Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.005
Year: 2021, Volume: 7, Issue: 2, Pages: 27-33
Original Article
Manabendra Baidya1 , Sandeep Pandey2 , Yogesh Yadav3 , Satendra Kumar4 , Hariom Kumar Solanki5
1 Assistant Professor, Department of Surgery, Government Institute of Medical Sciences, Greater Noida, Uttar Pradesh, India,
2 Assistant Professor, Department of Dentistry, Government Institute of Medical Sciences, Greater Noida, Uttar Pradesh, India,
3 Senior Resident, Department of Surgery, Government Institute of Medical Sciences, Greater Noida, Uttar Pradesh, India,
4 Professor, Department of Surgery, Government Institute of Medical Sciences, Greater Noida, Uttar Pradesh, India,
5 Assistant Professor, Department of Community Medicine, Government Institute of Medical Sciences, Greater Noida, Uttar Pradesh, India Address for correspondence: Dr. Hariom Kumar Solanki, Department of Community Medicine, Government Institute of Medical Sciences, Greater Noida, Uttar Pradesh - 201 310, India. Phone: +91-09968215493. E-mail: [email protected]
Introduction: Like elsewhere Government in India took some drastic steps including nationwide lockdown, conversion of fully functional hospitals into coronavirus infectious disease (COVID) facilities to address the COVID 19 pandemic. As the impact of these measures on surgical patients is little studied in India, this study was undertaken to evaluate and assess the hardships of surgical patients at a teaching hospital in Northern India.
Materials and Methods: This study included all patients who got discharged from surgery ward at the study site in March 2020. For data collection patients were contacted telephonically and a pretested semi-structured questionnaire was used to assess the logistic, financial and healthcare related concerns/barriers these patients experienced after their discharge in seeking medical care and anxiety levels related to their health and lockdown at the time of interview.
Results: We could contact 63 patients out of maximum possible 85 patients (Response rate = 74.1%). A total of 26 patients (41.3%) visited health-care facilities other than the study hospital amounting to a total of 44 visits. Only 14 participants (53.8%) faced no difficulty whereas 12 (46.2%) experienced at least some difficulty in visiting these facilities/providers to receive health care. Almost all of them (23 participants, 88.5%) had to spend more time while over two fifth (11 participants, 42.3%) reported of spending more money than usual during these visits. Over a third (20 patients, 38.5%) experienced at least some anxiety while almost half of them (48.1%) were stressed more than usual with a significant 7.7% participants experiencing severe stress.
Conclusion: There was hardship experienced by significant number of surgical patients during the initial lockdown phases in India. We recommend more research – both qualitative and quantitative – to better establish the impact of stringent measures on care of surgical patients.
KEY WORDS: Anxiety, coronavirus infectious disease-19, hardship, lockdown, stress, surgical care.
World has seen many pandemics before, let it be Spanish flu (1918–1920) or H1N1 Swine Flu pandemic (2009–2010) but coronavirus pandemic is different from others because of its rapid transmission and severity of disease.[1] Due to the advancement in transportation, this virus spread to almost every country,[2] In a short period of time which forced many governments to take tough measures to control and restrict the spread of the virus. Some of the decisions being complete nationwide lockdown,[3] conversion of fully fledged working hospitals into coronavirus infectious disease (COVID) care facilities to accommodate the huge inflow of COVID positive patients among which a section of patients also required advanced critical ICU care.[4,5] This pandemic was also different in a way that due to nationwide lockdown many patients who were in need of medical care were unable to visit hospitals for their problems.[6] In addition majority of hospitals also closed their outpatient departments (OPD) to avoid gatherings and transmission of virus. At many places elective/non-emergency surgeries were also postponed indefinitely.[7] As a result of which a lot of patients including surgical patients, could not seek or were deprived of the medical care.
This study was done at a government medical college in Northern India where strict lockdown was imposed in March 2020 and there was sudden closure of OPD and operation theaters on administrative orders with aim of controlling and restricting the coronavirus pandemic. As a result surgical patients who were discharged in the month of March might have faced difficulty in their postoperative follow-up and also some of these patients were deprived of surgery. Authors of this study have tried to assess and evaluate the hardships faced by these surgical patients (logistically, financially, and in accessing health care) post their discharge from the study hospital.
This was a cross-sectional study conducted at a newly established government medical college in Northern India. Approvals for this study were taken from the institutional scientific research committee and the institutional ethical committee before data collection for this study. Inclusion criteria for this study included those in-patients who were admitted in the surgery department in the month of March 2020. All the relevant files were retrieved from the medical record section and the telephone numbers of all these patients were retrieved and compiled. A semi-structured questionnaire was used to enquire about the logistic, financial, and healthcare related concerns/problems/barriers these patients faced post their discharge from the study hospital in seeking further medical care. The study also included the generalized anxiety disorder-7 questionnaire to assess the anxiety level of the study participants. A simple question asking whether study participants experienced more stress than usual and if so degree of stress was also included in the questionnaire based interview schedule. The assessment of anxiety, stress, and difficulty faced in routine life and activities was done only for participants who were the patients discharged from the study hospital. If the informant was care giver these were excluded from the final data analysis. Those patients whose phone number was not available, those who were called but did not picked up phone at least 3 times on different days and time and those who did not gave consent to carry on the telephonic interview were excluded from the study. We also excluded patient who left against medical advice or absconded from the study hospital. All the patients were called and interviewed by the single interviewer. Patients were informed about the study and its purpose in their own language (vernacular language – Hindi) and only after obtaining verbal consent and explaining them the results of this study will be published online the patient was interviewed further. All the data collected were compiled in Microsoft excel sheet and were analyzed using EpiInfo 7.2 software.
There were a total of 98 patient records from the surgery department with the medical records section of the study hospital who got discharged on or after March 1, 2020, from department of General Surgery, out of which five patients had absconded, another eight patients left against medical advice and 23 patients could not be contacted and hence excluded from the study. Overall 63 study participants contacted telephonically agreed to a full interview and were included in the study (Response rate of 74.1%). Among these, 26 (41.3%) were females and 37 (58.7)% were males, the average age of females was 35.3 years and for males it was 38.6 years in our study. Five patients in our study were below 18 years of age. Over four-fifth (82.5%) of the study participants provided the information for the study themselves. However, in rest 11 patients (17.5%) informer was the primary caregiver of the patient from his/her family. Among study participants, 52 (82.5%) had an indication for surgery, of which 42 (80.8%) underwent surgery (35 major and seven minor surgeries), surgery of four patients was postponed due to ongoing COVID-19 pandemic, another four patients refused surgery after admission and surgery of two patients was deferred due to associated medical conditions. About a sixth of study participants (17.5%, 11 patient) were managed conservatively. Almost all the patients – 61 patients (96.8%) were advised follow-up visits at the time of discharge, of which 45 patients were due for their follow-up when lockdown came into force (28 patients had 1 follow-up due, 15 patients had two follow-up due, and two patients had three or more follow-up due). Just over one fourth – 16 patients (25.4%) had completed all of their follow-ups. The reasons due to which study participants were not able to do the advised follow-up are described in Figure 1.
Regardless of problems, 26 patients visited other health-care facilities (other than the study hospital) amounting to a total of 44 visits, receiving different treatments details of which are listed in Table 1. Out of these 26 study participants who visited other health-care facilities, 14 (53.8%) faced no difficulty in visiting the health facility whereas 12 (46.2%) had at least some difficulty in visiting the health facilities where they went for treatment or follow-up during lockdown. A total of 22 visits to different health-care providers/health facilities were made by these 12 patients who faced difficulty. In five of these visits patient was not satisfied or not relieved of their problems. Over two-third of these patient (69.2%, 18 patients) were not able to see/consult an appropriate specialist, that is, general surgeon, while rest eight patients (30.8%) were able to consult a general surgeon.
Almost all these study participants (23 participants, 88.5%) had to spend more time for visiting a healthcare provider or health facility during the lockdown period while over two fifth (11 participants, 42.3%) reported of spending more money than usual during their visits to seek healthcare [Figure 2].
Out of 63 study participants, over two fifth (28 patients, 44.4%) reported to have delayed seeking health care. The reasons of delayed seeking health care are tabulated in Table 2. Another 17 study participants (27.0%) reported deterioration in their health condition during the lockdown period. About a third study participants (20 patients, 31.7%) had a feeling of helplessness related to their health condition due to various reasons listed in Table 2.
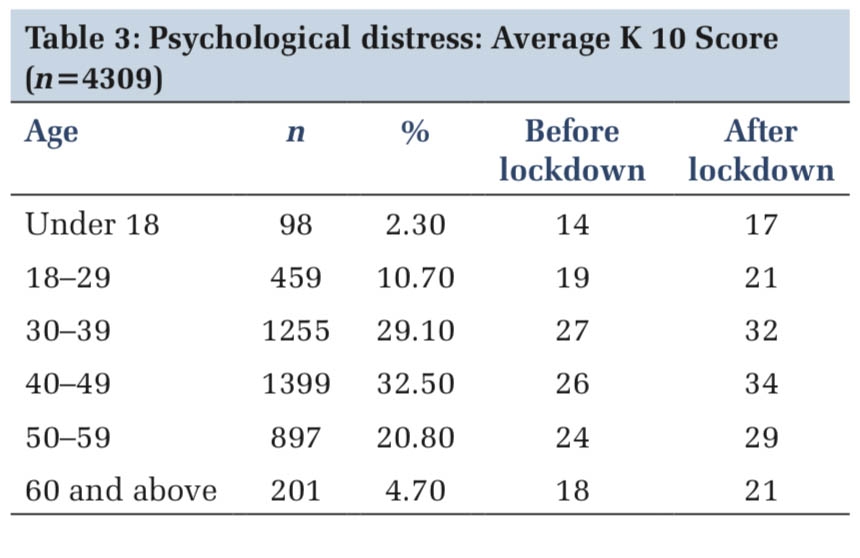
The stress experienced and the anxiety levels of the study participants during this lockdown period are summarized in Table 3. Over a third of the study participants (20 patients, 38.5%) experienced at least some anxiety while almost half of them (48.1%) were stressed more than usual with a significant 7.7% participants experiencing severe stress. A total of 40 study participants out of 52 eligible participants (76.9%) reportedly faced no difficulty at all, in their routine life and activities, for 18 study participants (34.6%) it was somewhat difficult and five study participants (9.6%) reported that they found carrying out routine life and daily activities very difficult. Details are described in Table 3. could not visit the study hospital because of the lockdown and conversion of study hospital into a COVID facility.
COVID-19 pandemic was an unexpected event for all which spread at unprecedented rate for a pandemic throughout the globe. The situation of lockdown was new to everybody including the governments, healthcare professionals, and the general populations. The gravity of the unfolding situation and possible health and economic repercussions forced the Indian governments to take some tough decisions one of which was the nationwide lockdown.[4,8] As per the directives of authorities, in the later part of the month of March 2020 elective surgeries were put on hold or cancelled and OPD were closed in view of spreading of coronavirus infection at the study health facility.[5,9] The idea behind closure of elective surgeries was to keep as many as hospital beds and ventilators free to meet the rising demands of COVID cases and also to divert the manpower and logistics toward COVID care.[10] The tertiary care hospital to which the authors belong was converted to a full-fledged COVID facility. Despite understanding the need of such measures and by en large cooperating with the government orders, many people including surgical patients, faced many difficulties to assess offline health services as a result of lockdown.[11] Although transport regarding medical or healthcare were allowed,[12] still there was a lot of stigma and fear within people related to COVID-19 and people were reluctant or unable to visit hospitals for their health needs.[13] Lockdown has also affected surgical patients like any other non-COVID patients. While most of the focus and concern was over COVID related symptoms, surgical patients got lower priority and occasionally got totally neglected. Either their surgeries were cancelled and postponed[14] or the patients faced difficulties in their post-operative period. Despite of all the hindrances and obstacles posed by this pandemic, this section of patients requiring surgery or undergone surgery have to be taken into considerations and solutions are to be made to address these problems.
In our study, we report that large proportion/number of patients (71.2%) who got discharged from health facility weeks before the lockdown came into force were not able to complete their follow-ups for reasons beyond their control. In spite of the fact that health related travel was allowed people could not come or did not came for follow-up due to stigma/ fear of Covid-19 or because the facility was no more catering to non-COVID patients. Post-operative follow-up is very much essential from the health point of view of patient as well as for the treating surgeon to track progress of the patient.
Over two fifth patients (41.3%) post their discharges from study hospital had to visit other health facilities for care. Most of these (53.8%, 14 patients) preferred to visit a local practitioner nearby (traditional practitioner, village practitioner, and quack). As the government was totally focused on the prevention, treatment and management of COVID 19 cases, and most facilities providing COVID care in the initial lockdowns were public health facilities, this group of patients got somewhat neglected in government set ups. Both fear and stigma of COVID 19 and restrictions like lockdown also played a significant role in it.[13] We report that only a small section of patients who required surgical intervention could get their surgery done during this lockdown period. Many of them still waiting (at the end of data collection in September end) to get operated.
Nearly half of the patients (46.1%, 12 patients) who visited outside facilities (total 22 visit) faced one or other significant problem. Over two-fifth visits (09 visits, 41%) compelled participant to spent more than usual money on consultation and purchase of medicine than she/he made before lockdown. However, less than fifth visits (4 visits, 18%) resulted in participant spending more money on transportation than usual. This is expected as due to COVID-19 pandemic in the initial months majority of the government health facilities were converted into exclusive COVID facilities to contain the spread of the virus,[15] as a result of which patients in dire need had to visit other health facilities/practitioners. Along with the money these patient also ended up spending more time to avail services from these facilities/practitioners. Again this is expected as the precautions, norms of social distancing, need of having testing before seeing a doctor as well as a degree of fear even among health providers slowed down the patient care services.
Overall there was loss of both time and money in a section of people who had to seek surgical healthcare during lockdown at a time when there was loss of jobs, closure of work places, and shut down of unorganized sector.[16] This may also have forced people to delay seeking care for their health concerns/ problems. We report that over two fifth study participants (44.4%, 28 patients) delayed seeking care for their health problem/ concern. Majority of them (82.1%, 23 patients) cited nationwide lockdown as their primary reason, followed by being scared/ stigma of COVID 19 (50%, 14 patients). Although lockdown allowed continuation of essential services and healthcare was one of them,[12] still patient in our study feared/felt uncomfortable to reach out for healthcare services. There was a lot of cautionary messages spread across all spaces including electronic media (television, radio, and mobile phones) and print media regarding the seriousness of the COVID-19 pandemic, stringent precautions to avoid contracting the disease and strict enforcement (including fines and sometimes arrests) of lockdown measures may also have contributed to the fact that in-spite of being in need, people avoided seeking healthcare.
There is no doubt that lockdown forced people to remain in the confinement of their houses whether willingly or unwillingly. Some people managed to work from their home but many people from the unorganized sector lost their jobs and had to sit idle at home.[16] On the top of this for a patient not being able to visit a hospital or a doctor for follow-up or further checkups can affect the patient psychology adversely. In our study, 20 patients (32%) out of 63 felt a sense of helplessness during the lockdown. For most of them (11 patients), the reason was nonavailability of doctors easily or unable to visit the treating doctors or health facilities. At the end of data collection for this study (mid-September 2020) four patients whose surgeries were postponed were still awaiting for their surgery
In a study in China in the initial phase of the outbreak, more than half of the respondents had psychological impact in between moderate to severe; also about one third had anxiety levels in the category moderate to severe.[17] In our study, out of 52 self-responding patients, over a third of them (20 patients, 38.5%) experienced at least some anxiety with a sixth of them having moderate anxiety (09 patients, 17.3%) while almost half of them (48.1%) were stressed more than usual with a significant proportion (7.7% participants) experiencing severe stress.
There were certain issues which could have been anticipated better and remedial steps initiated at the very beginning. One of the solutions can be to operationalize at least one telemedicine facility in each block (administrative subunit of district in India) at the earliest – ideally even before initiating extreme steps – if such a situation presents in future. It can be an audio or preferably video tele-communication system. It will help in maintaining social distancing, avoid crowding and panic at the existing health care facilities and will allow patients to get necessary consultations in pre-operative as well as post-operative period. Doctors can also do a limited physical examination through video tele-conferencing saving both time and money both for patients and the health-care system.[18] Simple photographs from post-operative period can help in detecting and diagnosing many post-operative complications.[19] It may also be not necessary to completely stop surgical procedures at health facilities and totally converting them to COVID/other epidemic or pandemic specific facilities. Surgical procedures can be carried out at the same time in a separate designated area/ block of the health facilities while following strict standard infection prevention protocols at all stages of patient care. This of course will require robust infrastructure, adequate dedicated well trained manpower, and periodic refresher training of staff and doctors, and having capacity to develop and follow standard operating procedures and quality control measures. In a study conducted by Philouze P in France, they operated over 100 patients within duration of 4 weeks following and implementing all protocols formed for their hospital. There was only one case of cross infection and no mortality due to COVID-19.[20] Government needs to make better options available for surgical patients and their care and not just merely converting fully functional hospitals into dedicated COVID facilities. Awareness also needs to be spread among patients that they can visit hospitals by taking all necessary precautions.
The study has a relatively small sample size and is based on patient experiences from a single public sector health facility in National Capital Territory region of India. Therefore, the experiences of surgical patients included in this study may not be applicable for all surgical patients in a vast country like India. Also as the study is based on self-reported data, information bias especially desirability bias and recency bias cannot be completely ruled out.



COVID-19 was and still is a serious challenge for all governments and health systems around the world. Closing of fully functional hospitals and turning them to COVID facilities probably left a huge amount of backlog in surgical disciplines as well as created stress and anxiety among patients. Governments need to make options available for surgical patients and come up with acceptable alternatives before implementation of nationwide lockdowns or other similar steps. More research is needed – both qualitative and quantitative – to better establish the impact of stringent measures on care of surgical patients as well as to identify the innovations and policies which may have mitigated such an impact.
Subscribe now for latest articles and news.