Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i2.24.104
Year: 2024, Volume: 10, Issue: 2, Pages: 175-182
Original Article
Mamta Yadav1 , Mani Bharti1 , Ashwini Kumar Nigam2 , Yofesh Goyal2 , Sahil Kumar Nautiyal3
1Assistant Professor, Government Institute of Medical Science, Greater Noida,
2Professor, Sarojini Naidu Medical College, Agra ,
3Professor, ESI Rohini, Delhi
Address for correspondence:
Mamta Yadav, Assistant Professor, Government Institute of Medical Science, Greater Noida. E-mail: [email protected]
Received Date:04 April 2024, Accepted Date:30 May 2024, Published Date:12 July 2024
Introduction: The escalation of community-acquired pneumonia cases amidst the COVID-19 pandemic has engendered a concerning phenomenon characterized by the unwarranted utilization of antimicrobial agents. Aims: To analyze the utilization trends of antimicrobial agents within the cohort of hospitalized individuals diagnosed with community-acquired pneumonia (CAP). Material and methods: A prospective observational study was conducted for 6 months within the Department of Medicine to investigate patients diagnosed with CAP. Detailed records of drug prescriptions were meticulously recorded, with subsequent computation of both the Daily Defined Dose (DDD) and Antibiotics Consumption Index (ACI). A dataset comprising information from 130 patients was meticulously examined and subsequent analysis conducted. Descriptive statistical analyses were undertaken to utilize both Microsoft Excel and SPSS software version 27. Results: The predominant empirical therapy for antibacterial agents was found to be amoxicillin-clavulanic acid, utilized by 73 (56.2%) patients, succeeded by levofloxacin, administered to 33 (25.4%) patients. Following culture and sensitivity testing, the most frequently employed antibacterial agents for definitive therapy included levofloxacin for 33 (25.4%) patients. Notably, the highest Antibiotics Consumption Index (ACI) value recorded was 14.4 for amoxicillin-clavulanic acid in empirical therapy, while in definitive therapy, levofloxacin exhibited an ACI of 14.8. A significant disparity in ACI values between empirical and definitive therapy was observed (p<0.05), signifying statistically meaningful differences. Conclusions: The findings of the current investigation accentuate a discernible trend in the administration of antibiotics for managing community-acquired pneumonia (CAP) within the Medicine Department amidst the COVID-19 pandemic.
Keywords: Community Acquired Pneumonia (Cap), Antibiotics Consumption Index (Aci), Defined Daily Dose, Antimicrobial Utilization Pattern, Antimicrobial Agents
Community-acquired pneumonia (CAP) represents a significant public health concern globally, posing a substantial threat to individuals across diverse geographical and socioeconomic landscapes. This infectious respiratory condition stands as a prominent cause of both hospitalization and mortality among adult populations, exerting its impact not only in developing nations but also in more economically advanced societies 1, 2. Physicians and patients frequently underestimate the gravity of community-acquired pneumonia 3. The World Health Organization (WHO) advocates for the utilization of indicators to monitor trends in antibiotic usage, facilitating local agencies in pinpointing shortcomings and focal points for intervention 2. The growing danger of antimicrobial resistance complicates CAP therapy, as does the propensity to focus on empirical therapy. Drug Utilization (DU) has emerged as a distinct research domain, facilitating rigorous examination of drug prescription and consumption patterns through systematic and formal methodologies. Such investigations illuminate the quality of drug prescribing practices, often assessed through predefined criteria such as the Defined Daily Dose (DDD) 4. The utilization of DDD confers several advantages for objective evaluation, encompassing standardization, simplification, comparability, and trend analysis. This metric is instrumental in drug utilization studies, enabling the quantification and comparative assessment of medication consumption across various therapeutic agents 5.
This study holds promise for evaluating the prescription patterns of antibacterial agents utilized in the management of CAP. Furthermore, our observations have elucidated a direct correlation between alterations in medication regimens and the progression of the disease. Such insights are invaluable for formulating guidelines tailored to the disease profile of CAP within our tertiary care facility.
The collaborative research was undertaken for six months, from September 2019 to March 2020, and involved the Departments of Medicine and Pharmacology at Sarojini Naidu Medical College and Associated Hospital situated in Agra, Uttar Pradesh. Approval for the study was obtained from the Scientific Review Board and the Institutional Ethics Committee (IEC). The study was also registered in the Clinical Trials Registry India (CTRI) under approval number CTRI/2018/02/011788. It was designed as an observational, prospective, and qualitative study of antibacterial drug utilization. Eligible participants were patients admitted to the medicine department with a diagnosis of community-acquired pneumonia who were receiving antibacterial agents. They were enrolled and followed up from admission to discharge. Written informed consent was obtained from each participant upon enrollment. Patient records were collected at admission for empirical therapy, on the third day after medication change following sensitivity testing, and until discharge. All patients of both sexes and ages above 18 years were included. Exclusion criteria included patients already undergoing antimicrobial treatment for more than 7 days, patients with ventilator-associated pneumonia, immunocompromised patients, patients diagnosed with lung cancers, and individuals with tuberculosis. Out of a total of 166 patients initially enrolled, 24 discontinued treatment prematurely, and 12 succumbed during treatment. Therefore, prescription records of 130 patients were analyzed over six months. Medication prescriptions were documented using the International Anatomical Therapeutic Chemical Classification Scheme (ATC). Consumption of antimicrobial agents was assessed utilizing the ATC-DDD classification system.
The Defined Daily Dose (DDD) represents the standard average maintenance dosage of a medication utilized in adults for its primary indication. For drugs with an existing Anatomical Therapeutic Chemical (ATC) code, a specific DDD has been allocated.
Number of DDDs = Total grams used / DDD values in grams
DDD/bed-day x 100 = Antimicrobial consumption index (ACI). The number obtained is the hospital's antibiotic consumption index for CAP. Quantifying antibiotic usage through the Antimicrobial Consumption Index (ACI) enables hospitals to compare their antibiotic consumption levels with those of other institutions, irrespective of variations in formulary composition, antibiotic potency, and hospital census 7. The collected data was statistically analyzed through SPSS version 27. Descriptive data were presented as percentages or the mean ± standard deviation.
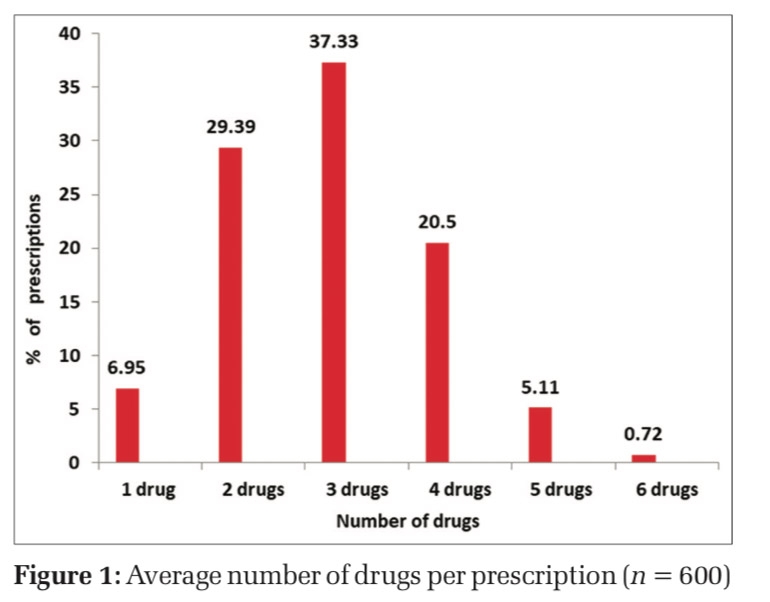
Patients included in the study belong to the 21-90 year age group. The mean age of individuals diagnosed with community-acquired pneumonia was 63.65 ± 11.54 years. Among the patients presenting with community-acquired pneumonia, a majority were male, constituting 96 (73.8%), while approximately 34 (26.3%) were female shown in Figure 1.
The empirical therapy most commonly prescribed for antibacterial treatment consisted of amoxicillin-clavulanic acid, administered to 73 (56.2%) patients, followed by levofloxacin for 33 (25.4%) patients, ceftriaxone for 16 (12.3%) patients, ofloxacin for 6 (4.6%) patients, and piperacillin-tazobactam for 2(1.5%) patients.
As definitive therapy, the most frequently utilized antibacterial agents included levofloxacin, [prescribed for 33 (25.4%) patients, azithromycin for 9 (6.9%) patients, and vancomycin for 5 (3.8%) patients. Less commonly used agents included linezolid, cefoperazone, and moxifloxacin, each administered to 1 (0.8%) patients.
The highest antibiotics Consumption Index (ACI) value observed for empirical therapy was 14.4, attributed to amoxicillin-clavulanic acid, followed by azithromycin with an ACI of 12.6. In contrast for definitive therapy, levofloxacin exhibited the highest ACI of 14.8, followed by meropenem with an ACI of 13.0 (Table 1). A statistical comparison of empirical and definitive therapies regarding the antibiotic consumption index revealed a p-value less than 0.05. This indicates a statistically significant difference in antibiotics consumption between the two therapies. The difference was calculated using a paired Student’s t-test (Figure 3, Figure 4).
Five pathogens were isolated via sputum culture, with Streptococcus pneumoniae being the most prevalent, affecting 50 (38.4%) patients. Following this, K. pneumoniae was identified in 34 (26.1%) patients, Escherichia coli in 29 (22.3%) patients, Staphylococcus aureus in 12 (9.2%) patients, and Pseudomonas in 5 (3.8%) patients (Figure 2)
In the management of Community-Acquired Pneumonia (CAP), the most commonly prescribed combinations of antimicrobials were amoxicillin-clavulanic acid in conjunction with azithromycin, accounting for 31 (43%) of cases in empirical and 14 (32.5%) in definitive therapy. Conversely, the least frequently utilized combination was amoxicillin-clavulanic acid combined with amikacin, constituting only 2.3% of cases. Overall, multiple antimicrobial prescriptions were observed in 115 cases (88.4%), Figure 5.
The hospital stay duration ranged from a minimum of 3 days to a maximum of 12 days, with a mean duration of 7.35 ± 1.63 days. The mean duration of empirical therapy was 3.42 ± 0.80 days, while that of definitive therapy was 4.47 ± 0.87 days.
The average number of drugs prescribed per prescription was 7.67 ± 2.17, with an average of 2.66 ± 1.89 antibiotics per prescription. Approximately 41 (32%) of drugs were prescribed using their generic names. On average, 89 (93.5%) of prescriptions included injections.
Community-acquired pneumonia is the predominant cause of hospital admissions among infectious diseases. Antimicrobial agents constitute the primary treatment approach empirically and upon confirmation of microbial pathogens. Nonetheless, their utilization has raised concerns due to instances of overuse and misuse, leading to adverse drug reactions, emergence of drug resistance, prolonged hospital stays, and escalated therapy costs 8. This study seeks to delineate the prevailing trends and extent of antibacterial utilization in patients diagnosed with Community-Acquired Pneumonia at Sarojini Naidu Medical College in Agra.
In this study, the highest proportion of cases (35.4%) fell within the age bracket of 61-70 years. The mean age of patients was recorded as 63.65 ± 11.54 years. Notably, approximately 72 cases were aged over 65 years, meeting one of the admission criteria for CAP patients. Studies conducted by Menon et al. and Shah et al. have consistently demonstrated that the highest incidence of Community-Acquired Pneumonia occurs in patients aged over 60 years 9, 10. The extremes of age are associated with lower immunity and an increased prevalence of predisposing risk factors, which contribute to multi-organ failure. This susceptibility to multi-organ failure is often attributed to the predisposition associated with old age.





|
Drug |
ATC code |
DDD (gm) |
ACI=DDD/100 bed - days (empirical therapy) |
ACI=DDD/100 bed - days (definitive therapy) |
|
Penicillin – Amoxicillin-clavulanic acid (O), Amoxicillin-clavulanic acid (P), Piperacillin-tazobactam |
J01CR50 - J01CA12 |
1 3 14 |
- 14.4 0.135 |
5.52 - 0.90 |
|
Cephalosporins Ceftriaxone Cefoperazone |
J01DD04 J01DD12 |
2 4 |
0.94 - |
6.17 0.10 |
|
Macrolide Azithromycin, (O) Clarithromycin (O) |
J01FA10 J01FA09 |
0.3 0.5 |
12.6 - |
5.14 0.94 |
|
Flouroquinolones Ofloxacin Levofloxacin Moxifloxacin |
J01MA01 J01MA12 J01MA14 |
0.4 0.5 0.4 |
0.62 6.47 - |
1.6 14.8 0.15 |
|
Tetracycline doxycycline |
J01AAO2 |
- |
- |
0.18 |
|
Aminoglycoside Amikacin |
J01GB06 |
1 |
- |
0.83 |
|
Carbapenem Meropenem |
J01DH02 |
2 |
0.18 |
13.0 |
|
Vancomycin |
J01XA01 |
2 |
- |
2.40 |
|
Linezolid |
J01XX08 |
1.2 |
- |
0.15 |
O= oral, P= Parental, ATC Code- International Anatomical Therapeutic Chemical Classification Scheme (ATC), DDD- Defined Daily Dose
|
Countries |
Antimicrobial prescribing |
Microbiological confirmation |
Adherence to guidelines |
Study |
|
Norway (2016, 2021) |
Narrow spectrum beta lactam -54% Fluroquninolones- 12% broad-spectrum cefotaxime, ceftriaxone- 34% |
S. pneumoniae- 23.8% H. influenza - 22.4% M. catarrhalis - 11.9% |
56.2% adhere to CAP norwegian guidelines |
Waagsbø et al. BMC Pulmonary Medicine (2022) 22:379 |
|
Malaysia (2022) |
Narrow spectrum beta lactam- 52.6% |
Not specified |
60.8% adherence to guidelines |
Loong et al. – Appropriateness of antimicrobial prescribing , J Infect Dev Ctries 2022; 16(12):1877-1886 |
|
Netherlands (2015) |
beta-lactam- 57% beta-lactam–macrolide- 20.8% fluoroquinolone-22.3% |
NA |
72.8% adherence to guidelines |
Antibiotic Treatment for Community-Acquired Pneumonia, n engl j med 372;14 |
The table shows different studies from other countries for comparison of CAP patients prescribing pattern of antibiotics along with microbial pathogen identified and adherence to the guidelines of that country.
|
Indicators |
Mean ±S.D. / percentage |
|
Average number of drugs per prescription(encounter) |
7.67±2.17 |
|
Average number of antibiotics per prescription |
2.66±1.89 |
|
Percentage of drugs prescribed by generic name |
32% |
|
Average number of prescription with injection |
93.5% |
The predominant approach to treatment in CAP largely relies on observational methods, emphasizing clinical and radiological diagnoses of the most prevalent causative pathogens. However, CAP remains a considerable public health concern. Therefore, it is imperative that antimicrobial treatment strategies be tailored to align with the distribution and prevalence of etiological pathogens within the population. Resistance trends at the local, national, and international levels, alongside prior exposure, must all be carefully weighed in antimicrobial decision-making. Additionally, the decision regarding hospitalization is guided by prognostic criteria, ensuring optimal management of patients with Community-Acquired Pneumonia. The results of this study reveal that amoxicillin-clavulanic acid combined with azithromycin (56.2%) and levofloxacin (25.4%) were the most commonly prescribed empirical therapy antibiotics. Interestingly, a study by Kotwani et al. conducted in Delhi over five years reported a similar trend, with two antimicrobials from the same drug class being prescribed to the majority of patients. Moreover, Nayar et al. found in their study a preference for the combination of beta-lactam and macrolide antibiotics, particularly ceftriaxone and azithromycin. These findings align closely with our study's observations regarding prescribed antibiotics 11, 12.
To compare the data with antimicrobial prescribing practices for patients with community-acquired pneumonia (CAP) in various countries, including those in Europe, Norway, and Malaysia. The studies found frequent non-adherence to national clinical practice guidelines, especially concerning empirical regimens in non-severe CAP, timely de-escalation to targeted therapy, transition to oral regimens, and overall therapy duration 13. There was a notable initiation and continuation of broad-spectrum antimicrobial therapy without a documented rationale. This was partly due to clinical improvement observed while on broad-spectrum regimens, even when microbiological tests did not confirm the necessity for such broad-spectrum coverage 14. These studies concluded that there is a need for better antimicrobial de-escalation strategies and continuous focus on improving microbiological diagnostics and adherence to guideline-recommended therapies. Table 2 shows the comparison of the studies from different countries.
Following the receipt of culture and sensitivity reports, definitive therapy was promptly initiated for targeted treatment based on the identified organism. It was noted that a significant number of cases of S. pneumoniae and K. pneumoniae exhibited resistance to first-line treatments, necessitating a shift to higher classes of antibiotics to which the organisms remained sensitive 13. Consequently, in this study, the most commonly prescribed drugs included levofloxacin (25.4%), ceftriaxone (19.2%), meropenem (13.8%), azithromycin (6.9%), amoxicillin-clavulanic acid, vancomycin, piperacillin-tazobactam, amikacin, clarithromycin, doxycycline, and cefoperazone. These findings align closely with those of the Kotwani et al. study, wherein cephalosporins followed by macrolides emerged as the most commonly prescribed antimicrobials, resembling the pattern observed in our study. Moreover, in the present study, antimicrobial agents were utilized empirically in 55.3% and as definitive therapy in 33.0% of patients, a pattern comparable to that reported in the Kotwani et al. study 11.
The total duration of antimicrobial therapy as definitive treatment for hospitalized patients in this study was 4.47 ± 0.87 days, while the overall length of hospital stay was 7.35 ± 1.63 days. Interestingly, these findings closely mirror those reported in studies conducted by Kotwani et al. and Nayar et al. 11, 12.
Indeed, the route of administration of antimicrobial agents (AMAs) is typically determined by several factors, including the site and severity of the infection 15, 16. In this study, a majority of antimicrobials were administered intravenously (76.2%), while medications such as clarithromycin, ofloxacin, and azithromycin were given orally (23.8%) as definitive therapy. A study by Cyriac et al. delves into the policy regarding changing the route of drug administration 17. In 72.3% of patients, a combination of antimicrobial agents (AMAs) was utilized. Amikacin was included in cases of gram-negative infections to enhance the synergistic prolongation of the post-antibiotic effect of beta-lactams. However, the concurrent use of ceftriaxone with amoxicillin-clavulanic acid and piperacillin with carbapenems may not be deemed rational, as there is no documented advantage with these combinations. In this study, the most frequently employed combinations included amoxicillin-clavulanic acid with either azithromycin or levofloxacin. A similar pattern of fixed-dose combination (FDC) prescription was observed in the study conducted by Mahajan et al. 18. Beta-lactam in combination with fluoroquinolones and macrolides was prescribed in 4.1% of patients. Additionally, fluoroquinolones paired with cephalosporins in 11% of patients were noted as being irrationally prescribed in empirical treatment.
In this study, the average number of drugs prescribed per patient was 7.67 ± 2.1, with an average of 2.66 ± 1.86 antibiotics per prescription. A critical indicator of prescription quality is the average number of medications per prescription. It is generally recommended to minimize this number as much as possible, as higher numbers often correlate with increased risks of drug interactions, bacterial resistance, and elevated hospital costs. Upon thorough screening of prescriptions, it was observed that mono-antibiotic prescriptions accounted for 35 (15.3%) instances, while poly-antibiotic therapy was prescribed in 195 (84.7%) cases. This presentation underscores the prevalence of poly-antibiotic prescriptions over mono-antibiotic therapy. Studies conducted by Mehrad et al. in 2015 and Bala et al. in 2009 demonstrated similar prescribing indicators 19, 20.
In our study, approximately 32% of drugs were prescribed using their generic names, with the majority of medications being prescribed by brand names. However, it is noteworthy that prescribing medications by their generic names can facilitate better inventory monitoring by the hospital pharmacy. A study conducted by Mittal et al. revealed a similar pattern of prescribing, highlighting the importance of this practice in optimizing healthcare management 21. The average number of prescriptions involving intravenous (IV) antimicrobials was 93.5%. Despite the feasibility of an oral route, the majority of inpatients receive IV antibiotics for an extended duration 22, 23.
Data on drug consumption was quantified in terms of fixed daily doses (DDD) per 100 bed days. Amoxicillin-clavulanic acid exhibited the highest value of 14.45 DDD per 100 bed days, indicating its status as the most commonly used broad-spectrum antibiotic, followed by azithromycin with a value of 12.6 DDD per 100 bed days in empirical therapy. In definitive therapy, the highest value was recorded for levofloxacin at 14.85 DDD per 100 bed days, followed by meropenem with a value of 13.0 DDD per 100 bed days. This pattern of drug utilization observed in our study aligns with findings reported by Ravi et al. in the Himalayan region of northern India and Charave et al. in Karnataka in 2020 24, 25. The consumption of antibiotics as definitive therapy was strongly correlated with the culture sensitivity report, with an overall DDD of 52.24 compared to 35.34 DDD/100 bed days for empirical therapy. This association can be attributed to the resistance observed against first-line drugs for CAP. Consequently, patients had to transition to higher-class antibiotics, resulting in increased consumption of DDD 26. The findings of this study were consistent with those of the study conducted by Naik et al., wherein patients in the medicine department exhibited increased consumption of antibiotics following the receipt of culture reports 27.
This research offers valuable insights into the prescribing patterns of antimicrobial agents (AMAs), which can serve as a foundation for designing intervention studies aimed at promoting rational drug utilization. The findings of this study shed light on the typical patterns of antibiotic usage in Community-Acquired Pneumonia (CAP) within medicine departments. However, antibiotic resistance presents a pressing challenge for the medical community, with overuse and misuse of antibiotics being significant contributing factors. The study gives a dearth of data on antimicrobial usage patterns in our community, particularly in Sarojini Naidu Medical College, Agra. Drug Utilization Studies should be conducted across various departments to assess antibiotic utilization comprehensively. An effective prescription program should advocate for the prudent use of reserve antibiotics and the efficient management of limited resources.
Subscribe now for latest articles and news.