Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.011
Year: 2021, Volume: 7, Issue: 2, Pages: 67-73
Original Article
U Geethalakshmi1 , S Rupashree1 , K Ramesh Babu2
1 Associate Professsor, Department of Pathology, Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India,
2 Professsor and Head, Department of Pathology, Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India
Address for correspondence:
Dr. S Rupashree, Associate Professsor, Department of Pathology, Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India. Phone: +91-9448182821. E-mail: [email protected]
Introduction: Salivary gland swellings are common entity and annual incidence of tumors is 0.5–13.5% per 1 lakh population worldwide. Imaging and aspiration cytology have limited role in accurately diagnosing salivary lesions and hence microscopic diagnosis is essential.
Aims and objectives: The aim of the study was to study frequency and histomorphological pattern of salivary gland lesions.
Material and Methods: A retrospective study conducted (from January 2017 to December 2019) in Department of Pathology, Government Medical College. All patients diagnosed with (clinically or radiologically) salivary gland lesions were selected. Clinical details and histopathology slides were collected from hospital and histopathology records, respectively. Data obtained were analyzed using appropriate statistical methods.
Results: A total of 39 cases were studied and majority of patients belonged to 31–50 years. In current study, tumors were common (53.8%) and benign tumors (76%) outnumbered malignant ones. Chronic sialadenitis (44.4%) was common among non-neoplastic lesions. Conclusion: Salivary gland lesions have morphological diversity and histopathology is crucial in deciding the final management of the patient.
KEY WORDS: : : Clinician, coronavirus disease 2019, healthcare workers, personal protective equipments.
Salivary glands are the exocrine glands which secrete saliva to help in digestion process, speech, mastication, and also has high concentration of antibodies thereby participates in body’s defense mechanism.[1] Salivary glands include paired major glands, namely, parotid, submandibular, and submaxillary/sublingual glands and minor salivary glands in and around the oral cavity mainly in lips, cheeks, palate, and tongue.[2] Parotid gland secretes serous saliva, submandibular gland secrets mucinous saliva, and sublingual gland have both serous and mucinous secretions.[3,4] Salivary gland is composed of serous or mucinous acini and ducts along with myoepithelial cells and supporting connective tissue stroma consisting of fibrous tissue, nerves, and blood vessels.[3,4] Salivary gland lesions are common and important entity in head and neck swellings. There is a wide spectrum of salivary gland lesions with clinical and morphological diversity.[5,6] Unilateral enlargement of major salivary glands is commonly seen in conditions such as inflammation cysts, or tumors. Bilateral enlargement of salivary glands is seen usually in inflammation (auto immune diseases), granulomatous disease or diffuse neoplastic involvement.[4] Developmental disorders are extremely rare in salivary glands.[3] A variety of infectious and non-infectious inflammatory conditions commonly occur in salivary glands. Acute and chronic sialadenitis, cysts, various benign, and malignant tumors are the most common causes for salivary gland swellings.[5] Annual incidence of salivary gland neoplasms ranges between 0.5% and 13.5%/1 lakh population worldwide.[7] Salivary gland tumors represent 6% of all the head and neck tumors.[8] Since there is clinically wide range of presentation of both benign and malignant lesions, imaging and fine-needle aspiration cytology also has limited role in accurately diagnosing salivary lesions.[9,10] Salivary glands are not subjected to incisional biopsy or core needle biopsy due to the fear of causing fistula or tumor implantation through the needle tract.[11,12] Minor salivary glands are not accessible for routine aspiration cytology because of their location. Even sonological evaluation has a limited role in diagnosing these minor salivary gland lesions and hence microscopic diagnosis remains gold standard.[13]
1. To study the frequency of various salivary gland lesions including both neoplastic and nonneoplastic conditions
2. To know the histomorphological pattern of these salivary gland lesions.
This study was conducted in the Department of Pathology, Government Medical College, from January 2017 to December 2019. All those patients who attended surgical/ENT outpatient department and diagnosed clinically and radiographically as having various salivary gland lesions were selected for the study. The biopsy samples of these patients who underwent resection/excision/biopsy of salivary gland lesions which were received in histopathology section were labeled, fixed, and examined grossly for various details and subjected for routine tissue processing and Hematoxylin and Eosin (H and E) staining. Complete clinical details including demographic details of all these patients were collected from hospital records. Corresponding H and E stained slides were retrieved from histopathology section and analyzed. Data obtained were tabulated and statistically analyzed using SPSS software.
A total of 39 cases were included for our study. The age group of these patients ranged from 10 to 70 years. Majority of patients belonged to 31–50 years (30.7%) and the least number of cases (2.5%) were seen in the age group of 61–70 years (Table 1). Male predominance (1.78:1) was seen in the present study.
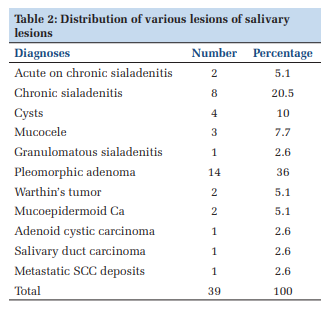
Out of total 39 cases, 46.2% were non neoplastic lesions and 53.8% were neoplastic lesions (Table 2). In non-neoplastic lesions, predominant was chronic sialadenitis (44.4%), followed by cysts (22.2%).
Among neoplastic lesions, benign tumors accounted for 76% and remaining were malignant tumors (Table 3). Most common benign tumor was pleomorphic adenoma (66.7%), followed by Warthin’s tumor (9.5%). Mucoepidermoid carcinomas (9.5%) were common among malignant tumors, while least were adenoid cystic carcinoma and salivary duct carcinoma which constituted 2.6% each of all the salivary gland lesions. There was only one case of metastatic squamous cell carcinoma of parotid gland.
The range of salivary gland lesions is wide and the relative incidences of neoplastic and nonneoplastic lesions are innumerable in different studies. Salivary gland lesions can be broadly categorized in to inflammatory (acute and chronic), non-inflammatory, and neoplastic lesions (benign and malignant neoplasms). Various studies have revealed that 50% of the salivary gland tumors are benign and 5–10% are malignant.[2]
Among non-neoplastic conditions, chronic sialadenitis was the most frequent lesion. There were eight cases of chronic sialadenitis in the present study which comprises more than 50% of non-neoplastic lesions of salivary glands. This is comparable to study by Omhare et al. [14] and Mohan et al. [5]
In our study, majority of non-neoplastic lesions peak in the age group of 31–40 years and was similar to the study done by Pachori et al. [15] and AL-Zamzami et al. [16] Male predominance was seen in overall salivary gland lesions in our study which is in accordance with study by Dave et al. [6]
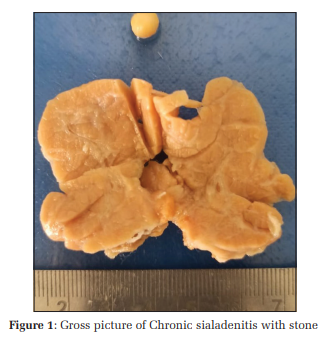
Chronic sialadenitis may be associated with systemic autoimmune disease. Involvement of both salivary and lacrimal glands is seen in SJogren syndrome (Kerato conjunctivitis sicca also known as dry eyes syndrome). Chronic sialadenitis is accompanied by mild clinical symptoms and on histology shows mild to moderate degree of lymphoplasmacytic infiltration associated with various degrees of atrophy, fibrosis, and microliths, if the causative factor is obstruction by stones[4] (Figures 1 and 2). Chronic sialadenitis was the most common disease among non-neoplastic lesions followed by cysts and mucocele of salivary glands. These were predominantly seen in submandibular glands. This is comparable to the study done by Omhare et al.,[14] Pachori et al.,[15] AL-Zamzami et al.,[16] Kumar et al.,[17] and Soni et al. [18]
Benign cysts of salivary glands comprised 10% of all the lesions. Out of this we documented one case each of simple cyst and one case of branchial cyst. This was comparable to the study done by Omhare et al.,[14] Mohan et al.,[5] and Pachori et al. [15]
Among the cystic lesions in salivary glands, the most common are lymphoepithelial cysts and other cysts like branchial cleft cyst. Lymphoepithelial cysts can occur in HIV positive patients or as non-specific cysts. These were characterized by unilocular/ multilocular cystic spaces lined by glandular or squamous epithelium surrounded by hyperplastic lymphoid follicles.
There were three cases of mucocele in our study and all were seen predominantly in submandibular glands. Mucocele results from blockage or rupture of a salivary gland duct with consequent leakage of saliva into the surrounding connective tissue stroma. Since mucocele occurs frequently in minor salivary glands, it is usually seen in the lower lip as a result of trauma. Mucocele, on histology, showed cyst like space lined by inflammatory granulation tissue or by fibrous connective tissue. These spaces were filled with mucin and numerous cyst macrophages.
Our study observed only two cases of acute on chronic sialadenitis (5.1%) both in the middle aged men and involved submandibular glands. Acute inflammation of salivary glands may result from bacterial or viral infections. Non-specific bacterial sialadenitis commonly involves major salivary glands. Acute sialadenitis due to Mumps virus generally occurs as epidemic since they spread through saliva. These lesions are rarely biopsied.[3] Acute sialadenitis can occur rarely due to fungal organisms especially in immune compromised individuals. In rare cases, acute sialadenitis may occur due to obstruction by stone (sialolithiasis). Sialolithiasis were frequently observed in submandibular glands. On microscopy, acute sialadenitis showed mild to moderate neutrophilic infiltrate in the gland and lead to suppurative sialadenitis in complicated cases.
In a study by Pachori et al.,[15] non-neoplastic lesions of salivary glands were 43.8% and neoplastic lesions were 56.2%. Current study observed that neoplastic lesions (53.9%) outnumbered non-neoplastic lesions (46.1%) which was a similar finding seen in study done by Pachori et al. [15] and AL-Zamzami et al. [16] In a study by Omhare et al.,[14] non-neoplastic lesions were more than the neoplastic lesions. The probable reason for this can be attributed to geographic variation.
A study of salivary gland tumors in Brazilian population by Reinheimer et al. [21] concluded that parotid gland is the most common location; pleomorphic adenoma is the most common benign tumor; and mucoepidermoid carcinoma was the most common malignant tumor. Malignant tumors showed various histological types.
Bobati et al. [22] observed 69% of benign tumors in their study. Pleomorphic adenoma and adenoid cystic carcinoma were the most common benign and malignant tumors, respectively. Among the salivary gland tumors, benign tumors (76%) were more commonly observed in the current study and pleomorphic adenoma (66.7%) was the most frequent benign tumor, followed by Warthin’s tumor (9.5%). These observations were comparable to the study done by AL-Zamzami et al. [16] and Pachori et al. [15] (Table 4).
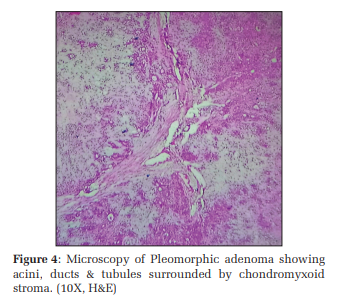
We observed 14 cases of pleomorphic adenoma (36%) and two cases of Warthin’s tumor (5%). Pleomorphic adenoma occurs in parotid gland more frequently with female preponderance. Because of their significant histologic diversity these tumors are also named as benign mixed tumors. These are derived from a mixture of ductal (epithelial) and myoepithelial cells and hence they exhibit both epithelial and mesenchymal differentiation. Grossly pleomorphic adenoma showed a well circumscribed tan white, firm, encapsulated mass with glistening, translucent appearance on cut section. On microscopy, these tumors showed epithelial cells arranged in various patterns such as ducts, acini, cords, tubules, and sheets. These epithelial cells are scattered within a mesenchyme such as background of loose myxoid, chondroid, fibrillar, and sometimes osseous stroma (Figures 3 and 4). Rarely carcinoma can arise in pleomorphic adenoma and it is referred to as pleomorphic adenoma ex carcinoma or malignant mixed tumors.[2] There were no cases of pleomorphic adenoma ex carcinoma in our study.
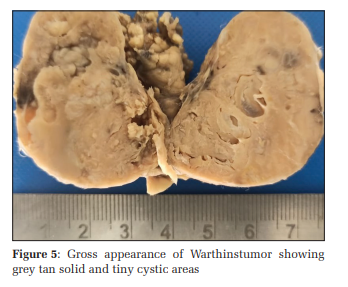
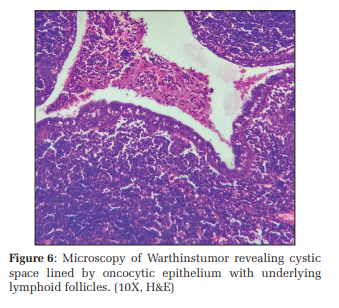
Warthins tumor was the second common benign tumor (9.5%) observed in our study. This is a benign tumor almost always arising in parotid gland and more commonly in males. Grossly these tumors were round to oval, encapsulated masses arising in superficial parotid gland. Cut section revealed a pale grey surface with tiny cystic spaces filled with mucinous or serous secretion. On histology, Warthins tumor showed cystic spaces, epithelial component, and lymphoid component. Cystic spaces are lined by double layered epithelial cells resting on dense lymphoid stroma (Figures 5 and 6). Surface epithelium shows palisading oncocytic cells and underlying basal cuboidal cells.[2] Stroma showed lymphoid cells at places having prominent germinal centers.
In the present study, we found that mucoepidermoid carcinoma was the most common malignant tumor (9.5%) and least was adenoid cystic carcinoma and salivary duct carcinoma (4.8%). This was similar to study done by Soni et al. [18] and Susmitha and Sathyaki.[23] Mucoepidermoid carcinoma grossly revealed a solid irregular grey white lesion occasionally shows microcysts. Microscopy shows intermediate type of tumor having of three types of cells, that is, squamous, intermediate, and mucin secreting cells. Tumor cells were seen in solid, nests, and sheets of tumor cells infiltrating the adjacent stroma. Mucoepidermoid carcinomas were categorized to high grade, intermediate grade, and low grade depending on cytologic atypia.[20]
There was one case of adenoid cystic carcinoma grossly showed partly circumscribed solid tumor with infiltrative growth pattern. Microscopy revealed characteristic cribriform pattern of the arrangement of tumor cells. It showed numerous pseudocysts filled with homogenous eosinophilicperiodic acid schiffpositive material. Adjacent basophilic bland appearing tumor cells also show glands, tubules, and solid pattern and also there were perneural infiltration by these tumor cells. This tumor has a tendency to invade perineural spaces.[20]
Our study observed one case of salivary duct carcinoma a rare malignant tumor of salivary gland occurred in elderly male. On histology, it resembled invasive ductal carcinoma of breast. Tumor may show different pattern such as solid, comedo, cribriform, papillary, apocrine invasive micro papillary, or mucinous areas.
In a study done by Franzen et al.,[24] secondary deposits in the parotid gland increasingly frequent and most of which are metastases of skin tumors, commonly squamous cell carcinoma. Our study observed a case of metastatic squamous cell carcinoma deposits to submandibular salivary gland in a female patient aged 42 years. Patient had squamous cell carcinoma of oral cavity and developed metastatic deposits in salivary gland. Grossly, it revealed a grey-white infiltrating growth in the salivary gland. On microscopy, this case showed well differentiated squamous cell carcinoma composed of nests and sheets of atypical squamous cells infiltrating adjacent stroma. There were many keratin pearls noted along with areas of hemorrhage and necrosis.
Overall, non-neoplastic lesions were commonly seen in submandibular gland and followed by parotid gland, whereas neoplastic lesions were commonly distributed in parotid gland followed by submandibular glands and minor salivary glands in decreasing order of frequency. Parotid region is the most common site for all tumors. Similar findings were seen in study done by Omhare et al. [14] and Khandekar et al. [25]





There is a wide spectrum of salivary gland diseases with morphological and clinical diversity. Our study concluded that neoplastic lesions are common than non-neoplastic ones and pleomorphic adenoma and chronic sialadenitis are the most common lesions observed, respectively. Mucoepidermoid carcinoma is the frequent malignant tumor seen. Parotid region is the most common site for all the salivary gland tumors. Histopathological examination is very crucial in diagnosing non-neoplastic and neoplastic lesions of salivary glands and it is also the gold standard in accurately deciding the final clinical management of the patient.
Subscribe now for latest articles and news.