Journal of Medical Sciences and Health
Year: -0001, Volume: 8, Issue: 1, Pages: 47-51
Original Article
Siddhartha Sarma Biswas1 , Dhrubajyoti Borpatragohain2, Changhom Thoumoung3
1Registrar, Department of Radio diagnosis, Assam Medical College, Dibrugarh,
2Associate Professor, Department of Radio diagnosis, Assam Medical College, Dibrugarh,
3Assistant Professor, Department of Radio diagnosis, Assam Medical College, Dibrugarh Address for correspondence: Siddhartha Sarma Biswas, Registrar, Department of Radio diagnosis, Assam Medical College, Dibrugarh.
E-mail: [email protected]
Background: Pulmonary tuberculosis is one of the most common infectious disease in developing country like India. Due to delay in diagnosis causes extensive lung damages leading to increased morbidity in patients. Objective: The aim of the study is to evaluate the various patterns of HRCT findings in cases of sputum positive pulmonary TB. In our study, findings of HRCT thorax of 50 patients of sputum positive pulmonary tuberculosis are studied retrospectively. Result & Conclusion: Consolidation was the most common HRCT finding in these patients. These patients also showed other patterns such as tree in bud opacities, ill-defined patchy opacities, cavities, bronchiectasis etc. Additional features like pleural effusion, pneumothorax, tubercular spondylitis are also seen in many patients. HRCT thorax is a useful investigation modality used to diagnose as well as for follow up of patients.
Keywords: Consolidation, Cavity, Bronchiectasis
Tuberculosis is an infective disease caused by bacteria of Mycobacterial species. It spreads via droplet infection when contaminated aerosols are transmitted from infected person to others especially at the time of coughing. Pulmonary tuberculosis is a very much prevalent disease in the world. It contributes to a large population suffering from morbidity and with patients recovering from the disease can be let with some irreversible results decreasing the quality of life.[1] The first killer disease among HIV positive patients in also tuberculosis.[2] Pulmonary tuberculosis is one of the most commonly encountered disease in developing country like India. Risk factors include overcrowded areas, elderly peoples, and peoples with poor nutrition and in immunocompromised persons, poor socio economic status. Patients may present to the physicians with symptoms which mimic common cold, allergy etc. Chest X ray is the most commonly and early done investigation in persons suspected of having pulmonary TB. However, early cases may be missed on chest radiograph ultimately leading to delay in diagnosis & more complication. More sensitive tool for diagnosis pulmonary TB is HRCT of thorax, which is able to demonstrate the subtle findings in the lungs. HRCT thorax is also well equipped to better demonstrate the extent of the parenchymal involvement. The tuberculin test is also used along with other investigations for the diagnosis of the condition.[3]
Following exposure of an individual to the bacilli, the person may develop latent infection or clinical disease.[2] When patients develop disease following primary infection it is called primary tuberculosis. In persons, exposed to the bacillus previously, develops disease it is called as reactivation tuberculosis. Primary tuberculosis is mostly seen in the pediatric population and post primary tuberculosis in the adult population.
Radiological imaging helps in achieving the following goals in cases of pulmonary TB – A) Diagnosis B) Treatment response C) Sequalae or complication of tuberculosis. HRCT of thorax is indicated in these cases.[3]
HRCT thorax findings which are suggestive of active pulmonary disease include the consolidation, tree in bud opacities, cavities etc. Fibrotic opacity, calcifications etc are associated with inactive disease.[4] Results of sputum and culture take relatively long time and have high risk of infected person communicating the disease process to other healthy individuals, thus showing the risks associated with conventional approaches. Moreover, CT scan can also be used to evaluate necrotic mediastinal nodes, parenchymal opacities in a more detailed pattern and as well as it is less time-consuming thus reducing the time required prior to start antimicrobial therapy.[5]
HRCT thorax is a useful tool in the evaluation of sputum negative pulmonary tuberculosis also.[6]
In our study, HRCT findings of 50 patients of sputum positive pulmonary tuberculosis were retrospectively studied and their results were evaluated, and their HRCT thorax findings and patterns were studied.
To study the HRCT pattern of pulmonary involvement in sputum positive patients of pulmonary tuberculosis in North Eastern part of India.
Our study was done in Department of Radiodiagnosis, Assam Medical College and hospital, Dibrugarh, Assam. The study is hospital based cross-sectional study. Duration of study was one year from June 2020 to May 2021. Institutional ethical clearance was taken prior to the study. Informed written consent was taken from all subjects who were part of the study.
Inclusion criteria: All patients who were advised to undergo HRCT thorax and were suffering from sputum positive pulmonary tuberculosis. Exclusion criteria: Patients who did not give consent and were not willing to be a part of the study and patients with known malignancy.
It is a retrospective study where 50 cases of sputum positive cases for AFB were subjected to HRCT thorax and the findings obtained were studied. We have considered 50 patients for our study. Out of total 50 patients, 36 (72 %) patients were males and 14 (28 %) patients were females. Consolidations were found in 42 (84%) patients. Out of these patients, 9 (21%) patients showed involvement of right lung only, 10(24%) in left lung and 23(55%) patients showed bilateral lungs involvement. Among the patients having consolidation upper lobar involvement was seen in 33 (79%) patients. Superior segment of lower lobe involvement was seen in 30 (71%) patients. Illdefined opacities were seen in 23 (46%) patients and absent in 27 (54 %) of cases. It was distributed in right lung in 4 (17%) cases, left lung in 2 (8%) cases and both lung involvement in 17 (73 %) cases.
Ground glass opacities was seen in 12 (24%) patients and absent in 38 (76 % of cases), It was distributed in right lung in 2 (16 %) cases, in left lung 3 cases (25%) and bilateral lungs involvement in 7 (58 %) cases. Tree in bud opacities which denotes endobronchial spread of the infection were seen in 22 cases (44 %) and it’s absent in 28 (56%) of cases. Endobronchial spread was seen along with consolidation in all the patients. 4(18%) cases showed right lung involvement. Left lung involvement was seen in 2 (9%) cases and bilateral lung involvement were seen in 16 (72%) cases. Cavities were seen in 31 (62%) of cases and absent in 19 (38 % of cases). Cavities were formed within the areas consolidation. The cavities were distributed in right lung in 8 (25%), in left lung in11 (35%) and bilateral involvement in 12 (38%) of cases. Pleural effusion was seen in 7 cases (14 % of cases). Mediastinal lymphadenopathy was seen in 9 (18 %) of cases.
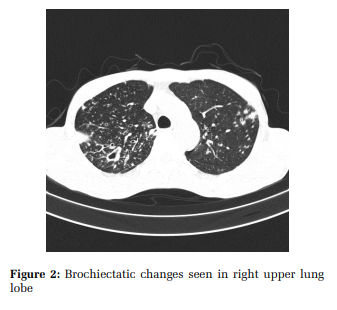
Pneumothorax was seen in 1 (2%) of cases. Bronchiectasis was seen in 21 (42 %) of cases & absent in 29 (58 %) of cases. Military pattern was seen in 2 (4 %) cases. Associated spinal TB was found in 1 (2 %) case. Fungal ball was seen in 2 (4 %) cases.
In our study we have found that majority of the patients are male compared to females which is similar to study done by Soujanya Bolla et al.[7] Similarly high incidence among male population was also reported by Philippe Glaziou et al.
84 % of patients show consolidation in lung parenchyma. In our study, consolidation with bilateral lung involvement is seen in majority of patients (54%). Unilateral lung involvement is seen in 46 % of patients, 21% in right lung and 24 % in left lung only. Mostly the upper lobe and superior segment of lower lobes are involved in our study. How Wu et al[8] reported consolidation in 68.3 % of patients and Bolla et al[7] reported consolidation in around 67 % of patients. Consoliation with volume loss was also reported by approximately 68.8 % patents by M. Aribandi et al.[9] Confluent consolidation was seen in 37.5 % cases.[9] Patchy poorly defined consolidation predominantly in apical and posterior segments of upper lobe is the earliest parenchymal finding of pulmonary tuberculosis.[10] However, Raniga et al found consolidation in about 52 % patients.[11]
In our study, ground glass opacities are seen in 12 (24%) of cases. Bolla et al[7] found it in 16.6 % of patients. Tree in bud opacities are seen in 44 % of patients. Bolla et al[7] found it in 75 % of patients. How Wu et al[8] found it in 61.3 % of patients and Hatipoglu et al[12] found it in 71 % of patients.[12]
Tree in bud opacities were reported in 80 % of cases by Raniga et al.[11] Tree in bud opacity suggests endobronchial spread of tuberculosis.[13] However, it may also be found in other various conditions.[14] Ill-defined opacities are found in 46 % of patients. Raniga et al[11] found it in 40 % of patients. Bolla et al[7] found it in 71 % of patients. It was found to be about 11 % by Steven et al and 61 % by Lee et al.[11] Ill defined opacities reveals spread of infection by the pores of Kohn.[15,16] In our study, mediastinal lymphadenopathy seen in 9 (18 % of patients). How yu et al[8] found it in 14.6% of patients. Hatipoglu et al[12] found it in 16 % of patients. Mediastinal node with diameter of more than 2 cm with necrotic centres is suggestive of active disease.[17]
It is to be noted that the most common finding in children with tuberculosis is mediastinal lymph node enlargement which is seen in approximately 90- 95 % of cases.[18,19] However, in post primary tuberculosis it is seen in approximately 5 – 10 % of patients.[20,21]
In our study, cavities were found in 62 % of patients. Raniga et al[11] found cavities in 64 % of patients. Bolla et al[7] found cavities in 41.6 % of patients. Hatipoglu et al[12] found cavities in 50 % of patients. RK Jayasree Devi et al found cavities in approximately 61 % of patients.[22] Steven et al and lee et al found cavities in 36% and 58 % of patients.[11] Tubercular cavities have usually satellite parenchymal pathology and have varying wall thickness. Tubercular cavities are usually multiple in number. Cavities are usually seen within the areas of consolidation. In active cavities, the walls are usually thicker and show mild post contrast enhancement. In case of super infection of a cavity there may be presence of air fluid level.[23] Cavity is the hall mark of post primary tuberculosis.[22] Cavity formation is less common in primary tuberculosis.[24] In our study, bronchiectasis was found in 42 % of patients. Hatipoglu et al[12] found it in 56 % of patients. 81.3 % of cases showed bronchiectasis in study done by M. Arabandi et al.[9] The distribution of bronchiectasis was more common in the regions of lung affection. Irreversible dilatation of bronchus develops due to the result of destruction and fibrosis of lung parenchyma. The upper lobes are the commonest site for development of bronchiectasis.[25] Thick and irregular narrowing of air way is seen in active disease. Smooth narrowing with thin walls is a finding of chronic disease.[26–28]
In our study pleural effusion is seen at 14 % of patients. How Yu et al[8] found it in 15.6 % of patients. Raniga et al found pleural effusion in 12 % of cases.[11] Lee et al found it in 10 % of cases.[11] Pleural effusion is commonly seen in patients with parenchymal involvement. Sometmes it may also be a loculated pleural effusion.[13] Half of the patients with pleural involvement with tuberculosis may show sub pleural cavity formation.[29] Post treatment there may be pleural thickening and calcifications.[30] We have seen miliary TB in 4 % of cases. Hatipoglu et al[12]
found military TB in 3 % of patients. Miliary pattern of tuberculosis is seen due to hematogenous pread of the bacilli.[11] Usually miliary nodules are distributed randomly in the lung parenchyma. CT scan is able to detect miliary tuberculosis earlier than the conventional radiographs. Intra and interlobular septal thickening is commonly associated with miliary pattern.[31,32] Focal or diffuse consolidation may form due to coalescence of the miliary nodules.[23]
In our study one case (2 %) of pneumothorax and spinal tuberculosis are associated with pulmonary tuberculosis. RK Jayasree Devi et al found pneumothorax in 0.6 % cases.[22] Fungal ball is seen in 2 (4 %) cases. Association of aspergilloma with chronic tuberculosis is reported to be at about 11 %.[33]
The presence of consolidation, tree in bud opacities, cavities and other HRCT patterns of pulmonary tuberculosis when examined can help in early diagnosis of pulmonary tuberculosis. The patterns may thus help the radiologist to identify the disease process early and in turn will help clinician to treat the patients and thus they will get rid of severe morbidity which can happen due to delay in diagnosis

Subscribe now for latest articles and news.