Journal of Medical Sciences and Health
Year: 2023, Volume: 9, Issue: 2, Pages: 233-236
Case Report
Neha Sharad1 , Smriti Srivastava1 , Purva Mathur2 , Rajesh Malhotra3
1Senior Resident, Department of Microbiology, AIIMS, New Delhi, India,
2Professor, Department of laboratory Medicine, JPNATC, AIIMS, New Delhi, India,
3Professor, Department of Orthopaedics, AIIMS, New Delhi, India
Address for correspondence:
Purva Mathur, Professor, Department of laboratory Medicine, JPNATC, AIIMS, New Delhi, India.
E-mail: [email protected]
Received Date:03 February 2022, Accepted Date:22 May 2022, Published Date:26 September 2023
Invasive Fungal Infections have posed a difficult challenge in the recovery of people infected with COVID-19. COVID-19-associated pulmonary aspergillosis (CAPA) has been described and found in about 30 % of ICU patients worldwide. Here we present an unusual microscopic finding in a case of CAPA in an ICU patient which was helpful in initiating early definite therapy. A 56-year-old gentleman presented with complaints of fever and shortness of breath and subsequently tested positive for COVID. Post admission, his respiratory distress worsened and his condition deteriorated. A provisional diagnosis of COVID pneumonia with acute respiratory distress syndrome (ARDS) was established based on chest radiographic finding of left lower lobe consolidation, increased pulmonary infiltrates in bilateral lung fields with evidence of pleural effusion. Pleural Aspirate obtained via ultrasound guided thoracocentesis revealed branched hyaline septate hyphae along with structures which were composed of elongated vesicle with one layer of phialides covering two-thirds of the vesicle and bearing globose conidia on KOH direct mount. Aspergillus flavus grew on culture, which was later confirmed by MALDI TOF VITEK MS. Patient was diagnosed with Proven Invasive Pulmonary Aspergillosis with COVID-19 and voriconazole was started. Patient successfully recovered and was discharged. Identifying the Aspergillus species directly on the basis of KOH Mount, helped in decreasing the turnaround time, in early initiation of definite therapy and possibly contributed to the favorable outcome. CAPA is a potentially life-threatening complication in patients with severe COVID-19, thus a timely diagnosis and treatment becomes crucial in the management.
Keywords: CAPA, COVID-19, Aspergillus
With the onset of Coronavirus disease 2019 (COVID-19), we were ushered in an unprecedented era. Two years later, we are still struggling to cope with pandemic, with each new wave bringing a new challenge, Co-infections in these patients challenge the recovery further. Secondary infections can easily go undiagnosed in the face of a SARS-CoV-2 primary infection, especially if symptoms overlap, diligent testing for other infectious diseases is vital.
People with COVID-19 sometimes present with acute respiratory distress syndrome (ARDS) and are usually admitted to ICUs and frequently receive broad-spectrum antibiotics along with corticosteroids and immunomodulatory agents, predisposing to Invasive fungal infections, common amongst them being Aspergillosis, Candidiasis and Mucormycosis. Diagnosing these fungal pathogens is vital to reduce delays in antifungal treatment.
COVID-19-associated pulmonary aspergillosis (CAPA) has been described and found in 19.6-33.3 % of Intensive Care Unit (ICU) patients worldwide. 1 Risk Factors for CAPA include severe COVID-19, patients in ICUs or on ventilators. It is difficult to diagnose as patients often have non-specific symptoms and appropriate sample is not easily obtained for microbiological analysis, it can lead to severe illness and death. 2, 3, 4, 5.
We came across a patient of CAPA in our ICU, whoselab findings revealed an unusual structure and assisted in rapid identification of the causative agent and was helpful in initiating early definite therapy.
A 56-year-old gentleman was admitted to the Covid dedicated facility of a tertiary care centre in North India in May 2021. He had presented with complaints of fever and shortness of breath and subsequently tested positive for COVID. He was a known hypertensive and diabetic with history of coronary artery disease bypass graft for chronic stable angina. Post admission, his respiratory distress worsened and his condition deteriorated. In view of worsening respiratory distress and fall in saturation he was given Oxygen with high flow nasal cannula. His chest radiograph revealed left lower lobe consolidation and increased pulmonary infiltrates in bilateral lung fields with evidence of pleural effusion. A provisional diagnosis of COVID pneumonia with acute respiratory distress syndrome (ARDS) was established. He underwent ultrasound guided thoracocentesis and the aspirate was sent to our lab for bacterial and fungal evaluation.
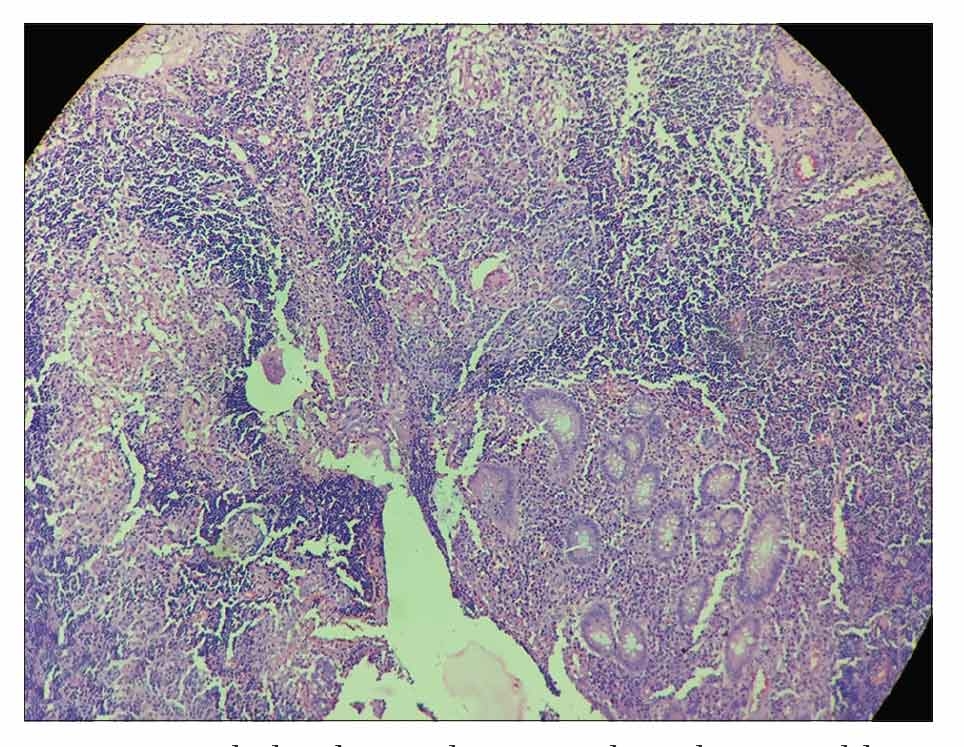
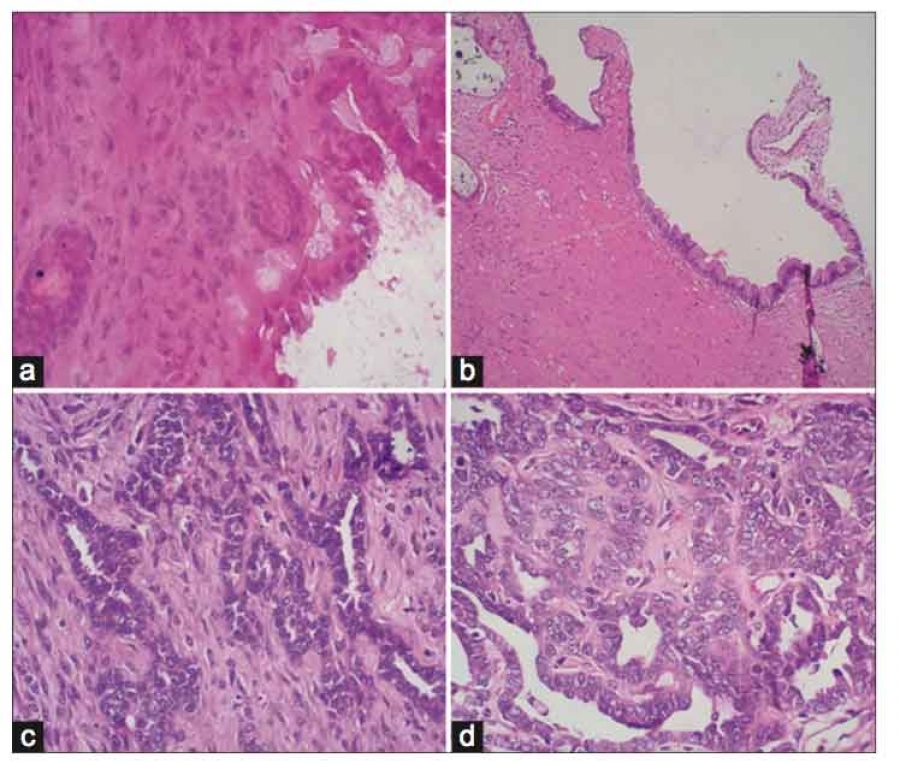
KOH microscopy revealed branched hyaline septate hyphae along with structures which were composed of elongated vesicle with one layer of phialides covering two-thirds of the vesicle and bearing globose conidia. Culture on Sabouraud dextrose agar grew yellowish green colonies on obverse side and the reverse was non-pigmented, seven days after inoculation. Lacto-phenol cotton blue mount from the culture was prepared. A repeat sample was received three (3) days later, similar findings were obtained from the repeat sample. We were able to rule out contamination as identical findings were obtained from two consequent clinical samples and the sample was ultrasound guided further decreasing chances of contamination. Bacterial cultures were sterile.

The structures seen on microscopy were tentatively identified as the fruiting bodies of Aspergillus flavus and based on culture findings, isolate was identified as Aspergillus flavus. We confirmed our isolate as Aspergillus flavus/oryzae using MALDI-TOF VITEK MS (Biomerieux, Marcy-I’Etoile, France), as per standard methodology used for fungal isolates.6 The complete blood count revealed leucocytosis, with normal neutrophil count. The patient also had sepsis with coagulopathy with an INR of 2.09 on the day of thoracocentesis. Due to coagulopathy, biopsy samples could not be obtained. 7
The patient was diagnosed as a case of Proven Invasive Pulmonary Aspergillosis 8, the same was informed to the treating team and intravenous voriconazole was added to the treatment regime. The patient successfully recovered and was subsequently discharged in July 2021. Informed consent was taken in written from the patient for the publication.
Awareness to secondary fungal infections in COVID-19 patients has increased many-fold in comparison to in beginning of the pandemic and it is essential to reduce delays in diagnosis and treatment in order to help prevent severe illness and adverse outcome from these infections.
In cases of Aspergillus infection, hyaline septate hyphae are seen on KOH mounts and fungal culture shows characteristic macroscopic colony growth. Fruiting body of Aspergillus is a rare sighting in clinical samples on microscopy, in cases reported in literature where fruiting bodies were seen, it was from tissue sections obtained from pulmonary cavities, external auditory canal, nasal cavity and skin biopsy. 9
The morphology of the fruiting body helps in species identification, it is composed of a vesicle and one or two layers of phialides which produce conidia. Fruiting bodies of Aspergillus species develop in areas of high oxygen tension, or severe infections. 10 In A. fumigatus, there is presence of a single row of phialides mainly over the upper one-third of the vesicle whereas in A. flavus there can be either one or two row of phialides covering the entire vesicle.
The diagnosis of Aspergillosis in humans is based on the clinical, radiological and microscopic findings. 10 The predisposing conditions in our patient for invasive Aspergillosis included poorly controlled diabetes mellitus, Covid-19 infection which is now known to cause immune dysregulation and ICU admission. 8, 11 Presence of septate hyphae in a KOH Mount helps in starting treatment empirically, covering the most common etiological agents. But if an identifying structure of Aspergillus species is seen, we can immediately start with the definite treatment. In routine practice, fungi take up to 4-6 weeks to grow and some may even not grow on culture, based on such findings, the appropriate treatment can be started immediately. Like if the causative agent is Fusarium, some species of Fusarium are non-responsive to Tri-azoles and Amphotericin B is the drug of choice, whereas azoles form the first line of therapy for Aspergillus species. 12, 13 Hence the presence of fruiting body can go a long way in immediate start of appropriate therapy and thus if we get a fruiting body on direct KOH Mount, it shouldn’t be overlooked. CAPA is considered a serious and potentially life-threatening complication in patients with severe COVID-19, thus a timely diagnosis and treatment becomes pivotal in the management.
COVID-19- Coronavirus disease 19; ICU- Intensive Care Unit; CAPA- Covid-19 associated Pulmonary Aspergillosis; ARDS- Acute Respiratory Distress Syndrome; MALDI-TOF- Matrix Assisted Laser Desorption Ionisation-Time of Flight
Subscribe now for latest articles and news.