Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.012
Year: 2021, Volume: 7, Issue: 2, Pages: 74-78
Original Article
Md. Mahboob Alam1 , Bikashendu Samui2
1 Associate Professor, Department of Physiology, M.J.N Medical College and Hospital, Coochbehar, West Bengal, India ,
2 Assistant Professor, Department of Physiology, Coochbehar Government Medical College and Hospital, Cooch Behar, West Bengal, India
Address for correspondence:
Dr. Bikashendu Samui, Assistant Professor, Department of Physiology, M.J.N Medical College & Hospital, Vivekananda Road, Khagrabari, Coochbehar, Pin – 736101, West Bengal, India. Phone number: +91-9903483880. E-mail: [email protected]
Background: Reports on pulmonary function in overweight and obesity are conflicting
Objective: The objective of the study was to evaluate the effect of increasing weight on dynamic pulmonary parameters.
Methods: A cross-sectional study involving healthy young adult male Bengali subjects was carried out in a tertiary care center in eastern India. The subjects were stratified into underweight, normal, and overweight based on their body mass index (BMI). Forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), FEV1/FVC ratio, forced expiratory flow between 25 and 75% of vital capacity (FEF25-75%), and peak expiratory flow rate (PEFR) were measured.
Results: Out of 153 male subjects, 27 were underweight, 96 were normal, and 30 were overweight. All the subjects were between 18 and 23 years. Median height, weight, and BMI were 170 cm, 60.1 kg, and 21.46 kg/m2 , respectively. Median FVC, FEV1, FEV1/FVC, and PEFR were 3.806 L, 3.2271 L, 85.22%, and 7.024 L/s, respectively. None of the respiratory parameters differed significantly between normal and overweight although lower FVC and higher FEV1/FVC was noted in underweight. Median FVC, FEV1, and PEFR were lowest in underweight and highest in overweight group. Weight had significant positive correlation with FVC, FEV1, and PEFR while BMI with FVC. Both weight and BMI negatively correlated with FEV1/FVC.
Conclusion: FVC, FEV1, and PEFR tend to increase while FEV1/FVC tends to decrease with increase in weight in adult healthy non-obese male.
KEY WORDS: Forced expiratory volume in 1 s, forced vital capacity, male, spirometry, weight.
Height correlates with lung size and is an important predictor of lung volumes.[1] Lung volume and capacities are larger in males and decrease with advancing age in both sexes.[2] Ethnic variations in values of different pulmonary parameters are also well-known.[3] There are reports of decrease in lung function in both under-nutrition and obesity. The initial increase in pulmonary function with increasing weight is due to increased muscle force while the decrease with further increase in weight is due to compromising mobility of the thoracic cage.[4]
Body mass index (BMI) is a simple tool for classifying individuals into underweight, normal, overweight, and obese. Reports on pulmonary function in overweight and obesity are conflicting. Some studies have found abnormal spirometry only in massively obese subjects. Others revealed altered spirometry in obese but not in overweight subjects. Decreased vital capacity has also been found in overweight group in one study.[5-7] This study was carried out in healthy young adult non-obese male subjects to evaluate the effect of increasing weight on dynamic spirometric parameters.
Approval from Institutional Ethics Committee was sought at first and permission for this crosssectional study was granted. Informed consent was taken from all the participants. Healthy non-obese young adult Bengali male subjects were recruited from among medical or paramedical students. Those with pre-existing respiratory diseases like asthma were excluded. Baseline and pulmonary parameters were recorded in a predesigned format. Height was measured in the standing posture to the nearest centimeter. Weight was measured to the nearest 0.1 kg from the zero reference point. BMI was calculated as weight in kilograms divided by the square of the height in meters.[8] The WHO criteria of classification of BMI were followed and BMI of <18.5 kg/m2 is considered as underweight, 18.5– 24.9 kg/m2 as normal weight, and 25.0–29.9 kg/m2 is considered as overweight.[9]
Digital spirometer (Spirowin version 2.0) was used to measure dynamic pulmonary parameters, namely, forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), FEV1/FVC ratio, forced expiratory flow between 25% and 75% of vital capacity (FEF25-75%), and peak expiratory flow rate (PEFR). Procedure of spirometry was demonstrated to the participants. After taking a maximal inspiration through the mouthpiece, they blew into it as quickly, forcefully, and maximally as possible, with nose manually closed. Criteria for acceptability and repeatability of spirometry as developed by American Thoracic Society were strictly followed.[10] At least three acceptable spirograms were obtained and spirometry was repeated until the two largest values of FVC were within 0.150 L of each other. Those with unacceptable spirometry or suspected to exert inadequate effort underwent a repeat spirometry on second or even third sitting. Maneuver with largest sum of FVC and forced FEV1 was taken for analysis and parameters were recorded.[10]
GraphPad Prism version 5 (San Diego, California: GraphPad Software Inc., 2007) was utilized for statistical analyses of data. One-way ANOVA followed by Tukey’s multiple comparison tests was used to compare the groups. P < 0.05 was considered as statistically significant. Correlation of weight and BMI with respiratory parameters was measured by Pearson’s test.
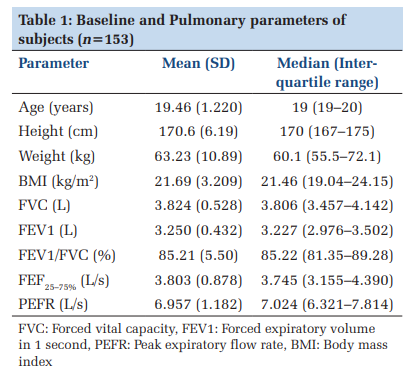
Out of 153 male subjects, 27 were underweight, 96 were normal, and 30 were overweight. Age of all the subjects ranged from 18 to 23 years. Their baseline and pulmonary parameters are shown in Table 1.
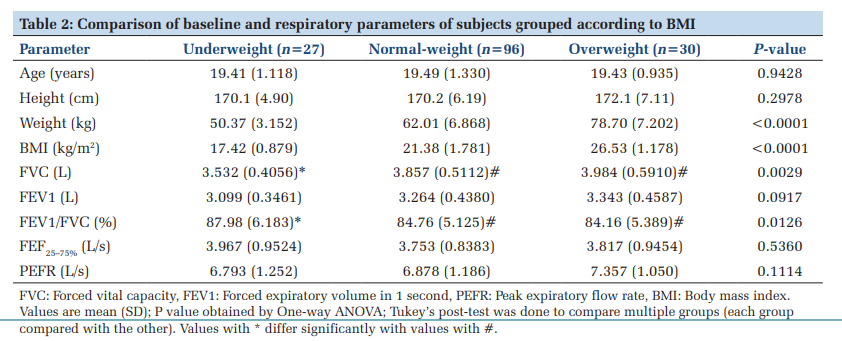
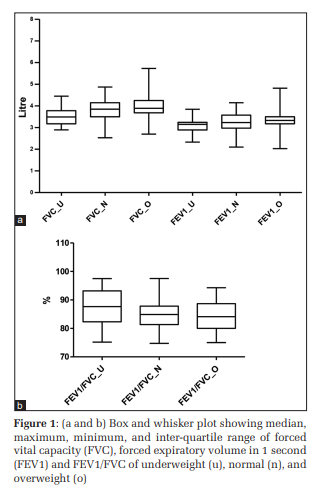
Table 2 compares the baseline and pulmonary parameters among three groups on the basis of BMI and shows the results of ANOVA. These groups were similar in age and height and differed significantly only in weight, BMI, FVC, and FEV1/ FVC. Tukey’s multiple comparison tests (not shown) revealed no significant difference between normal and overweight with respect to any pulmonary parameter. FVC and FEV1/FVC of normal weight group significantly differed with those of the underweight. The overweight group too differed significantly with the underweight with respect to FVC and FEV1/FVC. Median, minimum, maximum, and inter-quartile ranges of FVC, FEV1, and FEV1/ FVC of three groups have been depicted as box and whisker plot in Figure 1.
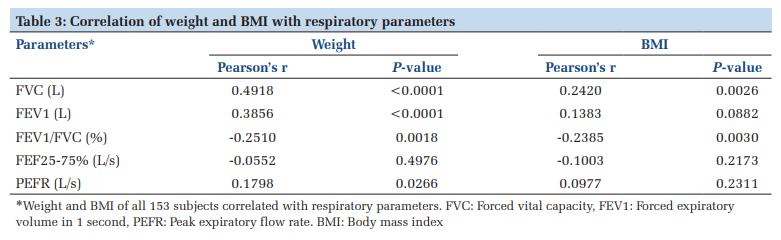
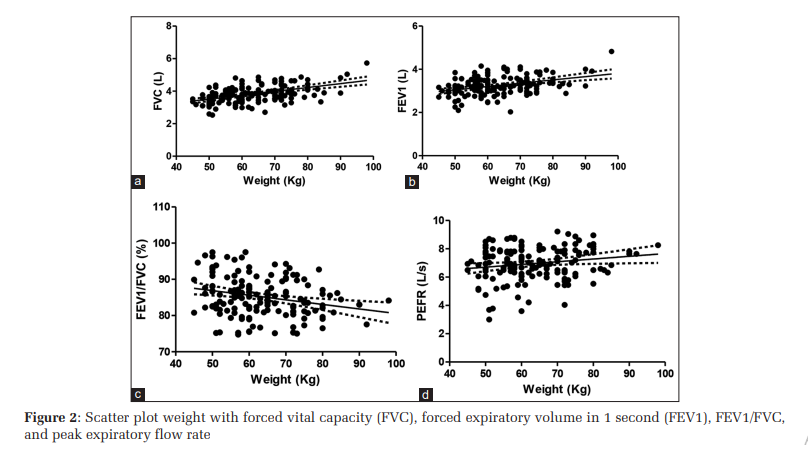
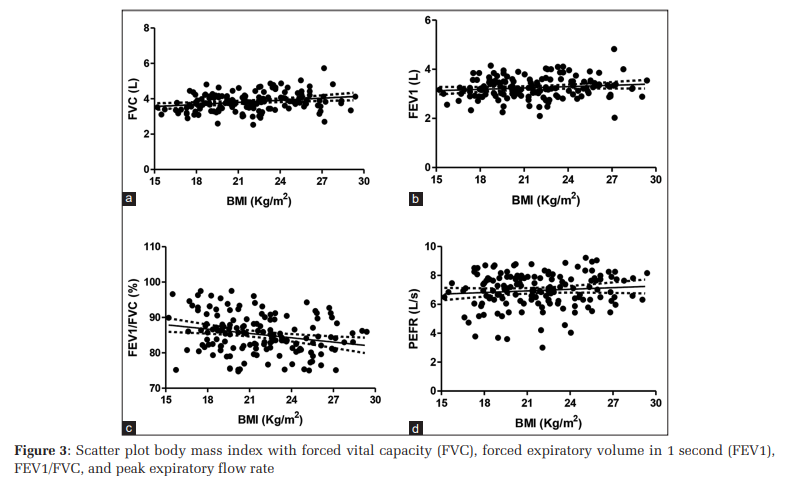
Correlations of weight and BMI with respiratory parameters are shown in Table 3. Both weight and BMI had significant correlation with FVC and FEV1/ FVC. Correlation of weight with FEV1 and PEFR was also significant and positive. The scatter plot of different pulmonary parameters with weight and BMI is depicted in Figures 2 and 3.
This study demonstrated decreased FVC, FEV1, and PEFR and increased FEV1/FVC in underweight group compared to normal subjects. Of these, only FVC and FEV1/FVC significantly differed. Overweight subjects had higher FVC, FEV1, and PEFR and the lower FEV1/FVC compared to normal but difference did not reach statistical significance. This may be due to the fact that overweight individuals were a small proportion (20%) of the total subjects. However, weight and BMI had significant linear relation with pulmonary parameters. Both weight and BMI had significant positive correlation with FVC and negative correlation with FEV1/FVC. Weight, in addition, positively correlated with FEV1 and PEFR.
Interaction of the lungs, the chest wall and respiratory muscles determine the respiratory mechanics. Lower lung volumes in underweight subjects have been reported in few earlier studies.[4,11] This may be due to decreased muscle mass which is often associated with a weaker diaphragm and other respiratory muscles and a decreased respiratory strength.[12] Our study also agrees with others who demonstrated no significant change in lung volume with increase in BMI.[13-15] Dynamic lung volumes and airflow are usually within normal limits even in mild obesity.[6,7,16,17] However, decrease in FVC with increasing BMI and adiposity has been found in some other studies.[18-20]
Lung volumes and airflow initially increase and then decrease with increase in weight. It has been suggested that the initial increase might be a sign of increasing muscle force, and the decrease with further weight gain may be due to obesity diminishing the mobility of the thoracic cage.[4] However, the point at which pulmonary function peaks and then starts to decline is hard to pin down. Our study indicates beneficial effect of increasing weight on FVC, FEV1, and PEFR in those having BMI up to 30. A study in children found elevated BMI increases lung volume but reduces airflow.[21] A recent meta-analysis indicates overweight and obesity is associated with lower FEV1/FVC.[22] This conforms to our finding of negative correlation of weight with FEV1/FVC.
The strength of this study lies in the fact that confounding effects of age, gender, and ethnicity were eliminated while measuring correlation of weight and BMI with lung parameters because subjects comprised male with similar age and of similar ethnic origin. Nonetheless, the smaller number of underweight and overweight subjects is a limitation of this study. It would have been better if total lung capacity (TLC) and diffusing capacity of lung for carbon monoxide (DLCO) could also be measured. However, our institution lacked the facility for measuring TLC and DLCO and these parameters could not be evaluated due to financial restraint.
FVC, FEV1, and PEFR tend to increase while FEV1/ FVC tends to decrease with increase in weight in non-obese male. A larger prospective study may be undertaken to correlate BMI with pulmonary function.
Subscribe now for latest articles and news.