Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i2.24.18
Year: 2024, Volume: 10, Issue: 2, Pages: 236-240
Case Report
Shalaka Khade1 , Sachin Chaudhari1 , Milind Bhatkule1 , Rasika Gadkari1
1Department of Pathology, All India Institute of Medical Sciences (AIIMS), Nagpur, India
Address for correspondence:
Sachin Chaudhari, Department of Pathology, All India Institute of Medical Sciences (AIIMS), Nagpur, India.
E-mail: [email protected]
Received Date:31 January 2024, Accepted Date:04 March 2024, Published Date:05 August 2024
Parapharyngeal space (PPS) neoplasms are relatively rare. Pleomorphic adenoma in the PPS can arise from the deep lobe of the parotid, however those arising de novo are extremely rare. Diagnosis and management of PPS lesions can be difficult due to the anatomic complexity of the space. A 47-year-old female came with swelling in the form of a bulge in the oral cavity on the right submandibular region. An intraoral fine needle aspiration cytology done from the mass revealed features of a benign salivary gland lesion, favouring Pleomorphic adenoma, which was confirmed on histopathology. Pleomorphic adenoma of PPS are rare tumors. FNAC along with careful clinical examination and radiological correlation can prove to be an imperative tool in diagnosis of PPS tumors and can aid in the appropriate management of these tumors.
Keywords: Parapharyngeal space, Pleomorphic adenoma, Cytology, Salivary glands, Neoplasms
Parapharyngeal space (PPS) neoplasms are relatively rare, accounting for about 0.5% of head and neck neoplasms 1, 2, 3. Most of these tumors arise from the salivary gland, comprising around 40-50% 2. Both benign and malignant neoplasms can arise in the parapharyngeal space, 70-80% being benign lesions 1. Pleomorphic adenoma in the PPS can arise from deep lobe of the parotid and extend through the stylomandibular tunnel into the PPS, however those arising de novo are extremely rare 2. Tumors of PPS are difficult to diagnose early due to absence of symptoms for a longer duration. Management of PPS lesions can be difficult due to the anatomic complexity of the space 4, 5. Though histopathology remains the gold standard for diagnosis, due to the difficult approach of tumors in this space, fine needle aspiration cytology (FNAC) has been proven to be helpful as a primary diagnostic tool, also in terms of cost and time 5.
Herein, we report a case of pleomorphic adenoma of the parapharyngeal space presenting with difficulty in swallowing, diagnosed based on intraoral fine needle aspiration cytology.
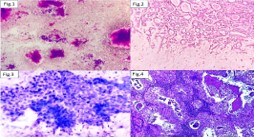
A 47-year-old female came to the Ear Nose Throat Out-patient department with a history of pain and difficulty in swallowing. Local examination revealed right peritonsillar bulge and 1x2cm hard swelling on the right side of the neck. No obvious submandibular swelling was seen clinically, but MRI suggested submandibular extension. MRI neck revealed a 5.2x5.8x4.3 cm mass in the right peritonsillar and parapharyngeal space. The lesion had sharp margins with the right tonsils being displaced anteriorly. It was seen displacing the carotid and internal jugular vein posteriorly and extending to involve the masticator and infratemporal space. However, no obvious sign of infiltration was seen, indicating a possible benign lesion. The rest of the neck spaces and salivary glands appeared distinct from Figure 1, Figure 2). Based on these features, a diagnosis of Benign salivary gland lesion, favouring Pleomorphic adenoma was given on FNAC. The patient further underwent an intraoral excision of the parapharyngeal mass under general anaesthesia. The tumor mass was received in bits and pieces aggregating to 4x4x3cm for histopathological examination. Sections showed relatively well circumscribed tumor. Tumor comprised of epithelial and stromal elements. Epithelial element was in the form of small tubules lined by cuboidal epithelium, surrounded by myoepithelial cells arranged in trabeculae, cords and having plasmacytoid appearance. Surrounding stroma was fibromyxoid to chondromyxoid and at places, hyalinised. Few small mucin cysts were also seen. Focally squamous metaplasia with keratin pearls was noted. There was no increased mitotic activity. Based upon these findings, a final diagnosis of Pleomorphic adenoma was given (Figure 3, Figure 4). The post-operative period was uneventful and the patient was stable at discharge.




The parapharyngeal space is an inverted pyramid shaped deep neck space having a skull base as the floor and greater cornu of the hyoid bone as the apex 6. Mass lesions of the parapharyngeal space account for only about 0.5% of all head and neck tumors 1. Majority of the tumors in this space are of salivary gland origin, accounting for 40-50% of cases and are located in the prestyloid PPS. Other tumors constitute neurogenic tumors and lymphoreticular lesions. The tumors of salivary gland origin can arise from the deep lobe of parotid, ectopic salivary rests in lymph node or minor salivary gland of lateral pharyngeal wall 2, 7.
The usual site of pleomorphic adenoma of minor salivary gland is the palate followed by the lip, buccal mucosa, floor of mouth, tongue, tonsil, pharynx, retromolar area and nasal cavity. Pleomorphic adenoma arising de novo in PPS is very unusual 2. Other tumors arising de novo in PPS are paragangliomas and schwannomas 8. Schwannoma accounts for about 20% of all PPS tumors. Paragangliomas at the head and neck region comprise of around 3% of all paragangliomas and almost all are located in the PPS 5.
Many of the lesions of the parapharyngeal spaces are usually detected incidentally as they are asymptomatic and painless 9. They grow slowly and remain silent for a long time. When the masses increase in size, they can present as palpable mass at the angle of mandible. Other symptoms can include change in voice, trismus, cranial nerve deficits and rarely obstructive sleep apnea 6. These tumors extend along the path of least resistance along the lateral pharyngeal wall, tonsillar fossa and submandibular triangle 9. Due to absence of symptoms for a longer time and the possibility of extension into hidden space like PPS, these lesions can grow for a long time before becoming symptomatic 3. This can increase the risk of malignant transformation over the years 4. In the present case, the patient had difficulty swallowing and swelling in the form of a bulge in the oral cavity in the right submandibular region. Meticulous intraoral examination and bimanual palpation are of importance as lesions of PPS can present many a time as intraoral swellings 10.
Direct examination of PPS lesions is not feasible due to difficulty in accessing the space for examination. Imaging studies including MRI and CT help in determining the extent of lesion and help the operating surgeon to plan the approach for surgery. MRI is said to be superior to CT as an investigation for PPS tumors 2. MRI is preferred to identify the extent of lesion and locate the adjacent vascular structures, while CT scan can identify bony involvement 9.
Fine needle aspiration cytology can be used as an easy and rapid modality of choice for early diagnosis of PPS tumors 11. It can be done percutaneously or intraorally, depending upon the location of the lesion. Intraoral FNAC can be done in the presence of intraoral lesion or bulge, as in this case where primary diagnosis was made on the basis of intraoral FNAC. Studies have shown FNAC diagnosis has around 92% accuracy rate, which can be improved further on combining it with imaging modalities 10. A study by Matsuki et al reported a correct diagnostic rate of 95.2% by FNAC 8. The diagnosis made on intraoral FNAC was confirmed after excision of tumor by histopathological examination. Use of FNAC in diagnosis can sometimes be challenging due to the localization of these lesions along with complex anatomy of the space and relationship with vascular and nervous structures. However, cytological examination still remains an important diagnostic modality to guide the surgeon in choosing the appropriate surgical approach and planning the extent of resection 3, 4, 12. FNAC can also be helpful in differentiating various tumors of the PPS. Cytology of Pleomorphic adenoma demonstrates fragments of chondromyxoid stroma along with spindle shaped cells with is characteristic.
Parapharyngeal space can be a common and first site of metastasis for tumors from nasal cavity, nasopharynx, palate and maxillary sinuses 5. Malignant salivary gland tumors like Adenoid cystic carcinoma and Carcinoma ex-pleomorphic adenoma are also documented at this site. In the presence of mixed population of benign cells and malignant epithelial cells along with stromal elements, a possibility of Carcinoma ex-pleomorphic adenoma should be considered 5. Other malignant tumors occurring at PPS include lymphoma, rhabdomyosarcoma, chordoma and undifferentiated sarcomas13.
Primary parapharyngeal tumors are rare with few cases published in literature. Shadab et al published a study comprising of 114 parapharyngeal tumors over a period of 27 years14.
Studies in literature have demonstrated that cytological diagnosis corroborated with the final histopathological diagnosis in maximum number of cases with few exceptions 5, 11, 13. Transoral tumor biopsies should be avoided to prevent the risk of recurrence by tumor capsule rupture 4.
The treatment of pleomorphic adenoma is mainly surgical resection 2, 5, 6. Despite being benign in nature, surgical resection with adequate margins is necessary to prevent recurrence of these lesions. Surgical procedures for PPS neoplasms can be difficult due to the complex anatomy of the space as well as deep location of the tumors 3.
Parapharyngeal space tumors are rare tumors, most of which are benign in nature and require careful preoperative assessment. Pleomorphic adenoma arising in the PPS de novo is a rare occurrence. FNAC along with careful clinical examination and radiological correlation can prove to be an imperative tool in diagnosis of PPS tumors, except for a few cases which need histopathological confirmation. It can also play an important role in planning appropriate management of these tumors.
SK and SC conceptualized the idea of the manuscript and were involved in drafting the manuscript. SC, MB and RG proofread the manuscript. All authors approved the final draft of the manuscript for publication.
Subscribe now for latest articles and news.