Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.008
Year: 2021, Volume: 7, Issue: 2, Pages: 43-46
Original Article
Diwakar Kumar Singh1 , Animesh Gupta2 , Shahul Hameed3 , S Nanjesh Kumar4
1 Assistant Professor, Department of Community Medicine, Heritage Institute of Medical Sciences, Varanasi, Uttar Pradesh, India,
2 Associate Professor, Department of Community Medicine, Narayan Medical College and Hospital, Sasaram, Bihar, India,
3 Associate Professor, Department of Community Medicine, Kanachur Institute of Medical Sciences, Mangalore, Karnataka, India,
4 Professor and Head, Department of Community Medicine, K S Hegde Medical Academy, Mangalore, Karnataka, India
Address for correspondence:
Dr. Animesh Gupta, Department of Community Medicine, Narayan Medical College and Hospital, Sasaram, Bihar, India. Phone: +91-7411004444. E-mail: [email protected]
Introduction: It is estimated that there are around 140 million children are orphans worldwide. These children suffer from physical neglect, poor hygiene, and a lack of nutrition, which result in various health problems among children. They are more prone to malnutrition, respiratory tract infection, skin diseases, and dental caries.
Aim: This study aims to assess the health status among children living in an orphanage.
Methods: A cross-sectional study was conducted at Kanyana residential ashrams or orphanages. The data were collected using pretested semi-structured questionnaire which includes sociodemographic profile, personal hygiene, anthropometric measurement, clinical examination, and investigation. Body mass index and anemia were classified as per the WHO criteria. Data were analyzed using appropriate statistical software.
Results: The mean age of the group of 69 children was 11.86 ± 2.29 years. Skin disease or infection and dental carries were most prevalent among children. The prevalence of moderately underweight, severely underweight, and anemia were 18.8%, 10.1%, and 21.7%, respectively.
Conclusion: The present study showed that the maximum children had skin disease and dental carries because of poor personal hygiene. Even the prevalence of anemia among children was slightly lower than the national data.
KEY WORDS: : Anemia, children, morbidity, nutritional status, orphanages
As per UNICEF, orphan can be defined as a child aged <18 years, who has lost either one or both parents by any cause of death.[1] It is estimated that there are around 140 million children are orphans worldwide.[2] In India, many orphan and street children are left without care and support and the main cause is urbanization and industrialization. Due to family disputes, accidental deaths, illegal contacts, etc., many children are becoming parentless. These orphan/ street children are involved in rag picking; pick pocketing and participating in antisocial, criminal activities.[3] The health of children is important that they constitute 25% of India’s population.[4] Many of these children suffer from physical neglect, poor hygiene, and a lack of nurturing is all too common even in today’s modern orphanages which results in various health problems among children.[5] The global burden of undernourished or malnourished children is an important public health issue since ancient times and it is still more common among children living in developing countries.
Children residing in orphanages or social welfare ashram/hostels are more prone to malnutrition as compared to children staying at home with their parents and this would lead to more mortality and morbidity conditions among these children.[6]
The most common health problems among children are malnutrition, respiratory tract infections, diarrhea, dysentery, intestinal worm infestation, infestation of lice, skin diseases, dental caries, etc. Hence, this study was planned with aim to assess the nutritional status among children living in an orphanage.
A cross-sectional study was conducted at Kanyana residential ashrams/orphanages which are situated around 47 km from Mangalore, Karnataka. After obtaining ethical approval from the Institutional Ethics Committee, the data were collected for a period of 6 months from July 2013 to December 2013, using pretested semi-structured questionnaire which includes sociodemographic profile, personal hygiene, anthropometric measurement, clinical examination, and investigation. Consent from legal guardian was taken. In case of children, additional questions were asked regarding personal hygiene and assessed. Nutritional assessment was done by the anthropometric measurement such as weight, height, and body mass index (BMI) of the child. The reference for underweight, stunted, and wasted was taken as per the WHO growth standards charts for their age.[7]
Clinical examination was done in good day-light which included vitals sign, general physical examination, oral cavity examination, and visual acuity. An arbitrary 10-point scale was devised for classifying the level of personal hygiene. Score 0 and score 1 were given for unfavorable and favorable outcomes, respectively. Total score was calculated by adding 10 questions. Score ≥7 considered good, 4–6 considered satisfactory, and score ≤3 considered poor hygiene.
Anemia was classified as per the WHO criteria.[8] Data were collected and entered into Microsoft Excel sheet. It was then tabulated and analyzed using SPSS software (Trial Version 21).
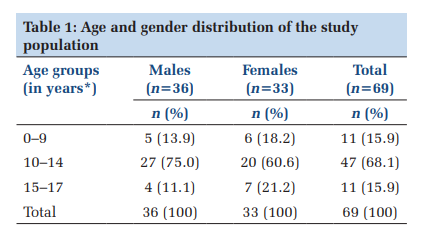
A total of 69 children were included in this study and majority of them belonged to the age group 10–14 (68.1%) years. The mean age of the group was 11.86 ± 2.29 years (males – 11.64 and females – 12.09) (Table 1).
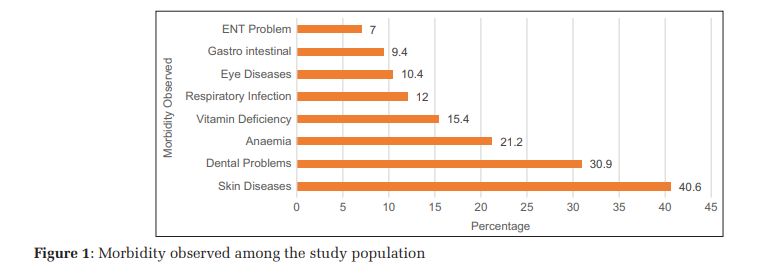
The majority of the children had skin disease (40.6%) followed by dental problems (30.9%) and anemia (21.2%) (Figure 1).
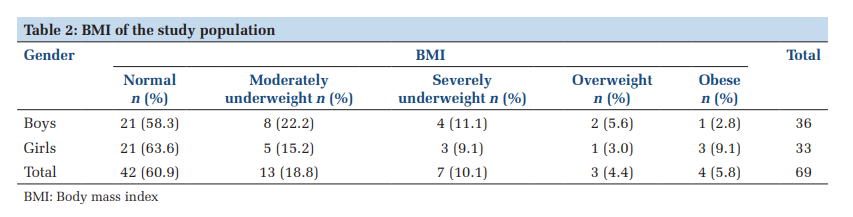
Majority of children’s BMI was normal (60.9%) followed by 18.8% of children had moderately underweight (Table 2).
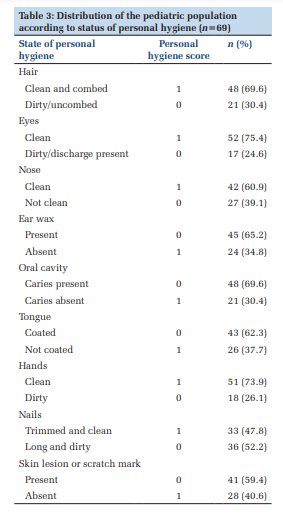
Table 3 shows that majority of the study population (n = 69) had favorable outcomes such as clean hair (69.6%), eyes (75.4%), nose (60.9%), hands (73.9%), and undergarments (84.1%), respectively. Only 1.4% of children had poor (score <1) personal hygiene. Maximum children had good personal hygiene.
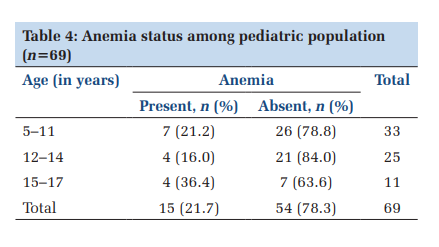
The prevalence of anemia was 21.7% and maximum prevalence was observed among children aged 15–17 years (Table 4).
In this study, maximum number of children were in the age group of 10–14 years. Similar findings were observed in Shukla and Shukla study in Chennai, which revealed that the highest percentage of children (29%) were in between the age group of 13 and 14 years.[9] The most common morbidity observed among children in this study was skin diseases followed by dental problems. Chhabra et al. conducted a study among orphanages in Delhi, revealed that skin disease was the most common morbidity (31.7%), followed by diseases of the oral cavity (16.1%), which was comparable to our study findings.[10] Even in the study done by Mayavati et al. in Pune, in primary school showed that majority of children (65.1%) were suffering from dental caries, followed by 38.2% having upper respiratory tract infection.[11]
In this study, 28.9% of children were malnourished and boys were more underweight or malnourished as compared to girls. In a study done by Sharada et al. in Bangalore city, the prevalence of underweight or malnourished among children in the age group of 5–9 years was 35.07%, which was similar to our study findings.[6] Similarly in the study by Chhabra et al. in New Delhi, the boys were found to be more malnourished than girls, which was similar to our study result.[10] In the study done by Shukla B and Shukla D among orphanages in Chennai, showed that 57.70% of orphanage children were malnourished, which was much higher to this study findings.[9] This may be because of poor nutrition and care provided to the orphanage children. The personal hygiene was almost good among all children in this study. Maximum children comb their hair, clean their eyes, and clean oral cavity. In the study by Deb et al. at Kolkata, results showed that majority (50%) of children had average personal hygiene, followed by good personal hygiene in 30.4%.[12]
Even in a study conducted by Reddy et al. among orphanages in Odisha, showed that 51% of children had good hygiene scores.[13] Even, in the study by Mayavati et al. in Pune, in primary school showed that majority of children had good personal hygiene scores.[11]
In this study, around one-fifth (21.7%) children are anemic as per the WHO cutoff point. This may be due to inappropriate intake of iron-rich food or proper nutrients or may be due to parasitic infection. In a study done by Reddy and Ramya in Chitradurga, the prevalence of anemia was 37.4% among orphanages children, which was comparable to our study findings. [14] In the study by Deb et al., among children in schools, the most common morbidity was pallor which is sign of anemia.[12] Even in the study done by Gur et al. among schoolchildren aged 6–16 years in Istanbul, revealed that the prevalence of anemia was 27.6%, which was comparable to our study findings.[15]
As this study was cross-sectional and had small sample size, thus the results may be representative of small community and had a limited extrapolative value. Only anthropometric measurement and hemoglobin estimation were done for the assessment of nutritional status of children, micronutrients deficiency was not assessed.
The present study showed that the maximum children staying at orphanages/ashram had good nutritional status. Most of the children had skin disease and dental carries because of poor personal hygiene. Even the prevalence of anemia among children was slightly lower than the national data. Health education program on hygiene practices and balanced diet should be emphasized. Periodic health check-up and screening of malnutrition should be conducted in the orphanages or ashram.
Subscribe now for latest articles and news.