Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i01.009
Year: 2016, Volume: 2, Issue: 1, Pages: 40-44
Case Report
M M Gopalaraju1, M Senthil Raja2, S Fiasmusthafa3, W Ajay Samkumar3, R Shankar4
1Professor, Department of Medicine, Vinayaka Mission’s Kirupananda Variyar Medical College and Hospitals, Salem, Tamil Nadu, India,
2Assistant Professor, Department of Medicine, Vinayaka Mission’s Kirupananda Variyar Medical College and Hospitals, Salem, Tamil Nadu, India,
3Post Graduate, Department of Medicine, Vinayaka Mission’s Kirupananda Variyar Medical College and Hospitals, Salem, Tamil Nadu, India,
4Associate Professor, Department of Community Medicine, Vinayaka Mission’s Kirupananda Variyar Medical College and Hospitals, Salem, Tamil Nadu, India
Address for correspondence: Dr. M M Gopal Raj, Department of Medicine, Vinayaka Mission’s Kirupananda Variyar Medical College and Hospitals, Salem, Tamil Nadu, India. E-mail: [email protected]
Cysticercosis is a parasitic disease caused by Taenia solium. It is a major public health problem in developing countries. Infection is acquired through ingestion of undercooked meat containing the cysticercus. Man is the definitive host and pig is the intermediate host. Cysticerci can be found anywhere in the body but are most common detected in brain, eye, skeletal muscle and subcutaneous tissue. One of the uncommon manifestations and a rare complication is its disseminated form. Neurocysticercosis is the most common parasitic disease of the central nervous system. Widespread dissemination of the cysticerci can result in the involvement of almost any organ in the body. We report a case of a 65-year-old person with disseminated cysticercosis (DCC) who had presented to our hospital with pain and swelling in smaller joints of hands and multiple palpable nodules in thighs. Computed tomography brain, whole body magnetic resonance imaging, X-rays and biopsy of the muscle had confirmed the diagnosis of DCC involving the brain, subcutaneous tissue, and skeletal muscles. The patient was treated with the albendazole 400 mg bid, for 30 days along with steroids. There was no history of convulsions in our case even though there was neurocysticercosis. The patients are currently under follow-up without any major complications.
KEY WORDS:Parasitic disease, Cysticercosis, Disseminated.
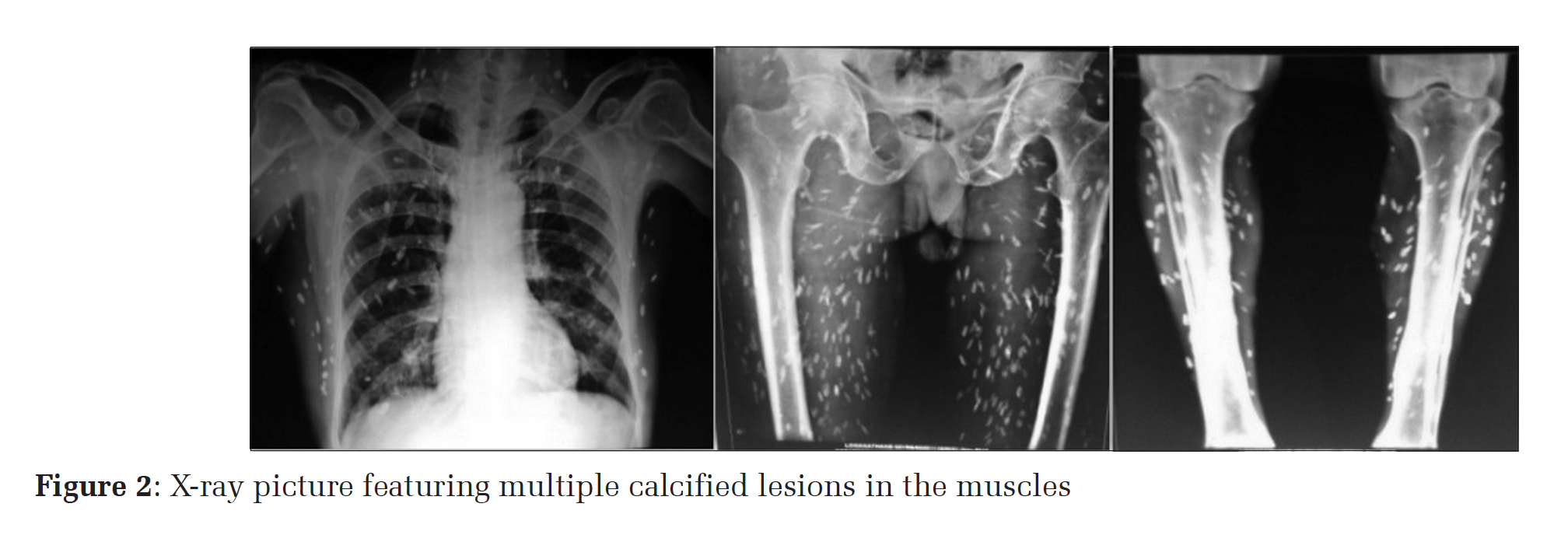
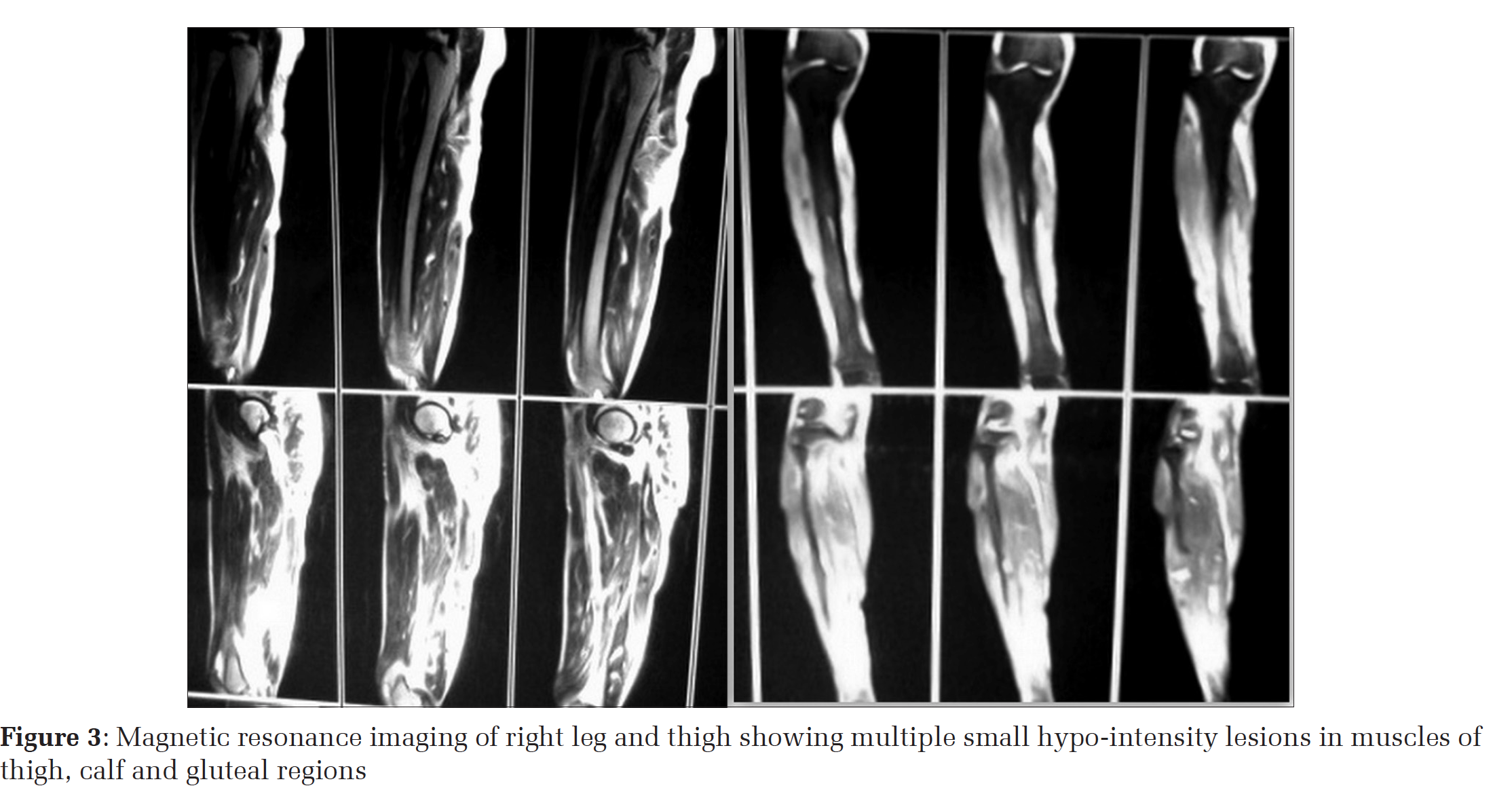
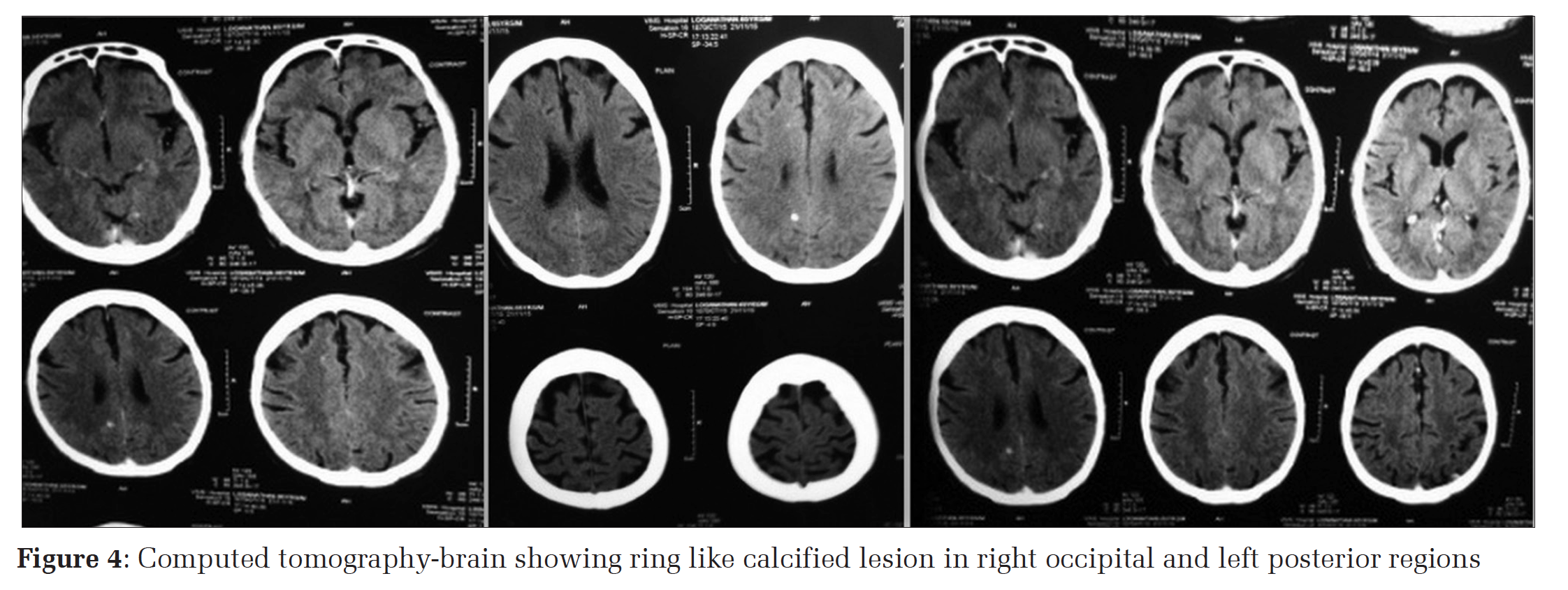
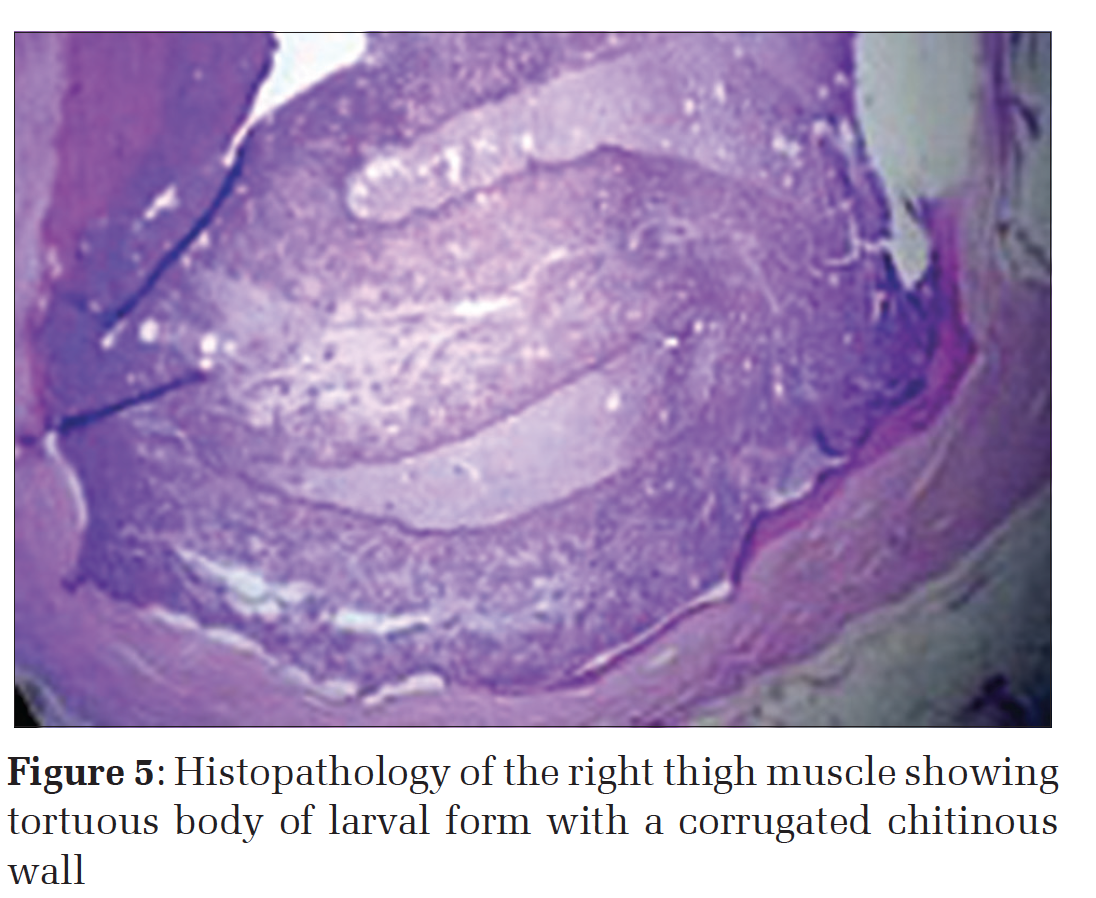
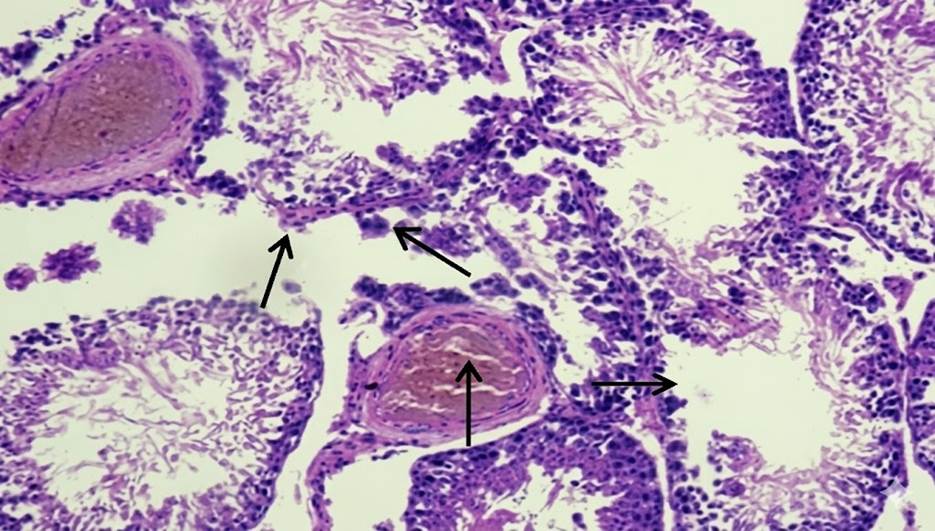
IntroductionCysticercosis is a parasitic disease caused by Taenia solium larva and it is a major public health problem in developing countries. It is considered as endemic in most parts of southeast Asia, and Africa.[1] The cysticercosis is common in places where the pigs are eaten undercooked, and the level of personal hygiene is a very poor. Neurocysticercosis is the most common type of cysticercosis. Human is the only definitive host of T. solium, and pig is the intermediate host, man can also act as an intermediate host.[2] Dissemination of the cysticerci larva was almost found in all places throughout the human body as reported by Krishna swami about a century back in 1912.[3] The main features of disseminated neurocysticercosis include intractable epilepsy, dementia, and enlargement of the muscles, subcutaneous and lingual nodules, and a relative absence of focal neurological signs or obvious raised intracranial pressure.[4] A set of diagnostic criteria for neurocysticercosis based on neuroimaging studies, serological tests, clinical presentation and exposure history had been explained in detail by Del Brutto et al.[5] Computed tomography (CT) and magnetic resonance imaging (MRI) remains the gold standard for diagnosing neurocysticercosis. The sensitivity of serological tests was high for patients with multiple cysts but it loses its significance if the cyst is either single or calcified. Cysticidal drugs such as albendazole and praziquantel have a wonderful effect in killing most of the parasites. The seizures with epileptic drugs come under control after treatment with these drugs. Del Brutto et al. had proven in his study that 83% of the patients who had received cysticidal treatment became seizure free when compared to only 26% of those patients who did not receive the cysticidal drugs.[6] Here, we report a case of disseminated cysticercosis (DCC) with diffuse involvement of the subcutaneous tissues, skeletal muscles, and brain. Case ReportA 65-year-old man from a rural area in Salem district presented with pain and swelling in the interphalangeal and wrist joints bilaterally (Figure 1). There was no history of recurrent fever, chronic cough, chronic diarrhea, weight loss, decreased appetite and past history suggestive of diabetes and tuberculosis. There was also no history of a headache, seizures or cognitive impairment. Swellings in the joint were insidious is onset, gradually increasing in size and it was associated with pain. The dietary history of the patient revealed that he had the habit of eating pork and beef from the childhood.On examination, the patient was conscious, alert and his appearance looked normal. There were no neurologic deficits seen on physical examinations. The only sign detected in the patient was tenderness present over the interphalangeal and wrist joints. In blood examination, the rheumatoid arthritis factor was found to be positive; erythrocyte sedimentation rate was elevated, C-reactive protein was positive (1:4 dil) 24 mg/L. Human immunodeficiency virusantibody test using enzyme-linked immunosorbent assay was negative. A routine X-ray chest showed multiple calcified lesions in the muscles and subcutaneous areas (Figure 2). Immediately, we screened the whole body with X-rays and MRI. MRI of the right leg and thigh showed multiple small hypo-intensity lesions in muscles of the thigh, calf and gluteal regions which were suggestive of multiple calcifications primarily due to cysticercosis of Stage IV (Figure 3). Cerebrospinal fluid (CSF) routine analysis revealed high protein, and antibody detection of parasite both in blood and CSF was negative. Ophthalmic examination showed no involvement. The electrocardiogram was normal sinus rhythm. CT-brain showed ring-like calcified lesion in right occipital and left posterior region (Figure 4). The biopsy from the right thigh muscle was sent for histopathological examination and it revealed tortuous body of larval form with a corrugated chitinous wall and diagnosed as cysticercus cellulose, T. solium larva (Figure 5). The patient was treated with albendazole 400 mg twice a day for 1 month along with steroids. No adverse drug reaction was reported by the patient during the treatment. The patient had no complaints of seizure in spite of central nervous system (CNS) involvement. The pain and swelling in the inter-phalangeal joints and the wrist joints was reduced. The patient was discharged and is regularly followed up in the outpatient clinic without any significant events. |
|
DiscussionThe life cycle of T. solium has two hosts, man the definitive host and pigs are the intermediate host. Intestinal taeniasis occurs when humans eat poorly cooked pork meat with living cysticerci (larvae) which develop into an adult worm in the small intestine, become attached to intestinal wall and start liberating gravid proglottides in feces. Human cysticercosis is caused by the dissemination of the embryos from the intestine it reaches the systemic circulation via the hepatoportal system and from there it travels further to almost all the organs of the body.[7] In most of the time these cysts are rapidly destroyed by our immune system except in certain immunologically privileged sites like a nervous system.[8] The sensitivity of stool examinations is poor in cases of neurocysticercosis, where the literature had shown only and 15% of patients harbor the larva at the time of diagnosis of neurocysticercosis. Parasites usually get lodged in the central nervous system resulting in neurocysticercosis. The larval stage might infest other tissues like skeletal muscle, diaphragm, heart, peritoneum, pleura and subcutaneous tissue.[9] The clinical symptoms of cysticercosis are usually based on the involvement of that particular organ. Among the various forms of cysticercosis, neurocysticercosis is the most common where the larva would get lodged in the brain parenchyma followed by meninges, ventricles, eyes and spinal cord. Normally, the presence of viable, living cysticerci larva in the central nervous system does not cause any symptoms. Hence, this patient also did not have any symptoms related to CNS manifestations. The symptoms may occur 5-10 years after infection. Pseudohypertrophy of the muscles is the most common presentation of DCC, followed by palpable nodules and seizures.[6] Whereas our patient did not have seizures, it had only features of pain and swelling in the smaller joints of the hand and the wrist joint, where the swelling of the joints might be due to the pseudohypertrophy of the muscles. MRI is a more sensitive than CT in identifying the scolex and live cysts in cisternal spaces and ventricles.[10] Unenhanced CT scans of muscles can demonstrate innumerable cysts standing out clearly against the background of the muscle mass in which they are embedded, the CT image would appear like a honeycomb or leopard spots.[11] In our case also both CT-brain and the MRI had proven the presence of the cysts in the various parts of the body. Definitive diagnosis of cysticercosis would always require a histological examination of the biopsy sample showing the cysticercus as was established in our case. The parasite appears as an undulating laminated membranous wall of a cysticercus (the larvae of a tapeworm), with associated marked inflammatory reaction (Figure 5). Management of DCC includes symptomatic treatment of the central nervous system lesions for the control of seizures using steroids and antiepileptics. In patients with raised intracranial tension, surgical removal of cysts and ventriculoperitoneal shunting is warranted. Pharmacological management with cysticidal drugs praziquantel (10-15 mg/kg/day for 6-21 days) and albendazole (15 mg/kg/day for 30 days) is the treatment of choice for reducing the parasite load. Few adverse drug reactions had been reported for these drugs like enlargement of the cysts causing a massive release of antigens leading on to local tissue swelling, and a generalized anaphylactic reaction. A low dose of steroid along with these drugs would take care of those adverse effects. There is no role for cysticidal drugs in inactive neurocysticercosis, which means the cysts are calcified and the parasites are dead.[12] As our case did not have any manifestations related to CNS anti-epileptics were not used, only albendazole along with a minimal dose of steroid was used to reduce the parasite burden.
ConclusionDCC is a very rare parasitic infection, as it go unnoticed many a times. It is important to recognize the condition clinically and perform appropriate radiological and serological investigations to confirm the diagnosis and treat the condition at the earliest with the available cysticidal drugs. Patients who are not treated effectively and who have active cysts remain at a risk both for themselves as well as for the community. |
Subscribe now for latest articles and news.