Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.003
Year: 2021, Volume: 7, Issue: 2, Pages: 13-20
Original Article
Lipi Chakrabarty
Associate Professor, Department of Ophthalmology, C.C.M. Medical College, Durg, Chhattisgarh, India
Address for correspondence: Dr. Lipi Chakrabarty, Department of Ophthalmology, C.C.M. Medical College Kachandur, Durg - 490 024, Chhattisgarh, India. Phone: +91 75810 34325. E-mail: [email protected]
Objective: The objective of the study was to assess the level of glaucoma awareness, knowledge, and self-care practices among health-care professionals at a medical college in Central India.
Materials and Methods: A cross-sectional, questionnaire-based observational study was carried out at Durg, Chhattisgarh, India, over a period of 2 months from February 2019 to April 2019. The study included 166 consenting adult health-care professionals – clinicians (excluding ophthalmologists), non-clinical doctors, and paramedical staff. Responses to a structured questionnaire covering various aspects of glaucoma knowledge and selfpractice were obtained with a face-to-face interview. Data were reported and analyzed using descriptive statistics and Pearson’s Chi-square test.
Results: One hundred and fifty-four (93%) participants had heard of glaucoma. Of these, 12 members left the questionnaire incomplete and were excluded (response rate 92%). Mean age of respondents was 35 ± 9.81 years. Respondents included 42 clinicians, 48 non-clinical doctors, and 52 paramedical staff. The knowledge about association of glaucoma with raised intraocular pressure (81%) was better than optic nerve damage (64%). Majority of the participants had knowledge that increasing age (76%) and family history (76%) were risk factors for glaucoma. Most paramedics were mistaken of digital screen usage (P = 0.004), prolonged reading (P = 0.01), and stress (P = 0.012) causing glaucoma. About 25% thought that glaucoma is painful and 37% opined that central vision deteriorates earlier (P < 0.01). Only 19% had undertaken glaucoma screening for themselves.
Conclusion: The study revealed unsatisfactory knowledge and deficient self-care practices concerning glaucoma among healthcare personnel including clinicians. This highlights the need to sensitize all cadres of medical staff to promote knowledge of this irreversible disease activating timely screening and adequate management for preventive ophthalmic care.
KEY WORDS: Awareness, Central India, Glaucoma, Health-care professional, Knowledge, Questionnaire, Self-care practice.
Glaucoma is second only to cataract as the leading cause of preventable blindness in the world.[1] Published evidence indicates that late diagnosis of glaucoma is an important risk factor for subsequent blindness and is associated with poor knowledge about the condition.[2] The referral source is an important contributing factor for early diagnosis. Blindness due to glaucoma can be curbed to a certain extent by educating the masses about the condition and thereby influencing at risk individuals to participate in regular ophthalmic care.[3] Since glaucoma is associated with comorbidities such as hypertension, diabetes, and smoking, health-care professionals form an important link for patients with risk factors to be referred to the ophthalmologist for screening. Medical personnel are a trusted source of information and paramount in promoting health awareness.[4] Lack of awareness regarding glaucoma is an important reason for its late presentation, which significantly increases the risk of blindness. Due to the blinding natural course of the highly prevalent disease and the poor awareness of the disease in the population, there is a need for an efficient link between the population at risk and the ophthalmologist.[5]
Given that the outreach of health-care system in developing countries remains far from optimal, it is essential that each of the health-care provider be educated about glaucoma, so as to reach a large sector of the population, which does not have access to a comprehensive eye care center.[6,7] Albeit important, not much information is available on knowledge and self-care practices associated with glaucoma among hospital workers in India. This study was conducted to assess the awareness, knowledge, and self-care practices associated with glaucoma among health care workers employed in a medical college hospital in Central India.
This cross-sectional, descriptive, questionnairebased study was done over a period of 2 months from February 2019 to April 2019. The study was undertaken at a private medical college and 750-bedded hospital at Durg, Chhattisgarh in Central India. A convenience sample of 166 adult consenting participants of either gender was included. The sample comprised health-care professionals working in the medical college and understanding English/ Hindi language. Sample was grouped as: (1) The clinicians excluding ophthalmologists (defined as medical graduates who deal with the patients directly during the discharge of duties in the hospital include physicians, surgeons, and anesthesiologists), (2) non-clinical doctors (defined as a medical graduate who did not come in direct contact with the patients during their discharge of duties in the hospital such as anatomists, physiologists, and microbiologists), and (3) paramedical staff (defined as hospital staff with paramedical qualifications such as nursing staff, physiotherapists, and paramedical technicians)
Individuals were invited to participate in the study, with adequate time given to consider whether they wished to participate. One hundred and seventy-five staff members were approached. Written informed consent was obtained from 166 willing subjects. No incentive was provided to the participants. Since the questionnaire was in English and Hindi; adults able to speak and comprehend either of the languages were included in the study. Non-willing subjects and subjects with communication difficulties were excluded from the study. All participants were informed about the scope and purpose of the study. The study adhered to the tenets of the Declaration of Helsinki. Permission and ethical clearance was obtained from the Institutional Ethical Committee of the medical college where the study was conducted.
The study instrument used was a structured questionnaire designed by the investigator. Questionnaires previously used for similar study were referred.[5-11] The questionnaire was designed based on standard framework.[12,13] The questionnaire was developed in English and then translated into Hindi by a translator. Another translator backtranslated the translated version to English. The third translator compared the original and backtranslated versions and prepared the final draft.[14,15] The questionnaire was pilot tested on 30 consecutive, literate, non-glaucoma patients presenting to the ophthalmology outpatient department. Elements assessed in the pilot of the questionnaire included ability to comprehend the instructions in the covering letter, understanding of questionnaire items and the terms used, the sequence of questions and the flow of statements, the format, and the time taken to complete the questionnaire. Observations were taken into account and errors amended.
The questionnaire comprised 20 closed questions (15 questions on knowledge regarding glaucoma and 5 questions on self-care practices) with a list of possible responses. The participants were asked to check the box opposite the chosen response. The questionnaire was self-administered and participants were not allowed to take the questionnaire away. The participants were instructed to check item completion at submission which was double checked by the investigator.
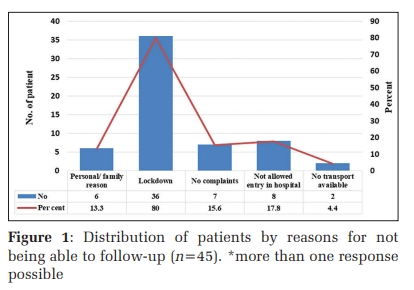
Having heard about the term glaucoma (Kalamotiya or Kaanchbindu in Hindi) was considered as awareness. Only those who were aware of glaucoma were required to complete the next section on knowledge of glaucoma. Knowledge assessed included etiology, risk factors, symptoms, treatment, and prevention of glaucoma. Only fully completed questionnaires were included in the analysis (Figure 1).
All data were coded, entered, and analyzed using Microsoft Excel 2010 and Epi Info 7 (7.2.2.6, Center for Disease Control and Prevention). Data were reported using descriptive statistics. The level of knowledge among the staff categories was compared using Pearson’s Chi-square test. P ≤ 0.05 was considered statistically significant.
Out of 166 participants, 154 (92.77%) participants had “heard of glaucoma.” The 12 subjects who were not aware of the term were all paramedical staffs. Out of the 154 subjects, 12 participants left the questionnaire incomplete and were excluded giving a response rate of 92.20%. Majority participants had heard of glaucoma during their course training.
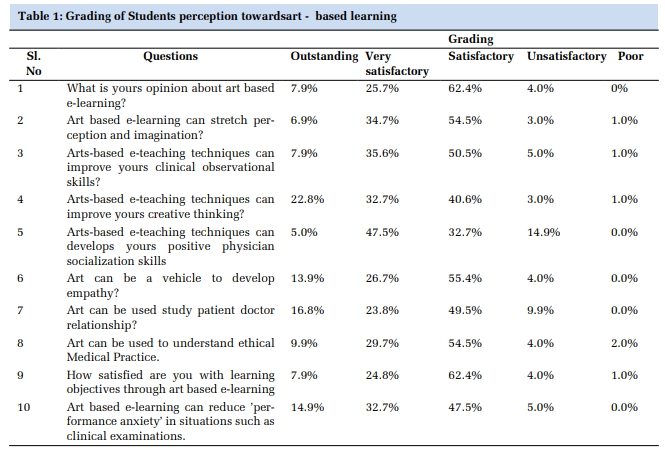
A total of 142 participants completed the questionnaire. Fifty-eight (40.85%) respondents were male while 84 (59.15%) were female, with a male-to-female ratio of 1:1.45. The mean age was 35 ± 9.81 years with age range being 26–64 years. There were 29.58% clinicians, 33.8% non-clinical doctors, and 36.62% paramedical staff (Table 1).
Most participants (81%) had the knowledge that glaucoma is associated with increased intraocular pressure (IOP). The fact of glaucoma causing optic neuropathy was lesser known to non-clinicians and paramedics (P = 0.011). Only 39% acknowledged that glaucoma can occur in eyes with normal IOP, the knowledge being poor across all the three groups (Table 2).
Majority (76%) had the knowledge that positive family history of glaucoma is a risk factor. Association of myopia with glaucoma was the least known (32%), with a significant difference across the three groups (P = 0.0007). The knowledge of corticosteroids as a risk factor for glaucoma was higher among clinicians (86%) than in non-clinicians and paramedics (Table 3). Major facts about the clinical features and course of glaucoma were found to be lesser known. Only 51% knew that glaucoma patients can be asymptomatic in the early stage of the disease and 68% knew that vision loss due to glaucoma is irreversible. About 37% of subjects were unaware that glaucoma generally affects peripheral side vision before central vision (Table 4).
In response to questions on factors that could worsen the progression of glaucoma, there was a significant difference in the response of the three groups with majority paramedics lacking knowledge of the enquired aspects (Table 5). In total, 31.69% of participants thought that prolonged digital screen use could make glaucoma worse while 14% of participants felt that lots of reading will worsen the progression of glaucoma.
About 78% of participants believed that screening for glaucoma should be done after the age of 40 years. Still, only 19% of subjects had visited ophthalmologist for self-screening (Figure 2). About 95% of subjects were willing to visit ophthalmologist regularly and continue treatment, if diagnosed with glaucoma. If surgery was the only treatment option available, then 74% were ready to undergo same promptly (Table 6).
In our study, 7% of the staffs were not aware of condition called glaucoma. In a similar study by Nageeb and Kulkarni[8] in South India, about 8% health professionals had not heard of the term, all of them being paramedical staff. In the present study too, the 12 subjects who were not aware were all paramedical staffs. In Padmajothi et al. [9] study at rural Karnataka, 95% were aware of glaucoma. In the survey among teaching hospital workers in Nigeria, 4.9% were not aware of the term.[6] In Onabolu and Bodunde[16] study of Nigeria, awareness was 97% among 181 primary health caregivers involved in the study. In other research studies in North India and Africa, almost all the health personnel were aware of the condition.[5-7,10] In Osaguona and Edema[11] study at Nigeria, involving hospital workers, 25.7% were not aware. These differences may be due to the selection criteria of the participants, their personal experiences in the subject of ophthalmology and individual intelligence. The high level of awareness among the medical doctors in these studies is not surprising as they are expected to have had lectures on glaucoma in the course of their training.
The knowledge about association of glaucoma with raised IOP (81%) was better than optic nerve damage (64%). These observations about awareness of high IOP are comparable with similar Indian studies.[7,8] In the work conducted by Komolafe in Africa, 88.3% of professionals knew that glaucoma was due to high pressure in the eye.[5] The knowledge about increased IOP being better than optic nerve damage has been reported by Ichhpujani et al. [7] (67.2% and 47.1%) and by Nageeb and Kulkarni[8] (82.4% and 32.4%). In the present study, about 67% of clinicians upheld that optic neuropathy in glaucoma may exist with normal IOP and merely 11.5% of paramedics knew this fact (P = 0.0008). This indicates that the general understanding about glaucoma, even among health professionals, is about its relation to the intraocular pressure and not to the optic nerve damage that results. The knowledge that glaucoma can occur in eyes with normal IOP was poor in our study even among clinicians. This points out that the understanding about the occurrence of glaucoma in the absence of raised IOP is not common to them. In one of the studies in India, it was noted that some of the glaucoma cases were missed by optometrists and ophthalmologists, possibly because a comprehensive eye examination was not performed.[17] Similar findings were observed in Barbados Eye Studies and England Eye Hospitals study.[18,19] In a study conducted by Van Zyl et al. [20] among general practitioners, only 53% of respondents considered the ability to diagnose glaucoma as important despite it being a major cause of irreversible blindness in the world. In the present study, most (94%) of the participants knew that glaucoma is a treatable disease. In Nageeb and Kulkarni[8] study, 96.4% of the participants affirmed the same.
There were major lacunae in knowledge on the clinical features of glaucoma. Majority thought that glaucoma is a painful disease (25%) and affects central vision earlier than peripheral vision (37%). Only half of the participants (51%) knew that early glaucoma can be asymptomatic. In Premnath et al. [10] study involving 319 doctors and medical interns, 12.7% thought it to be painful, 23.1% commented central vision to be affected first, and 18% of the participants thought that glaucoma is always symptomatic. In Onabolu and Bodunde[16] study in Nigeria, most of the respondents knew that glaucoma is caused by high pressure in the eyes, but nearly all thought that it is a painful disease. This is unfortunate since the painless nature of chronic open-angle glaucoma is one of the factors responsible for late presentation. The typical features of glaucoma make it a “silent thief of sight” and necessitate early diagnosis.[21] In glaucoma, central vision, which is what is used for testing visual acuity, can be preserved until the disease is advanced. It is, therefore, vital to realize that normal visual acuity does not exclude glaucoma.[22]
In the present study, only 68% of subjects acknowledged that blindness due to glaucoma is irreversible. In the study of Ichhpujani et al.,[7] about 61% of the interviewed knew the fact. In a study from Karnataka, 60% were aware of the irreversibility of vision and 41% knew that it will lead to blindness.[9] In the study from a university teaching hospital in Nigeria, involving majority of medical doctors and nurses, 48.8% of subjects did not know whether visual loss due to glaucoma was permanent or reversible.[6] These features of glaucoma need to be well known to the hospital professionals, since by the time, a patient is aware of vision loss, the disease is usually quite advanced.[23] Vision loss from glaucoma is not reversible with treatment, even with surgery.
The knowledge of diabetes, hypertension, and family history of glaucoma as risk factors for glaucoma was high, but the knowledge of corticosteroid (54%) and myopia (32%) as a risk factor was low. The knowledge of corticosteroids usage being a risk factor was high in clinicians (86%) than in non-clinicians (58%) and paramedical staff (23%). This is probably because clinicians use steroids in their practice and know of the adverse effects from medical school. In Nageeb and Kulkarni[8] study, 57% of participants knew about the propensity of steroids causing glaucoma. In Padmajothi et al. [9] survey involving medical and non-medical staff, only 28% knew that steroid instillation can cause glaucoma. In the study conducted in Africa, 31.7% thought family history to be a strong risk factor but 26.7% had no knowledge of risk factors for glaucoma.[5]
In this study, many paramedics believed that digital screen usage, prolonged reading, and stress may trigger glaucoma. This difference in opinion was clinically significant for the paramedical staff. In Premnath et al. [10] study involving doctors, 13.3% thought that stress and 10.4% opined that prolonged computer viewing will worsen glaucoma which is contrary to the fact. This agrees to our study wherein 10% of doctors (clinicians and non-clinicians) associated stress and 18% associated digital screen usage with glaucoma. Most health workers know about digital eye strain and computer vision syndrome. Knowing this, they might have associated digital screen with eye disease like glaucoma too. Again, the responses may be a reflection of the limitations of closed-ended structured questionnaire, wherein respondents may be biased into giving a certain response.
Despite working in a hospital with easy access to health care, only 19% have undergone screening for glaucoma. In Nageeb and Kulkarni[8] quest, 15.7% had undergone screening. In Ichhpujani et al. [7] study, 42% had visited ophthalmologist in the past 1 year. Premnath et al. [10] marked that 16% of the medical doctors had never undergone an eye check-up. In Adegbehingbe and Bisiriyu[6] survey, 41.5% had not seen an optometrist or ophthalmologist in the past year. These differences in the cited figures may be because in the present study, and in Nageeb and Kulkarni[8] questionnaire, the question pertained specifically to screening of glaucoma. In other mentioned studies, the question focused on last visit to an ophthalmologist. Among the participants, only 23% of the family members were screened. This is comparable to Nageeb and Kulkarni[8] study where 19.2% of family members were reportedly checked for glaucoma. In Ichhpujani et al. [7] survey, almost one in four doctors and nurses did not realize that it is important to screen family members of glaucoma patients for the disease, since they have a higher risk of having glaucoma. There are barriers to seek medical health care which may be due to the low knowledge and lack of clear understanding about the disease.
The low level of knowledge could be a result of the low interest these participants had in ophthalmology while in training, as this information is generally gathered from curriculum. In a study at a medical college in South India undertaken to assess the adequacy of ophthalmology teaching in undergraduate medical education, only 54.5% reported an adequate level of comfort in Schiotz tonometry. This was mentioned as an area of concern because glaucoma contributes majorly to the burden of blindness in India.[24] In his publication, Jha concluded that undergraduate teaching of ophthalmology in India requires reorientation and reconfiguration.[25] Another factor that could explain the paucity of knowledge is the interval between graduation and the time the questionnaire was administered.
About 95% of subjects were willing to visit ophthalmologist regularly and continue treatment, if diagnosed with glaucoma. This is unlike Ichhpujani analysis, where reluctance to visit ophthalmologist and the use of medication were reported by more than 20% of subjects.[7] If surgery was the only treatment option available, then 74% were ready to undergo same promptly as compared to 87% in Ichhpujani et al. [7] research.
Being a private medical college hospital-based and questionnaire-based design, the study has associated limitations. While a fair sample size and three well-defined and equally distributed study groups contribute to the study, the study cohort may not be representative of general hospital community. Since our observations are from a single center, generalization of results is limited. The medical and paramedical staff of tertiary institutes or of hospitals holding frequent educative programs might differ in awareness and knowledge. The presence of glaucoma in participants or their acquaintances has not been taken as an exclusion criterion in the study. Diagnosed glaucoma subjects could have had better knowledge of the disease. We have tried to minimize interviewer and response bias by effective designing and administration of questionnaire. Adequate response rate of 92% helped in data quality. There are limited publications exploring the knowledge and selfpractices of hospital health workers as concerned with glaucoma worldwide and to date, no published data on this specific issue in Central India, as per author’s knowledge. The data derived from this study reflect the lack of knowledge about glaucoma and perturbing self-care practices. In Van Zyl et al. study, responding general practitioners felt that there is a need for ophthalmology upskilling courses and 99.9% of them would attend such courses.[20] This announces the need for glaucoma education for health workers.


It was found that being a hospital worker did not translate into being knowledgeable about glaucoma. In India, paramedical workers are closer to the people at primary level and are often the first point of contact. All doctors also need to have not only the right knowledge about glaucoma but also carry positive healthseeking behavior toward it, so as to be able to advise others appropriately. To conclude, there is unsatisfactory knowledge and deficient self-care practices concerning glaucoma among health professionals. Glaucoma education needs to be emphasized among the medical staff and in the community outreach programs.
Subscribe now for latest articles and news.