positive bacteria Corynebacterium diphtheriae. The disease spreads via air droplets from a case or carrier. In the pre-vaccination era, diphtheria was a leading cause of mortality in children.[1] However, the incidence of diphtheria decreased after introduction of diphtheria-tetanuspertussis (DTP) vaccine. In India the Expanded Programme of Immunization (EPI) was introduced by World Health Organization (WHO) in 1978 which led to the increased vaccination.[2]Despite this, India alone accounted for 83.3% of the global burden of Diphtheria in 2014.[3]
Here, we report three cases from West Maharashtra (Dec 2020-Jan 2021), suggesting of persistence and possible re-emergence of the disease.
Relevant demographic characteristics of all the three cases were assessed and analysed. This included age, sex, whether hospitalized, immunization and clinical history, other investigations, treatment and outcome. These all are mentioned in the Table 1.
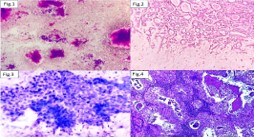
In all the above mentioned three cases, diagnosis of diphtheria was confirmed by microscopic examination and aerobic culture of throat swabs. For all the three cases, two throat swabs were sent for microscopic examination and aerobic culture, respectively. Microscopic examination of Gram stained smear revealed occasional gram-negative bacilli, pus cells and Gram positive bacilli with clubbed ends some of which were arranged in Chinese letter pattern like ‘L’ and ‘V’ suggestive of Corynebacterium diphtheriae. Microscopic examination of Albert stained smears showed green bacilli with dark blue metachromatic granules at their ends morphologically suggestive of Corynebacterium diphtheriae (Figure 1).
Blood, MacConkey, and Blood Potassium Tellurite (BPT) agar plates were respectively inoculated and incubated under aerobic conditions. Raised, Black colonies approximately 2–3mm in size were obtained on BPT agar after 48 hours of aerobic incubation (Figure 2). Gram and Albert stained smears were prepared from these colonies, which respectively revealed same findings as mentioned above
In all the three cases, patient’s household contacts were investigated. There were no diphtheria carriers nor outbreak in the community resulted from this patient.
Over the years, Diphtheria continues to be a public health problem in India. It is mainly a disease of the upper respiratory tract and spreads via air droplets from a case or carrier. Carriers are also important source of infection as the ratio is 95 carriers for 5 clinical cases.[3]The exotoxin produced by the bacterium may lead to the obstructive pseudomembrane formation extending into the airways. The disease can also produce other complications like myocarditis, often being the cause of mortality in many cases. Patients with more severe respiratory symptoms may commonly present with myocarditis.
Also myocarditis is present in 19–68% cases with diphtheria.[4]Hence, timely diagnosis helps prevent these fatal complications.
Detection of the potent exotoxin produced by toxigenic C. diphtheriae is considered as the definitive test.[5]However, in all the above mentioned three cases, strong clinical suspicion and microbiological examination (staining and culture) gave us final diagnosis.
Also, all three cases were notified to the hospital and state health authorities as per the Integrated Disease Surveillance Programme (IDSP) guidelines. Appropriate measures were also employed by Hospital Infection Control team in order to prevent a nosocomial outbreak of diphtheria as per Centres for Disease Control guidelines.[6]
Since diphtheria antitoxin (DAT) is the mainstay of treatment for the disease, its ready availability is also a major issue as studies have reported patient loss due to delay in availability of DAT.[6,7]But in our cases, we had ready availability of DAT and could manage patient quickly without further complications. Furthermore, early diagnosis is crucial in identifying early manifestations of faucial diphtheria, bacteraemia, and toxaemia, as initial treatment with penicillin can stop the disease progression.
In India, Under the Universal Immunization Programme, 3 doses of Diphtheria, Pertussis and Tetanus (DPT) vaccine starting at 6 weeks of age followed by 2 booster doses at 18 months and between 54 and 72 months of age are given. Despite this, India alone accounted for 83.3% of the global burden of Diphtheria in 2014.[3] As per the Central Bureau of Health Intelligence (CBHI) data, during 2005– 2014, India reported 41,672 cases (average: 4,167 per year) with 897 deaths (case fatality ratio: 2.2%).
Ten Indian states (Andhra Pradesh, Assam, Delhi, Gujarat, Haryana, Karnataka, Nagaland, Maharashtra, Rajasthan, and West Bengal) bore this burden.[8] Studies show that vaccination is highly effective at preventing symptomatic disease but it has no effect on preventing infection. Compared to symptomatic cases, asymptomatic infections still transmit infection but at the rate of only 24%.[9]According to the national level surveys, the coverage of three primary diphtheria vaccines ranged between 55.1% (1998–1999) and 78.4% (2015–2016). However, Diphtheria boosters is not included in the national level surveys.[8]
However, vaccination still remains a big challenge for India due to reasons like, lack of awareness of the disease among people, negligence by parents, rumours by certain faith groups that vaccines may lead to impotence and that these are “inventions” by westerners to destroy certain communities or leaders of some religious sects telling that vaccinating children as “personal choice of freedom”;[10]all these factors may lead to persistence of the disease in India in spite of the efforts of the government.
Our case series highlights the need of having a vigilant approach for clinical suspicion for diphtheria and timely microbiological diagnosis by laboratory confirmation of cases with membranous tonsillitis. Moreover, National surveillance of the disease is of paramount importance as it will provide with more data regarding new infections as wells as vaccination status which will further help in understanding the burden of diphtheria in India.
Adequate immunization with emphasis on taking booster doses along with awareness among physicians, early microbiological diagnosis, and widespread universal immunization can control the re-emergence of this infectious disease.



Subscribe now for latest articles and news.