Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i1.24.216
Year: 2025, Volume: 11, Issue: 1, Pages: 8-14
Original Article
Paheli Maru1 , Vibha R Vyas1 , Varnika Rai1 , Shilpa Kapoor1 , Samanta Satarupa1
1Assistant Professor, Oncopathology Department, Gujarat Cancer Research Institute, Ahmedabad, Gujarat, India
Address for correspondence:
Samanta Satarupa, Assistant Professor, Oncopathology Department, Gujarat Cancer Research Institute, Ahmedabad, Gujarat, India.
E-mail: [email protected]
Received Date:07 July 2024, Accepted Date:23 October 2024, Published Date:06 February 2025
Background: The liver is a common site for malignant tumors, both primary and secondary. An early and accurate diagnosis can help in the clinical management of these tumors. Fine needle aspiration cytology (FNAC) is a minimally invasive procedure that aids in an earlier diagnosis than a biopsy. Aims and Objectives: 1) The main objective of the present study was to establish the adequacy and accuracy of FNAC in diagnosing malignant liver tumors in a tertiary cancer institute, 2) To analyze inconclusive and inadequate aspirations and find out diagnostic pitfalls. Materials and Methods: A total of 406 patients underwent image-guided percutaneous FNAC and biopsy sampling of liver mass lesions from 2018–2020. Hematoxylin, eosin, and May-Grünwald-Giemsa stains were examined. Statistical analyses were performed using histological diagnoses from liver biopsy samples as the gold standard to ascertain the sensitivity, specificity, and accuracy of FNAC in the diagnosis of liver lesions. Results: Among the 406 aspirations received over a period of three years, 364 (90%) were adequate, 30 (7%) were inconclusive and 12 (3%) were inadequate. Among the positive aspirations, primary hepatic malignancies were 69 (20%) and secondary malignancies were 230 (63%), the most common being gastrointestinal primaries. The sensitivity, specificity, accuracy, positive predictive value and negative predictive value of FNAC in diagnosing malignant liver lesions in our center were 87.25%, 71.21% and 22.72% respectively. Paucicellularity, repeated aspirations from the necrotic area and aspiration of reactive hepatocytes in the vicnity of metastasis were the most frequent diagnostic errors. Conclusion: Fine needle aspiration cytology is a cost-effective and precise diagnostic method for both primary and secondary malignant liver cancers. It should be incorporated as a point of care in personalized medicine.
Keywords: Malignant liver lesions, Fine needle aspiration cytology, Sensitivity, Specificity
Liver mass lesions are often evident at an advanced stage because they don't cause any symptoms for a long time. Both primary tumors of higher stage and metastatic malignant tumors are inoperable at the time of presentation. Clinical, radiological, and serological findings cannot reliably distinguish a benign from a malignant lesion, as well as primary from metastatic tumors; but they can help narrow the differential diagnosis.
The primary indicator for FNAC of the liver is one or more localized abnormalities shown on radiography (US or CT scan), as the majority of these tumors are impalpable. Due to its accuracy in these situations, FNAC with image guidance is becoming more and more accepted as the preferred diagnostic method. Because of its ease of use, flexible needle placement, real-time monitoring and infrequent, if any, aftereffects, ultrasound guidance is typically chosen. 1, 2
Fine needle aspiration cytology (FNAC) is a straightforward test used to diagnose palpable malignancies of the superficial organs before surgery. Since its discovery, the initial diagnosis of various lesions using safe, cheap, rapid, and relatively painless cytology
A quicker, less expensive, and less intrusive method for diagnosing benign and malignant lesions in deeper organs is percutaneous fine-needle aspiration cytology. Ehrlich applied this to the liver for the first time in 1893, and in 1923 it was done for the first time as a diagnostic procedure. 3
The current study sought to determine the diagnostic pitfalls associated with inconclusive and inadequate aspirations, as well as the accuracy of an ultrasound-guided fine needle aspiration cytomorphological study as a quick and affordable procedure for diagnosing liver lesions in correlation with histopathology in a tertiary cancer institute in West India.
This was a retrospective observational study conducted at a tertiary cancer center in India between January 2018 and December 2020. A total of 406 patients who underwent a fine-needle aspiration biopsy of liver lesions were enrolled in the study using a non-random, convenient sampling method. Following clinical, biochemical, and radiographic signs of liver illness, these patients were made to undergo FNAC and biopsy.
Using a 20- or 22-gauge, 90-mm spinal needle and two to three passages into the lesion under ultrasonic guidance, the cytological material was extracted. After making five to seven smears, they were fixed in 95% methanol and stained with hematoxylin and eosin (H&E), papanicolaou (PAP) and other dyes. Trucut biopsy samples acquired through ultrasound guidance were processed, embedded in paraffin blocks, and fixed in 10% formalin. H&E stain was applied to the sections and when necessary, immunohistochemistry was carried out.
Benign and malignant lesions were gathered using the first in first out rule to eliminate selection bias. Both FNAC and biopsy slides were rereviewed in all the cases. Immunohistochemistry was used to give a confirmatory diagnosis wherever required. The sensitivity, specificity and accuracy of FNAC in the diagnosis of liver lesions were assessed statistically using the SPSS software and Chi square method. Liver biopsy histopathological findings served as the gold standard. A portion of the patients' baseline characteristics were reported as percentages, while others were stated as means and +/- SD.
The mean age of the patients with HCC was 58.72 years; hepatoblastoma was 4 years; and secondary malignancy was 55.15 years. The incidence in males was higher in both primary (M:F = 1.3:1) (129 and 98) and secondary hepatic malignancy (M:F = 4.7:1) (47 and 10). FNAC was repeated twice in 35 patients and three times in 13 patients. There were no mortalities following the procedure and there were no bleeding episodes.
Positivity for hepatitis B surface antigen (HBsAg) was found in 28% of cases, while anti-HCV antibody was detected in 4% of HCC. None of the cases of hepatoblatoma showed a positive viral serology. Secondary hepatic malignancy also showed positivity for HBV in 3.5% of cases, mostly of colorectal origin and none for HCV.
An elevated serum AFP level was detected in primary hepatocellular carcinoma (55/64). The tumor markers Carcinoembryonic Antigen (CEA) and CA-19.9 could predict secondary malignancy wherever suspected.
The examination of cellularity, pattern of cells, cytoplasmic and nuclear details, among many other characteristics, was included in the cytomorphological investigation. Among the 406 aspirations received over a period of three years, 364 (90%) were adequate, 30 (7%) were inconclusive and 12 (3%) were inadequate. The inconclusive and inadequate aspirates were excluded from the study. Primary malignancy was detected in 69 cases, out of which hepatocellular carcinoma comprised 64 cases and hepatoblastoma comprised 3 cases (Figure 1, Figure 2).


Among the 364 adequate aspirates, 278 were signed out as malignant tumors and 86 as benign or normal hepatic parenchymal tissue. FNAC was correlated with histopathological examination in all the patients. Biopsy confirmed malignant tumors in 299 cases and benign or normal hepatic parenchyma in 65 cases. However, 47/86 cases were benign or truly negative for malignancy on FNAC. In 39 patients, FNAC was benign; however, it turned out to be malignant on histopathological examination, out of which 37 patients were secondary and 7 patients had hepatocellular carcinoma. In 18 cases, FNAC raised suspicion or a false positive for primary or secondary malignancy (Table 1). In order to diagnose malignant liver lesions at our center, the sensitivity, specificity, accuracy, positive predictive value and negative predictive value of FNAC were, thus, 87.25%, 71.21%, and 22.72%, respectively (Table 2).
|
|
Malignancy present |
Malignancy absent |
|
|
FNAC Positive |
260 |
18 |
278 |
|
FNAC Negative |
39 |
47 |
86 |
|
Total |
299 |
65 |
364 |
|
Statistic |
Value |
95% CI |
|
Sensitivity |
87.25% |
82.92% to 90.82% |
|
Specificity |
71.21% |
58.75% to 81.70% |
|
Positive Likelihood Ratio |
3.03 |
2.07 to 4.44 |
|
Negative Likelihood Ratio |
0.18 |
0.13 to 0.25 |
|
Disease prevalence (*) |
95.00% |
|
|
Positive Predictive Value (*) |
98.29% |
97.52% to 98.83% |
|
Negative Predictive Value (*) |
22.72% |
17.38% to 29.11% |
|
Accuracy (*) |
86.45% |
82.50% to 89.79% |
Secondary malignancy was detected in 230 cases and comprised predominantly of metastatic adenocarcinoma (73%). Others included poorly differentiated carcinoma, metastatic small cell carcinoma, GIST, squamous cell carcinoma, sarcomas, and non-Hodgkin lymphoma (NHL) (Figure 3 a). The gastrointestinal tract was the primary source of metastases from metastatic adenocarcinomas, which were the most common cause of space-occupying lesions in the liver. This was followed by the pancreatobiliary region (18%). The distribution of the various malignant lesions of the liver is summarized in (Figure 3 b).

The liver is a common site for benign as well as primary and secondary malignancies. Differentiation between benign and malignant liver lesions is extremely important from a management point of view. While surgical excision is a possibility and may guarantee a cure if HCC is detected early, the development of metastases typically precludes surgery. Supportive therapies for advanced metastatic tumors and partial hepatectomy for primary carcinomas are among the possible treatments.
The most prevalent primary malignant tumor of the liver is hepatocellular carcinoma (HCC), which often manifests as unifocal or occasionally multifocal tumors. 4 On the other hand, primary cancer and hepatic infiltration with secondary cancers present with comparable clinical presentations. Even though it's generally accepted that adenocarcinoma metastases are many and hypoechoic on ultrasonography when compared to the surrounding liver parenchyma 5 , accurate definition of the individual lesions isn't always possible using radiological imaging. When serological markers, like AFP, are noticeably increased, they can help narrow the differential diagnosis. Unfortunately, on initial presentation, most patients do not have increased levels of these markers. Thus, FNAC and biopsy play a major role in the evaluation of a hepatic mass. This makes the liver probably the most common target of an abdominal deep-organ FNA biopsy.
The use of imaging tools has made guided aspiration from deep-seated liver lesions a common practice. Ultrasound provides the best real-time guidance with needle tip visualization of all the imaging techniques. It also has advantages like easy availability, relatively low cost, speed, and absence of radiation, making it the preferred method for guided FNAC.
The ability to sample the mass in several planes and execute many needle punctures during the aspiration biopsy technique are two benefits of FNAC. Furthermore, aspiration cytology enables prompt analysis of the data, enabling the assessment of a specimen's suitability and the acquisition of extra material for supplementary diagnostic investigations if necessary. 6 But FNAC has its own set of limitations for liver lesions. It is less useful in patients with diffuse parenchymal diseases like hepatitis or cirrhosis, and a well-differentiated hepatocellular carcinoma can be confused with a benign lesion.
Among complications, there is some, albeit very little, risk of bleeding and intraperitoneal tumor spillage. Needle track seeding, bleeding and bile leakage are some of the risks linked to FNAC. For abdominal malignancies, the incidence of mortality following FNAC procedure is estimated to be between 0.006% and 0.031% 7 . After FNAC for liver tumors, the risk of needle tracking is typically between 0.003% and 0.009% 8 . However, more recent research has indicated that primary liver tumors have a higher chance of needle tracking (0.4%–5.1%) 9 .
Men are affected by HCC 2.1 to 5.7 times more commonly than women, according to a surveillance study conducted in the USA (mean 3.7:1). In places with intermediate incidence, the ratio falls to a mean of 2.4:1, while in areas with low incidence, it is lower. 10 Men also had a higher incidence of primary and secondary cancers, according to our study. The trophic influence of androgens, exposure to environmental pollutants, and variations in hepatitis carrier states could all be contributing factors to this variation in sex distribution. 11
According to one study, which used a representative sample from 11 WHO-based regions, HBV (53%) or HCV (25%) are responsible for 78% of HCC cases worldwide.11 These diseases typically cause more than 50% of HCC in a given region. Regionally, these infections usually account for >50% of HCC. 12 In this study, only 32% of cases were attributable to HBV (28%) and HCV (4%). Secondary hepatic malignancy also showed positivity for HBV in 3.5% and none for HCV.
The effectiveness of FNAC in the treatment of metastatic cancer has been reaffirmed by numerous extensive series of hepatic aspirates. Several reports have also confirmed the procedure's accuracy in diagnosing primary hepatocellular cancer. 4 In the literature, the sensitivity of FNAC to liver neoplasms ranges from 92 to 96%. 3 The specificity of FNAC in the liver reaches 100% when it comes to differentiating between benign and malignant lesions, while the sensitivity varies from 67 to 100%, with an average of approximately 85%. 9, 13
The diagnostic accuracy in our study (86.45%) was similar to that by Kuo et al. (86.1%) 14 and lesser as compared to that reported by Swamy et al. 15 (97.5%) and Mondal et al (99.5%). 16 One major study indicated that the sensitivity, positive, and negative predictive values of FNAC diagnosis for liver cancer were 100%, 59.1%, and 92.4%, respectively. 17 The sensitivity and specificity were lower in our study was lower as compared to others. The negative predictive value of FNAC in this study is only 22%. This could be due to a discrepancy in the number of benign and malignant lesions which is because ours is a referral cancer centre. Ours being a referral cancer center, we received more malignant cases. A major proportion of adenocarcinomas were signed out as poorly differentiated tumors because it was difficult to differentiate whether they were primary or metastatic. The false-positive cases were misdiagnosed due to reactive atypia in hepatocytes. The false negative aspirates were paucicellular and consisted predominantly of macrophages.
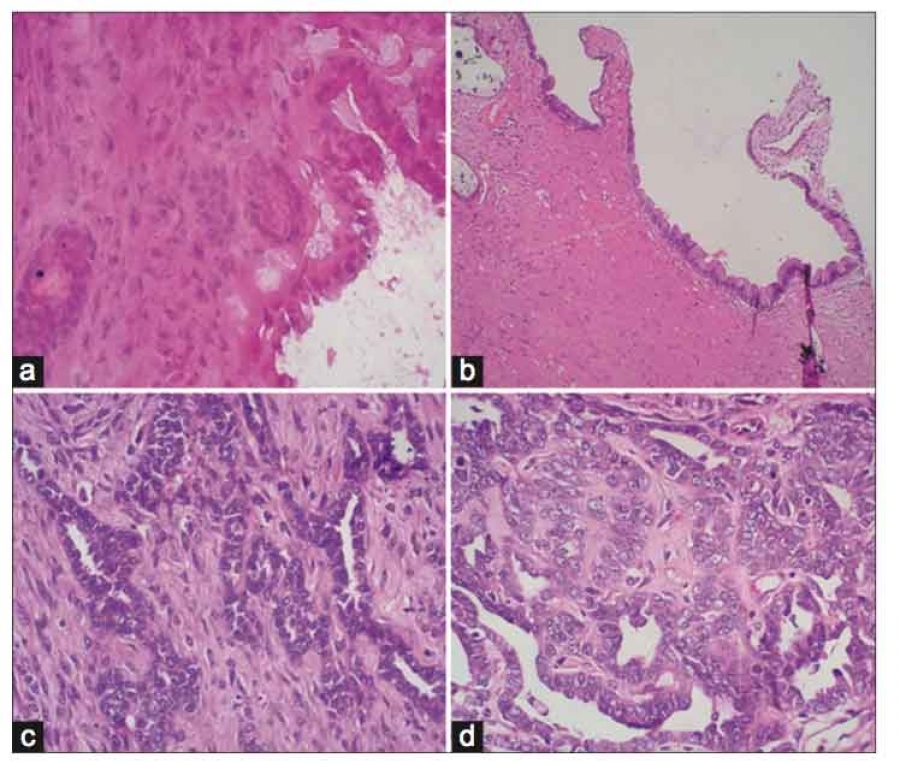
The salient features of cytology that aid in the diagnosis of HCC are transgressing vessels within cell clusters and cell clusters lined by endothelial cells, whereas metastatic adenocarcinomas appear as a foreign population of cells, forming acini with columnar configuration and occasional intracytoplasmic mucin. The preserved architectural pattern in histological specimens and the ease with which auxiliary procedures, like mucin stains or immunohistochemistry, can be applied to biopsy material are two factors contributing to the discrepancy in cyto-/histo-pathological analysis. Consequently, it is important to think of these two methods as complimentary while looking at liver abnormalities. 18, 19
When compared to non-neoplastic lesions, malignant lesions among all hepatic lesions were diagnosed with greater accuracy. Research on non-neoplastic and particularly neoplastic mass lesions of the liver has shown that FNA biopsy is helpful (Nasit et al., 20 ; Hemlatha et al., 21 ).
Numerous parameters, including aspiration methods (guided or blind), the number of passes, operator skill, lesion size, location, consistency, smear quality, combination of ancillary testing and cytohistologic studies, and reader expertise, might affect sensitivity. The most important requirement for cytodiagnosis is to obtain a representative sample. Aspirated material from the tumor's surrounding tissue may only exhibit proliferative and reactive alterations. On the other hand, a big tumor's aspirate may solely contain necrotic and degenerative material. Therefore, the needle needs to go through the full mass of the tumor in order to obtain a representative aspirate. Assistance from a cytopathologist during the procedure can increase overall accuracy. Rapid on-site evaluation (ROSE) helps in ensuring the adequacy of material for evaluation.
Although it is associated with low risk of needle tracking in malignant liver lesions 22, in situations when costs and the accessibility of investigations are constraints, FNAC can nevertheless be a secure, efficient, fast, and reasonably priced diagnostic instrument.
When a patient cannot afford a computed tomography (CT) scan, FNAC from liver under ultrasound guidance is a highly helpful tool. When patients have advanced cancers and do not require active cancer-directed therapy, it can be helpful to counsel them. However, a combined strategy of FNAC with clinical symptoms, tumor markers, and ancillary procedures should be performed to gain maximum diagnostic information with a reduction of ambiguous reports.
PM, VR and SK: acquisition of the data. PM, VR and SK: analysis and research of the literature, and preparation of the manuscript. PM, VV and SS: conception and design of the manuscript and critical revision of the manuscript for intellectual content. VV and SK: critical revision of the manuscript for intellectual content. SS: administrative support and supervision. All authors read and approved the final manuscript.
The authors received no financial support for the research, authorship, and/or publication of this manuscript.
The authors declare that they have no competing interests.
Subscribe now for latest articles and news.