Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2022.v8i1.37
Year: 2022, Volume: 8, Issue: 1, Pages: 22-27
Original Article
Vimal Agrawal1 , H G Ravikiran2 , M S Santhosh3 , C Vijay2 , B S Prashasth1 , Avinash Chandra4
1Senior Resident, Department of Orthopedics, JSS Medical College and Hospital, Mysuru -570004, Karnataka, India, 2Associate Professor, Department of Orthopedics, JSS Medical College and Hospital, Mysuru - 570004, Karnataka, India, 3Assistant Professor, Department of Orthopedics, JSS Medical College and Hospital, Mysuru - 570004, Karnataka, India,
4Post Graduate, Department of Orthopedics, JSS Medical College and Hospital, Mysuru -570004, Karnataka, India
Address for correspondence: C Vijay, Associate Professor, Department of Orthopedics, JSS Medical College and Hospital, Mysuru - 570004, Karnataka, India. E-mail: [email protected]
Introduction: Arthroscopic ACL reconstruction is one of the most successful surgeries in sports medicine. But the donor site morbidities have been reported with bone patellar tendon bone graft and hamstring tendon graft. The objective of the study is to evaluate the functional outcome of and donor site (ankle) morbidities with full thickness peroneus longus tendon (PLT) autograft in arthroscopic anterior cruciate ligament (ACL) reconstruction. Methods: A Prospective study was done in 30 patients with ACL injury. Knee stability and function were evaluated using the Lachman test, pivot shift test, International Knee Documentation Committee score (IKDC) and Lysholm knee score. Donor ankle was assessed using American Orthopedic Foot and Ankle Score (AOFAS) and grading muscle power by Medical Research Council scale. Data collected preoperatively and postoperatively at 6 & 12 months were compared. Results: The IKDC score was normal or nearly normal in 24 patients and abnormal in 6 patients. The mean Lysholm score had excellent or good results in 24 patients. The Lachman test showed normal findings in 24 patients, 6 patients had 1+ laxity. The pivot-shift test was negative in 22 patients and 8 patients had 1+ glide. The mean AOFAS score was 100±0.0 (preoperatively) and 96.0±9.6 (at final follow up). No patient experienced ankle pain and instability. Conclusion: PLT autograft gave painless stable knee, with a good range of motion. It didn’t have any morbid effect on ankle and gait parameters. So, PLT autograft can be suitable graft with respect to its strength, safety and donor site morbidity.
Keywords: ACL, Peroneus Longus Tendon, Knee Arthroscopy
Anterior Cruciate Ligament tears represent more than 50% of knee injuries and ACL reconstruction has traditionally been recommended for the restoration of anterior-posterior as well as rotatory knee laxity.[1] Bone-patellar tendon-bone (BPTB) complex and hamstring tendon (HT) autograft are commonly used
as the graft source. A Meta-analysis conducted in 2015 failed to conclude which among them is a better autograft.[2] Donor site morbidities have been reported following the harvest of graft from the knee region (bone patellar tendon bone and hamstring tendon autograft) which includes patellar tendon rupture, patellar/tibial fracture, loss of knee full extension, anterior knee pain, difficulty in harvesting graft, unpredictable graft size and a potential decrease in hamstring power.[3] Given the hostile side effects of using these grafts, another alternative autograft should be sought that meets the demands of kneeling along with optimal strength and minimal donor site morbidity. There is precedent in the literature suggesting peroneus longus tendon (PLT) as an alternative autograft for ACL reconstruction.[4] Therefore, nowadays some orthopedic surgeons are using PLT as an autograft for ACL reconstruction. Some previous studies have reported that PLT can be considered as the first option for an arthroscopic ACL reconstruction with good clinical outcomes and very less donor ankle morbidity.[5] While other studies could not recommend it, because of donor ankle morbidity.[6] The advantages are its strength and mean thickness is nearly the same as that of the native ACL and is very easy to harvest but there are very few studies in the literature concerning the acceptability of PLT autograft as a source for ACL reconstruction. Hence, our study aims to evaluate the functional outcome and donor site morbidity after harvesting PLT graft for ACL reconstruction.
This is a prospective interventional study conducted in the Department of Orthopedics, JSS Hospital, JSSAHER, Mysuru for a period of one year from October 2017 to September 2018 after obtaining Institutional Ethical Committee Clearance and the Study population were all the patients with ACL tears who underwent arthroscopic ACL reconstruction using ipsilateral Full thickness PLT autograft. The inclusion criteria were all the patients of the age 18 years to 50 years old with Clinical instability and MRI proved ACL insufficiency associated with or without medial or lateral meniscal tear with the presence of peroneus longus graft with eversion power equal to or more than 4 on grading by Medical Research Council (MRC) on the same side of injury. Exclusion criteria was ACL rupture associated with a tibial or femoral fracture or avulsion injuries, Illnesses that prevent them from ambulating normally, patients with a significant ankle injury or instability, Posterior cruciate ligament laxity/ injury, Postero-lateral Complex injury, patients with associated medial collateral or lateral collateral ligament injury (Grade III), and patients with a history of previous surgery in the affected knee.
A total of 30 patients were enrolled in the study and followed up for 6months and 1 year.
Clinical and subjective evaluation of the ankle was done using American Orthopedic Foot and Ankle Society Score (AOFAS) and grading peroneus longus muscle power (Eversion & Plantar flexion) by Medical Research Council (MRC) Scale.
Clinical and Subjective evaluation was done preoperatively and postoperatively at 6 months and 12 months and scores were compared.
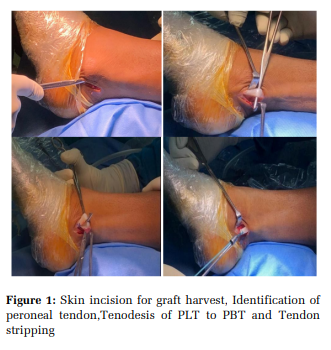
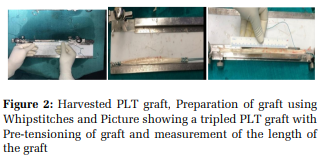
ACL reconstruction using ipsilateral PLT autograft was performed by a single senior knee surgeon. The patient is placed in supine position under spinal anesthesia. If preoperative examination reveals considerable knee laxity, PLT graft harvesting is done straight away. If ligament laxity is not significant, diagnostic arthroscopy was done before proceeding with the graft harvest. The Full thickness PLT Graft was harvested using an incision of about 2 cm long and this longitudinal incision is given 2 cm above and 1 cm behind to the posterior prominence of lateral malleolus just above the superior peroneal retinaculum of the ipsilateral limb (Figure 1). Subcutaneous tissues, superficial and deep fascia is incised and dissected to expose the peroneus longus and peroneus brevis tendon, taking care not to injure the sural nerve. (Figure 2). PLT and PBT are levered out of the skin window. Tenodesis of PLT to PBT is done using absorbable suture (vicryl). (Figure 3). Heavy nonabsorbable Krackow stitches are placed on the PLT (Ethibond 5) and cut with a scalpel with curved artery forceps, the PLT is separated from the surrounding soft tissues. The tendon is harvested proximally using a long tendon stripper by controlled tension while advancing a stripper proximally to about 4-5cms from the fibular head to prevent peroneal nerve injury. Subcutaneous tissues and fascia are closed in layers. Skin is closed using staples/ ethilon 2.0. Graft preparation (Figure 2) was done by separating the muscle fibers from the tendon with a no. 10 blade. Krackow-type whip stitches are placed on both ends of each tendon with no. 2 non absorbable sutures. The graft may be doubled, tripled or quadrupled depending on the length and diameter of graft obtained. The femoral and tibial tunnels were prepared. After drilling the tunnel, we proceeded with the implantation of the tendon with the graft fixation on the femoral side with an endo button and graft fixation on the tibial side with a bioabsorbable screw. The post-operative protocol is by applying Jones compression bandage,crepe bandage and ROM knee brace were applied immediately after the operation. Broad-spectrum IV antibiotics were given for 2 days. Dressings were done on the 2nd, 5th and 10th postoperative days. Patients were encouraged to do partial weightbearing with ROM knee brace 2nd postoperative day onwards (in case of isolated ACL reconstruction). Physiotherapy was taught according to the American Association of Orthopedic Surgery (AAOS) ACL reconstruction postoperative rehabilitation protocol. The objective and subjective evaluation were done as mentioned below.
Statistical analysis was done by using SPSS (Statistical Package for Social Science) software (Version 24.0). Comparison of preoperative data and postoperative data was done using Paired Student t-test and Chi-square test for inferential statistics. Mean, Standard deviation, Frequency and Percentages were used for Descriptive statistics. P-value of < 0.05 was considered statistically significant.
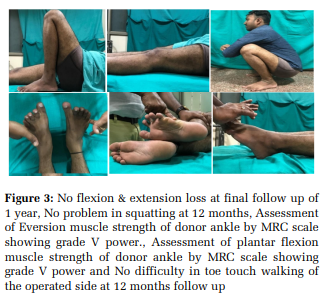
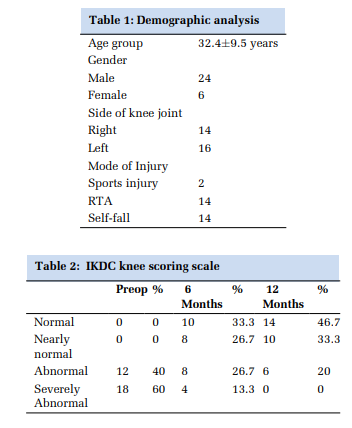
Demographic analysis of study is shown in Table 1. ACL reconstruction was performed by a single senior arthroscopic surgeon using the same harvest and graft technique. The study revealed a significant increase in Lysholm and IKDC score (p<0.0001) postsurgery compared to pre-operative values (Table 1 & Table 2). Stability of the ACL was assessed by the Lachman test, which showed normal findings in 24 patients, while 6 patients had 1+ anteroposterior laxity. The pivot-shift test was negative in 22 patients and 8 patients had 1+ pivot glide. There was no flexion or extension loss of the knee at the end of 12 months of follow up (Figure 8, 9). Mean pre and post-operative AOFAS scores were 100±0.0 and 96.80±3.36 respectively at final follow up (Table 3). The score indicates no subsequent instability noted at the donor site. No patient experienced ankle joint dysfunction or difficulty in sports activities due to PLT graft transfer (Table 4). However early superficial infection of the graft harvest site was present in 1 case at 3 weeks which delayed wound healing, for which debridement and re-suturing was done. There was no deep infection.
Anterior cruciate ligament (ACL) reconstruction is performed using different grafts. Allografts, autografts and synthetic grafts have been used with variable success rates. Currently, the hamstring and the bone patella bone tendon grafts are the forerunners among the autografts with wide acceptability. Tensile characteristics of these grafts are shown to be superior (maximum loads of 2977 N for BPTB and 4140 N for quadrupled HT) to the native femur-ACL-tibia complex (2160 N) with similar stiffness.[7] Although these grafts are used commonly, disagreements regarding suitable graft choice still persist because of some hindrances. Certain complications have been reported after harvesting BPTB and HT autograft. The most widely used BPTB autograft is associated with complaints of anterior knee pain and kneeling pain postoperatively.[8] A meta-analysis of studies has shown an increased incidence of osteoarthritis in a BPTB autograft ACL reconstruction of knee.[9] On considering autograft of hamstring, there was an electromechanical delay in knee flexors/weakness.[10] Harvesting HT may be deleterious in postoperative rehabilitation of ACL reconstruction as HT protects the reconstructed ACL from anterior drawer force, which is exerted by the quadriceps.[11] It might also hinder active knee flexion.[12] The other autografts are the peroneus longus tendon, quadriceps tendon, fascia lata etc. The use of peroneus longus tendon (PLT) autograft as an alternative to the conventional autograft is a recent development in the field of ACL reconstruction. In a recent study by Shi et al., it was found that the ultimate tensile strengths of doubled PLT, quadrupled HT, and native ACL were 4,268 ± 285, 4,090 ± 265, and 2,020 ± 264 N, respectively.[13] The advantages of doubled PLT graft is that its strength and mean thickness is nearly the same as that of the native ACL making it a strong contender for ACL reconstruction.[14] For these reasons, we used the peroneus longus tendon for ACL reconstruction in our patients. The peroneus longus tendon autograft showed an excellent functional outcome with no significant donor site morbidity.
6 patients reported mild knee pain while doing heavy physical work, running and squatting. No patient had developed fixed flexion deformity of knee or extension lag at 1 year follow up. The mean ROM of the knee was 136±4.71 (Range 0-140 degrees) at the final follow up. Kerimoglu et al published the results of 29 patients who had undergone ACL reconstruction by a PLT autograft. The results were assessed according to the IKDC ligament evaluation system and the Lysholm score system at the end of at least 5 years.[5] A similar study was conducted by B. L. Khajotia et al, in which 25 patients underwent arthroscopic ACL reconstruction by PLT autograft, evaluated the functional outcome of the knee using the IKDC scoring system at the end of 6 months. The results of these studies are compared with our study are depicted in Table 5 [15] . In above mentioned both the studies, a satisfactory outcome was present in 84% & 58.6% respectively and it is 80% in our study. Results in our study were consistent with the findings of the study done by B. L. Khajotia et al, while outcomes were better than the study conducted by Kerimoglu et al.
Assessments of the functions of the donor ankle after harvesting PLT autografts was done using the AOFAS score and by grading the power of the peroneus longus muscle particularly the eversion and plantar flexion movement by MRC scale. Mean AOFAS scores at preoperative and postoperative at 12 months were 100±0.0 and 96.80±3.36 respectively. There was no significant difference between preop and 12 months post-op AOFAS score, which suggests that harvesting PLT autograft did not affect ankle functions and ankle functions were grossly preserved. The examination of eversion power was graded V in 26 (86.67%) patients, while 4 (13.33.%) patients had grade IV power and on plantar flexion 28(93.33%) patients had grade V power and 2(6.66%) patient had grade IV power as per MRC scale muscle grading. Figure 10, 11 No patients had difficulty in sports activities and ankle joint and foot dysfunction due to transplant harvest abnormality. Functions of the ankle were preserved in all the patients. Results of AOFAS score and muscle power of the foot by MRC scale showed excellent results at 12 months follow up.
1 patient had developed superficial infection over the graft harvest site at 3 weeks post-surgery, for which debridement and re-suturing was done. No paresthesia, numbness or ROM limitation or any other discomfort or difficulty noted over the donor site of the ankle. The results of donor site (ankle) morbidity after harvesting ipsilateral PLT autograft of Angthong et al[6] and Sholahuddin Rhatomy et al[16] were compared to our study. Table 6 Even though the previous study by Angthong et al have observed a significant reduction in peak torque eversion and inversion strength of donor ankle, results in our study and study done by Sholahuddin Rhatomy et al showed that the functions of donor ankle and foot were still excellent and preserved after harvesting the PLT autograft. Based on overall findings in the present study we found that ACL reconstruction using ipsilateral PLT autograft produces excellent functional score without compromising ankle functions.
Limitations include evaluation of the donor ankle morbidity was done by grading of peroneus longus muscle power by MRC scale. The ligament laxity was assessed clinically, and not measured with the help of an arthrometer. The relatively small sample size and duration of the study of the ankle morbidity is one of the drawbacks of this study but the same samples and along with the new samples are under study for a long term morbidity results. Ankle morbidity assessment for two year follow up is more applicable in fracture management around the ankle joint and more so in geriatric patients, but in our study many belong to the younger age group and graft harvested from the normal ankle joint. There was no control group in the study.
This study showed that the Full thickness PLT autograft gives a painless stable knee postoperatively, with a good range of motion and increased quality of life and it did not have any contrary effects on ankle and gait. The results in our study showed that Full thickness PLT can be considered as a promising alternative for ACL reconstruction in an attempt to avoid potential donor site morbidities of harvested autograft (hamstring and BPTB graft) from the knee region.


Subscribe now for latest articles and news.