Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i2.23.24
Year: 2024, Volume: 10, Issue: 2, Pages: 219-222
Case Series
Nikhil Era1 , Samsuj Joha1 , Amar Kumar Gupta1 , Soni Kumari2 , Mala Mukherjee3 , Shatavisa Mukherjee4
1Department of Pharmacology, MGM Medical College and Hospital, Kishanganj, Bihar, India,
2Department of Dermatology, Geetanjali Medical College, Udaipur, Rajasthan, India,
3Department of Pathology, MGM Medical College and Hospital, Kishanganj, Bihar, India,
4Department of Clinical & Experimental Pharmacology, School of Tropical Medicine, Kolkata, West Bengal, India
Address for correspondence:
Shatavisa Mukherjee, Department of Clinical & Experimental Pharmacology, School of Tropical Medicine, Kolkata, West Bengal, India.
E-mail: [email protected]
Received Date:27 December 2023, Accepted Date:08 May 2024, Published Date:30 July 2024
Bullous haemorrhagic dermatosis (BHD), a distinctive non-immune cutaneous eruption, manifests as the formation of haemorrhagic bullae on the skin. While it is an uncommon dermatologic entity, its clinical significance is underscored by its association with various medications, including anticoagulants and antiplatelet agents, as well as chemotherapeutic drugs. Clinical or pathological signs of inflammation are usually absent. The pathophysiology of BHD involves the disruption of normal skin integrity, leading to the development of bullae containing blood. These bullae typically appear at sites distant from the initial lesion or injection site, posing challenges in diagnosis and management. Here we discuss three such cases and their presenting features.
Keywords: Bullous Haemorrhagic Dermatosis, Cutaneous Adverse Drug Reactions, Histopathology
Cutaneous adverse drug reactions (CADRs) refer to undesirable skin-related effects caused by the use of medications, with incidence varying widely depending on the specific drug, individual patient characteristics, and other factors. These reactions can manifest in various forms, including rashes, itching, blistering, and more severe conditions such as Stevens-Johnson syndrome or toxic epidermal necrolysis. The incidence of CADRs is challenging to pinpoint precisely due to factors like underreporting, variability in patient susceptibility, and differences in drug metabolism.
Bullous haemorrhagic dermatosis (BHD) is a rare cutaneous disorder characterized by the development of blisters and haemorrhagic lesions on the skin. Some medications have been associated with the development of bullous and haemorrhagic skin lesions like antithrombotic, antiplatelets, anticancer drugs. It is important to recognize that the association between drugs and bullous haemorrhagic dermatosis may not be well-established for all medications, and individual responses can vary.
BHD was first described in 2004 by Dyson et al. 1 The precise mechanism underlying BHD still remains unclear, although the suggested explanation involves delayed hypersensitivity, the administration of high doses of anticoagulants, and the presence of antibodies targeting heparin-platelet factor 4 (HPF-4). 2
Here we highlight three cases of BHD and their presenting features.
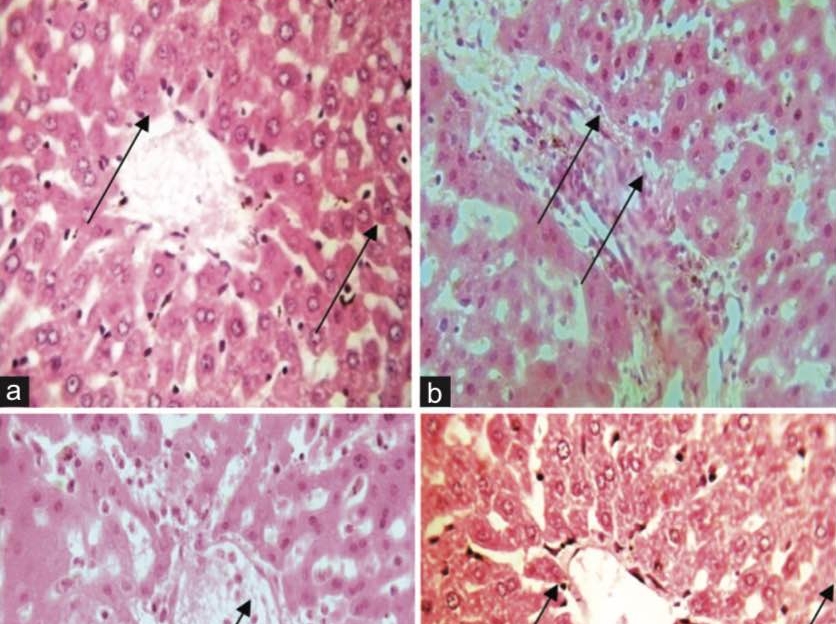
A 40-year-old woman was admitted for a fractured neck of the femur. She was prescribed enoxaparin 60mg subcutaneously every 12 hours for deep vein thrombosis prophylaxis. After 4 days, she developed multiple haemorrhagic abdominal blisters, with extension to other areas distant from the injection site. On examination, there were irregularly scattered, tense stable haemorrhagic bullae and vesicles Figure 1) Laboratory investigations conferred her coagulation values and his platelet count to be within normal range. A clinical diagnosis of enoxaparin-induced BHD was made and confirmed by punch biopsy. The histopathological examination (HPE) showed intraepidermal blisters containing red blood cells (RBCs), extravasated RBCs in the papillary dermis, and no signs of vasculitis or inflammatory infiltrate. (Figure 2) Enoxaparin was discontinued, and oral heparin was initiated. Subsequently, the lesions began to regress.


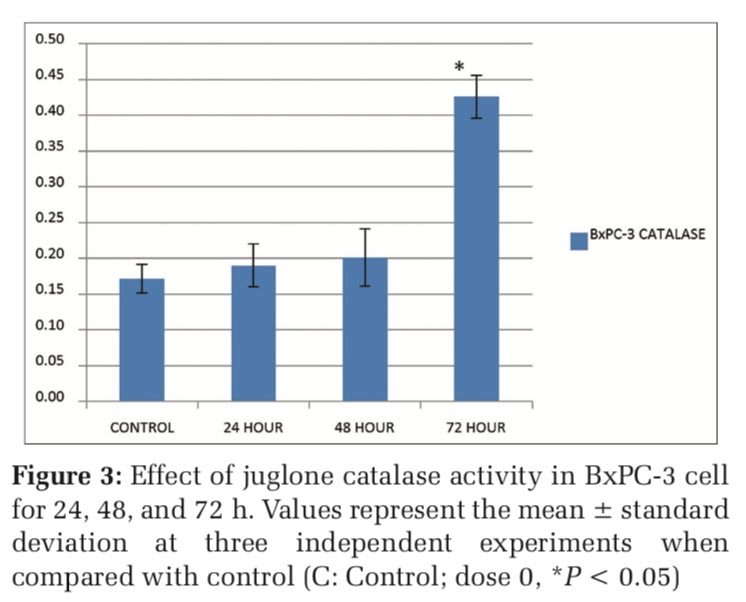
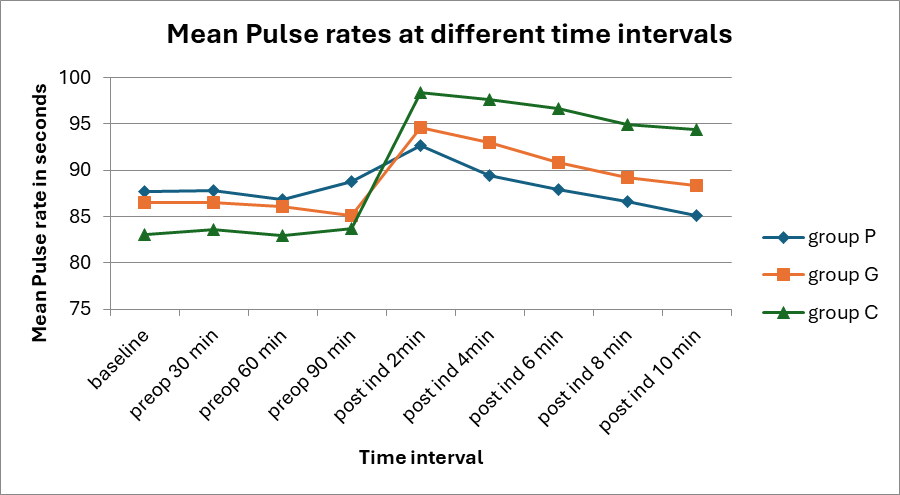
A 52-year-old patient with a history of coronary artery disease presented to the cardiac department with complaints of dizziness, syncope, and palpitations. An electrocardiogram (ECG) was performed, leading to the diagnosis of non-valvular atrial fibrillation. Subsequently, the patient was prescribed oral xarelto (rivaroxaban) 10 mg twice daily. One week later, the patient reported the development of small painful, tense, blood-filled blisters on the anterior abdominal wall extending to buttocks. (Figure 3) Histopathology of the lesions showed subcorneal blister, with mild spongiosis and dermal inflammatory infiltrate, confirming the diagnosis of BHD. (Figure 4) The implicated drug was promptly discontinued, and the patient was transitioned to apixaban, resulting in an uneventful recovery.


A 47-year-old man presented to the dermatology outpatient department with generalized haemorrhagic spots. Upon history elicitation, the patient disclosed receiving four tablets of aspirin (75mg each) from a local practitioner four days earlier due to sudden chest pain. Subsequently, the patient developed multiple blisters and hyperpigmented plaques with associated pain and itching, primarily affecting the upper trunk and umbilical area. (Figure 5) A diagnosis of BHD was confirmed through HPE. The patient was advised to discontinue aspirin and transitioned to clopidogrel. Following this change, the lesions gradually began to recover.
The causality assessment on applying WHO-UMC-causality assessment scale was found to be probable for all the three cases. The severity of the reactions were conferred to be moderate as per the Hartwig Seigel Scale. Preventability was assessed as ‘not preventable’ under Schumock Thornton Scale.

BHD, a rare and distinctive cutaneous disorder, manifests as the formation of haemorrhagic bullae on the skin. While it is an uncommon dermatologic entity, its clinical significance is underscored by its association with various medications, including anticoagulants and antiplatelet agents, as well as chemotherapeutic drugs. Clinical or pathological signs of inflammation are usually absent.
The pathophysiology of BHD involves the disruption of normal skin integrity, leading to the development of bullae containing blood. These bullae typically appear at sites distant from the initial lesion or injection site, posing challenges in diagnosis and management. The BHD lesions usually range from small to large size, dark haemorrhagic blisters, albeit they resemble clinically relevant entities of subepidermal blisters, such as necrotic skin or bullous vasculitis and pemphigoid and these lesions are characterized by urticarial plaques with pain 3 The diagnosis of BHD can be made by HPE which typically shows the presence of intraepidermal blisters filled with red blood cells 4
BHD typically develops around an average of 7 days, with a range of 3–270 days, after initiating the medication. 5, 6 It can also be associated with the use of dalteparin, warfarin, fondaparinux, and unfractionated heparin. Rakotonandrasana et al3 reported a case of 54-year-old male presented with BHD on the left upper limb surfacing 4 days after injection enoxaparin administration. Report from Chowdhury et al stated a case of 74-year-old female developing BHD at a distant site from subcutaneous delivery of enoxaparin.5 Switching over to alternative oral anticoagulants and prompt discontinuation of the implicated drug appears to be the only treatment modality in majority of the cases.
Recognizing the distinct features of BHD is crucial for healthcare professionals, as it aids in prompt diagnosis and the initiation of appropriate therapeutic interventions.
Dermatologists are likely to encounter these benign, self-limiting lesions which is more likely to be underdiagnosed in their practice, and thus should be aware of its favorable clinical course and through this case series, we aim to enhance awareness and understanding of this intriguing dermatologic condition
Source of Support: Nil
Conflict of Interest: The authors declare having no conflict of interest.
Acknowledgement: The authors acknowledge the contribution and untiring efforts of Pharmacovigilance Programme of India (PvPI) in ensuring patient safety nationwide.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Subscribe now for latest articles and news.