Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i01.010
Year: 2021, Volume: 7, Issue: 1, Pages: 56-63
Original Article
Lakshmi V Pandit1, Neil M Salian2, Aishwarya M Salian3
1Professor and Head of Department, Department of Psychiatry, Kempegowda Institute of Medical Sciences, Bengaluru, Karnataka, India,
2Intern, Kempegowda Institute of Medical Sciences, Bengaluru, Karnataka, India,
3Intern, A.J. Institute of Medical Sciences, Mangalore, Karnataka, India
Address for correspondence:
Mr. Neil M Salian, Intern, Kempegowda Institute of Medical Sciences, Bengaluru, Karnataka, India. Phone: +91-9972530030. E-mail: [email protected]
Objective: In December 2019, the world experienced spread of severe acute respiratory syndrome- Coronavirus disease 2019 (COVID-19). Measures to contain spread included movement restrictions (Lockdown), quarantine for contacts, and institutional care for those infected. Fear of contracting the infection, mortality rates, experience of a lockdown, and economic concerns exposed people to great stress. On this background, the present study was conducted to assess psychological distress in these times.
Methods: Consenting individuals comfortable to respond to an online survey were included as subjects. The study is cross-sectional in design; descriptive analysis and Chi-square tests were done. Socio demographic details were collected. Kessler 10 Psychological Distress Scale was administered to assess psychological well-being.
Results Psychological distress was seen in 68% of the sample, ranging from mild-to-severe, across all age group, except in those below 18 years. Those aged 30–59 years experienced psychological distress before lockdown as well. Females experienced more distress than males, as well as those of the group with lower income.
Conclusions: Responsibility of maintaining psychological well-being rests with each of us. Healthcare workers and mental health professionals need to identify and address psychological issues in the population during this period. Governmental organizations must take on the responsibility to educate the public through newspapers, television, and social media about the importance of maintaining positive psychological health and contribute to the same by honest journalism.
KEY WORDS: Coronavirus disease 2019, pandemic, psychological distress
The first coronavirus (CoV) outbreak was witnessed in 2002–2003 with the emergence of severe acute respiratory disease CoV (SARS-CoV).[1] A second severe CoV, Middle East respiratory syndrome CoV (MERS-CoV), emerged in 2012 in Saudi Arabia.[2] The human CoVs, including MERS-CoV and SARS- CoV, is thought to be outspread by bats into an intermediate host. In December 2019, a series of pneumonia cases of unknown cause emerged in Wuhan, Hubei, China, with clinical presentations greatly resembling viral pneumonia. Analysis from lower respiratory tract samples indicated a novel virus, named 2019 novel CoV (2019-nCoV). The disease spread the world over and was declared by the World Health Organization as a pandemic on March 11, 2020.[3] The existence and identity of an intermediate host for the 2019-nCoV have yet to be determined. Direct transmission of CoVs from bats and snake to people is also theoretically possible by virus entry into the tracheo-bronchial tree, by droplet, contact, and fomites. The Coronavirus disease 2019 (COVID-19) has undergone eleven mutations so far, the implications of which are yet to be understood.[4]
World’s statistics The total number of confirmed cases as on May 29 was 57,01,337, with deaths numbering about 3,57,688. The United States of America have 26,13,092 cases with about 1,51,212 deaths.[5]
India’s outbreak 2020 The first COVID-19 case was confirmed in Kerala’s Thrissur district after a student who had returned home for a vacation from Wuhan University in China, tested positive. It quickly spread to other states. Since then Government of India (GOI) have taken essential steps to curtail the disease spread, by the ideology of quarantine of the diseased in the first stage of the pandemic. India has more than 1,65,799 cases with about 4,706 deaths.[5] Given the phase of the pandemic, isolation became mandatory to control spread. Given the population of the country and the fact that social distancing would be very hard to implement and maintain, India chose to lockdown. The global picture of the pandemic took an ugly turn with a large number of deaths in Italy, Germany, Spain, and then USA.[6] A large number of people lost jobs and are likely to lose jobs in the aftermath of this epidemic. Life seemed extremely uncertain, both in terms of health and economic stability. Staying indoors all day involves immense lifestyle modifications. This change, coupled with the current times and events is bound to exert some degree of stress on all of us. With this in mind, the current study was undertaken, to evaluate the psychological distress in the Indian population, an issue yet to be looked at in our country.
Objectives The objective of the study was to study the psychological distress due to SARS CoV-19 pandemic in a state of imposed lockdown.
Nature of study group This study was conducted by the Department of Psychiatry, Kempegowda Institute of Medical Science and Research Centre, Bengaluru. It is a quantitative, community based cross-sectional study.
Recruitment
A request to participate in the study was sent to all contacts of the researchers, through a mobile message. On their approval, details of the study were sent to them with a mention that all data would be kept confidential, anonymous, and that they could withdraw their response at any time. They were in turn requested to send us details of their contacts, which were also recruited in the study if willing.
Sample size
Estimated sample size was 3600. The total number of subjects who participated in this study was 4,309, 1,065 of whom were from outside the country, with 897 being non-resident Indians (NRI) and 168 international citizens.
Measurement/evaluation
Online based, self-administered questionnaires were personally sent to all participants starting April 1, 2020, recruited being continued till April 21, 2020, Day 8 to Day 28 of the enforced lockdown. Socio-demographic details were procured using a pro forma made for the purpose. The Kessler Psychological Distress Scale (K10) was used to assess psychological distress. It contains ten questions, each with a five-level response: From (1) “none of the time” to (5) “all of the time”. Scores of the ten items are then summed up, yielding a minimum score of ten, and a maximum score of 50. Low scores indicate low levels and high scores indicate high levels of psychological distress. Interpretation of total scores: 10–19: Likely to be well; 20–24 likely to have a mild disorder; 25–29 Likely to haveamoderatedisorder;30–50Likelytohavea severe disorder.[7] The Kessler ten scales were to be answered for two occasions – for the month before lock down and the period of the lockdown. Travel history in the past 3 weeks, and an understanding about the illness (signs, symptoms, and mode of transmission) was noted.
Inclusion criteria
All consenting individuals who were comfortable in answering an online questionnaire were included in the study.
Exclusion criteria
Those individuals who were not comfortable with answering an online questionnaire were excluded from the study.
Statistical analysis
The statistical data were analyzed using the Python statistical tool. Descriptive statistics and multiple logistic regression analysis were done.
Sample details
Sample size of this study is estimated using Cochran’s Formula and estimated to at least 3760 samples. Total of 4309 samples were taken for the study after excluding the incomplete data.
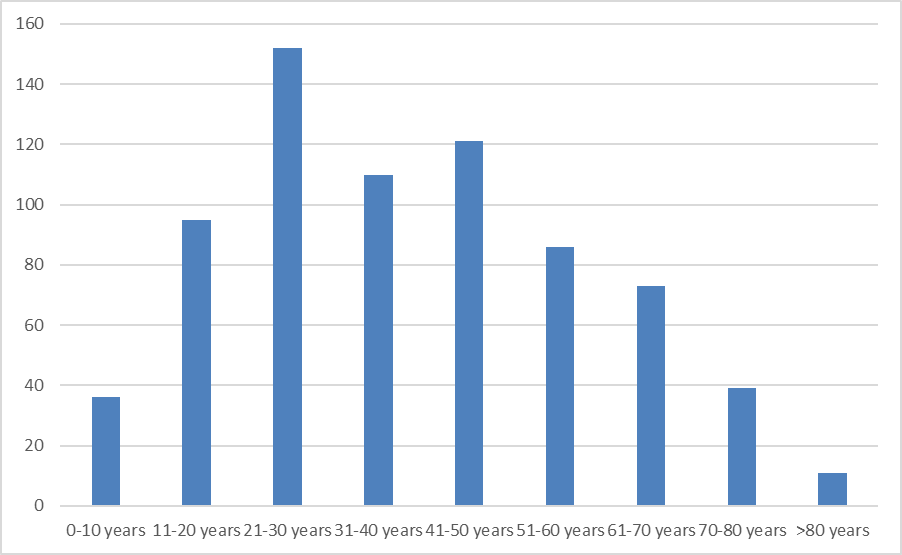
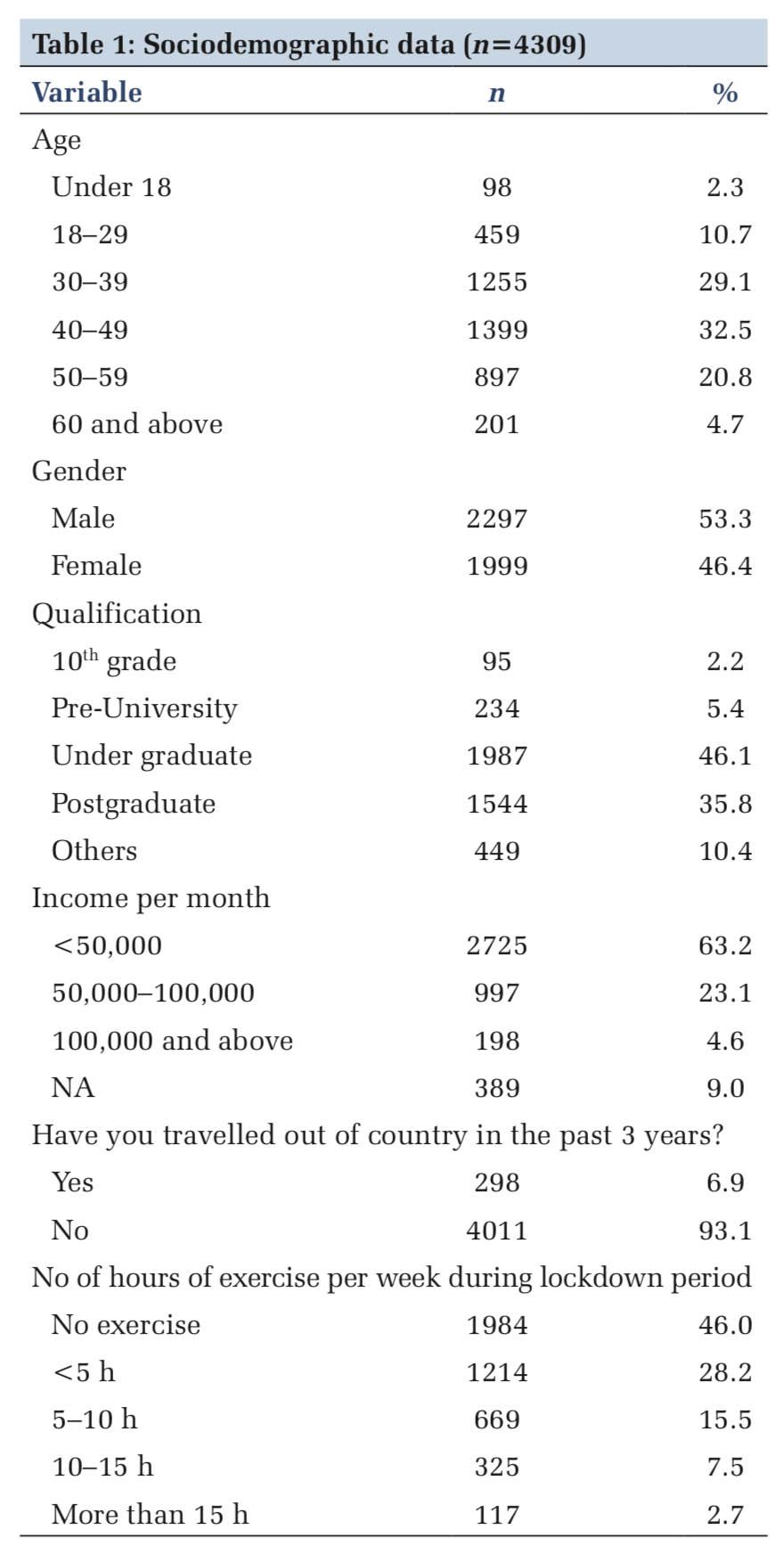
The statistical data were analyzed using the Python statistical tool. Majority of the responders were in the third and fourth decade of life (61%). Both genders were almost equally represented in the sample, with a slight male preponderance. About 92% of the sample had an undergraduate or higher level of qualification. Indian National citizens constituted majority of the sample (75.3%) (Table 1). About 63% of the respondents had a monthly income less than 50,000 while 23% had between 50,000 and 100,000. Only 7% of the respondents had travelled out of the country in the past 3 weeks. About 46% of the subjects had no form of exercise (Table 1).
Study limitations This study has been conducted at a period in time which is extremely rare, a pandemic. Prior documentation on the mental health impact of other infectious disease outbreaks is sparse. There is, therefore, very little literature to compare with. As it is an online survey, responses were sought from the urban, educated, affluent population, and are therefore difficult to generalize.
Strength of the study The population of the study was large, and subjects responded within the period of lockdown. The responses received would, therefore, be depictive of their emotional state.
1918–1920 saw the Spanish Flu pandemic, infecting 500 million and killing 50 million people. The world is now witnessing the COVID-19 pandemic, a global health crisis posing the greatest challenge to the world since then. Since it was first reported from Wuhan, China, in December 2019, it has spread to every continent except Antarctica. The pandemic has the potential to create devastating social, economic, and political crisis than ever before. Countries are going into lockdown, creating ghost cities. People are losing jobs, their livelihood, and their income, with absolutely no idea when things will get back to normalcy.
India is a developing country, with a population of about 137 crores. The first case in our country was reported on the January 30 and has been spreading widely. To contain the spread, India, went into lockdown in two phases, March 25 to April 14–26, 2020, with an extension to May 3, 2020, and subsequently till May 21. People remained indoors, venturing out for their daily needs, while some worked from home. Anxiety regarding several issues occupied the minds of one and all.
Socio-demographic details In the current study, majority of the subjects were between 18 and 60 years of age, probably the age that the researchers could connect with digitally, and who would be comfortable responding to an online questionnaire. The population was represented by highly qualified individuals, as compared to the education levels in the country, with both genders being almost equally represented and belonging to the upper or the upper middle class.[8] About 7% of the subjects had travelled outside the country over 3 weeks before onset of lockdown. All the participants were aware of the pandemic, its cause, the symptom profile, need for quarantine, treatment, and possible outcomes.
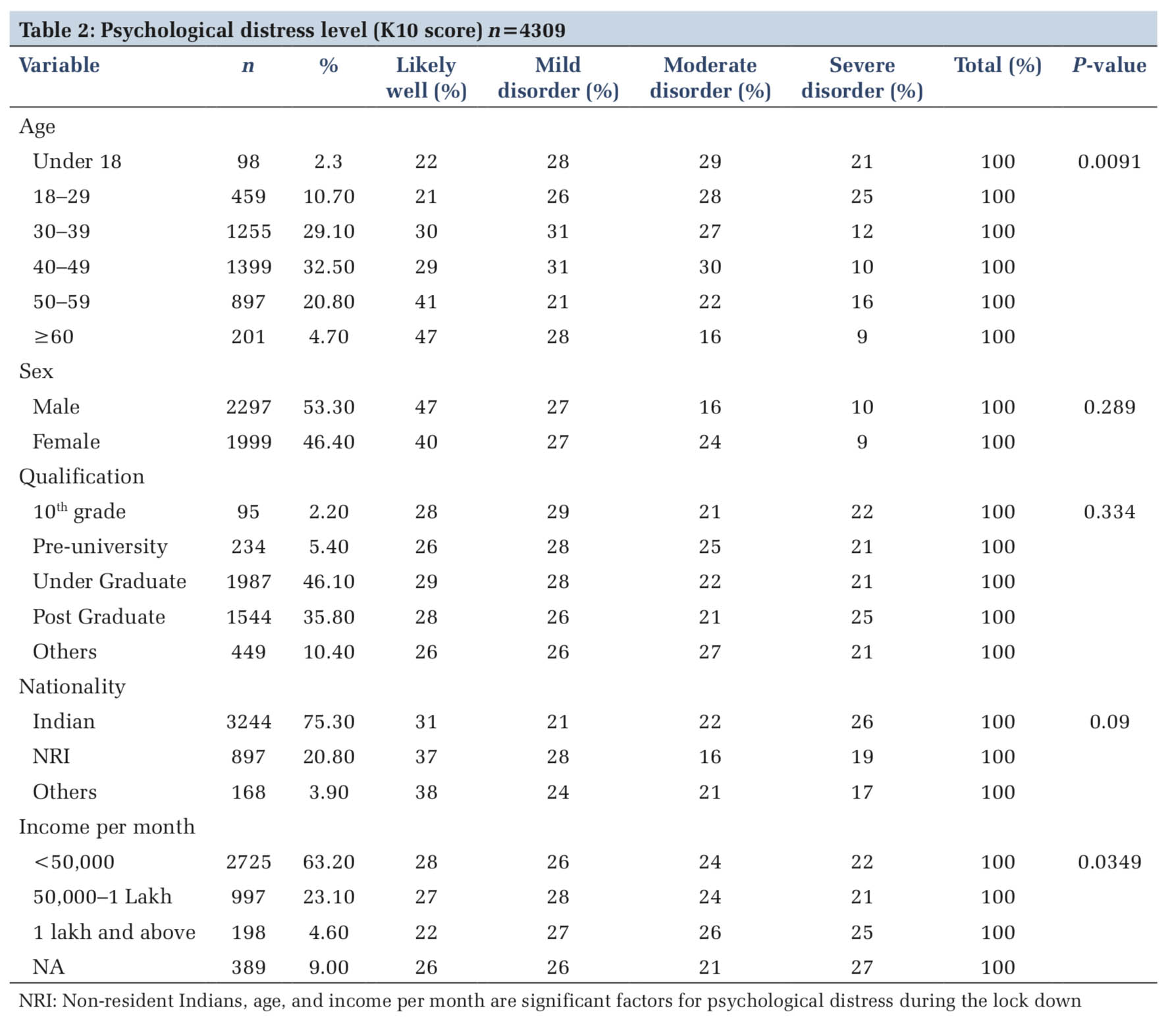
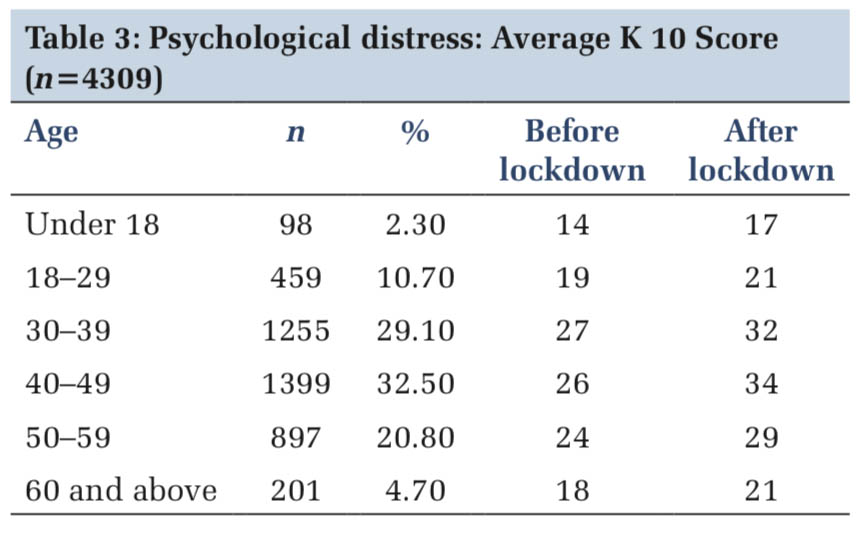
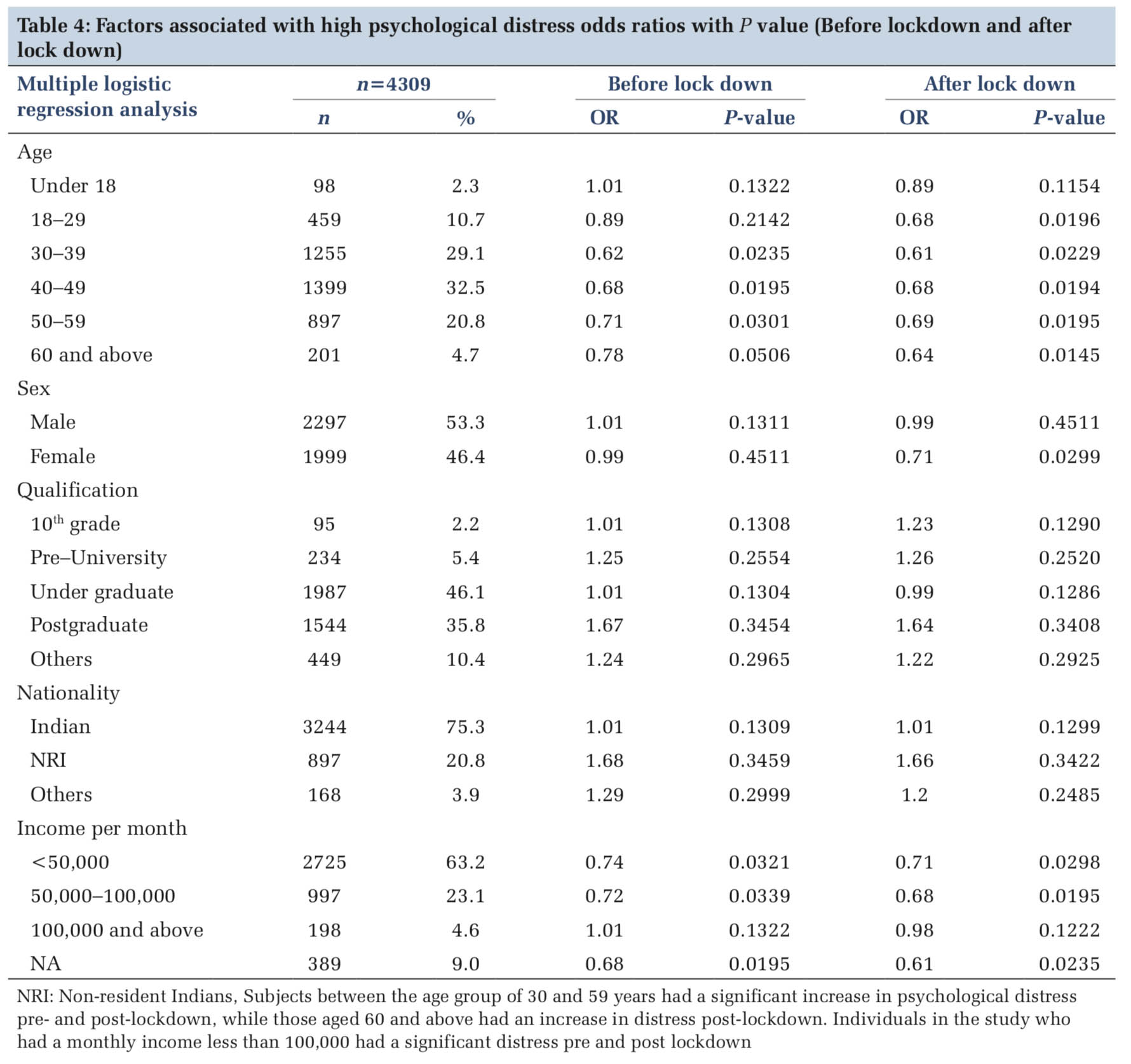
Psychological distress and lockdown The CoV pandemic “has the seeds of a major mental health crisis,” the United Nations warned the world. In our study, psychological distress was seen in 68% of the sample (1363/4036), ranging from mild-to-severe, across all age groups, except in those below 18 years of age [Table 2]. Those aged 30–59 years experienced psychological distress before lockdown as well, with average K10 scores showing an increase post lockdown [Table 3]. The age groups 30–39 and above 60 years experienced distress post lockdown [Table 4]. Our findings are in keeping with several other studies done in the same period.
Symptoms of depression, anxiety, and stress were found in a Chinese study done in the early stages of the COVID-19 infection.[9] In the South Indian state of Kerala, the number of persons who contacted counselors seeking help to overcome stress, anxiety, depression, sleep impairment, stigma issues (fear of contracting COVID-19), and other psychiatric issues stood at 8659, with 1930 reporting of anxiety, 98 of depression, 789 of sleep impairment, 1149 of stigma issues, and 214 for other psychiatric issues.[10] Another Indian study on initial impact of COVID-19 found that there was a significant psychological impact on one-third of their sample population.[11] In particular, people who contract the disease, those at heightened risk for it (including the elderly, people with compromised immune function, and those living or receiving care in congregate settings), and people with pre-existing medical, psychiatric, or substance use problems are at increased risk for adverse psychosocial outcomes.[12]
Being an unnatural situation, the lockdown has given rise to several behavioral issues. Man was meant to be a social animal, and confinement in a small space for any length of time can cause great distress. With an indoor life and nowhere to go, combined with an environment of disease, death, and poverty, negative cognitions are almost the rule, and nihilism sets in. A study conducted in communities affected by SARS in the early 2000s revealed that although community members, affected individuals, and healthcare workers were motivated to comply with quarantine to reduce the risk of infecting others and to protect the community’s health, emotional distress tempted some to consider violating their orders.[13] Individuals have ended their lives, unable to face the suffering of the illness and the isolation[14-16] or for fear of being infected with it.[17,18]
Access to the outside world is only through the media, in terms of the newspapers, television, and social media, with TV being the most popular, both for information and entertainment. The good and the bad of the pandemic situation are constantly discussed in all channels, and very often deficits faced by the country, defeats, and death are amplified. Psychological distress is, therefore, imminent.
Several factors probably govern the experience of psychological distress pre lockdown in the above named age groups in the current study. These individuals are bread winners, being called on to bear financial and other family responsibilities. Before the outbreak of the virus, India, was experiencing an economic slowdown, as a part global slowing of economy 2019. Retaining a job, being paid for the period of lockdown, or finding another appropriate one became a matter of immense stress. College education for children, within the country or abroad, makes huge demands on financial resources. This population also need to provide care for elderly parents, some of who live with them. This is a responsibility they are expected to fulfil, though families structure is more nuclear.
The income groups that form the sample under the current study are the upper middle and upper classes of society. Over the past few decades, procuring several comforts for the family such as housing, land, vehicles, and education through loans has been on a significant rise.[19] Families are thus committed to paying monthly installments toward repaying them. Hitherto, this was not an important factor, as buying any comforts on a loan was looked on as a taboo, and most families would have shunned it.
In India, working from home has been followed only in certain sectors of the work force, namely information technology and biotechnology. With a change in work pattern, organizing office space, internet connectivity, power supply, technical failures, etc., become maters of great concern.
The female population in the study sample faced significant distress post lockdown. With all members of the family being home, the lady of the house has to deal with extra demands on domestic work such as cleaning washing. If she is a “work from home” person, the demands on her are immense. Indian homes, especially those with incomes such as those included in this study, have in their employment a maid who does the washing and cleaning,[20] and a cook who manages the entire kitchen activities. Non availability of helpers during lockdown has increased household burden. Staying indoors and interacting with family members for long periods of time gives rise to interpersonal issues, and divorce rates have increased during this period.[21] Domestic violence, intimate partner violence, and mostly against women have been on a steep rise during the current lockdown.[22]
The younger individuals (< 18 years) appear to be less distressed in our study; however, psychological distress scores have increased post lockdown. There are issues with regard to online classes, more so in rural India, where connectivity is inadequate and home schooling o poses many issues. In an incident in Mallapuram, Kerala, a girl in her ninth grade ended her life as she did not have access to a smart phone for her classes.[23] Incidents of incest against the female child have been reported in this period.[24]
In our study, it was seen that those older than 55 years had an increase in distress score post lockdown, though not statistically significant. Most of them are likely to be suffering from one or more medical morbidity[25] and it is known that the prognosis for such individuals if infected, is poorer. Fear of quarantine, hospitalization, intensive unit care, ventilator care, etc., would be responsible for their distress.
With life coming back to normal, and people returning to work, social distancing would be hard to maintain in a country like India, where cities are densely populated.[26] People get to work in public transport, where social distancing is near impossible to maintain given fewer numbers of buses and trains. The infection is expected to see a huge spread once cities are reopened, with a possibility of lockdown for the second time.[27] We must take some lessons from the experiences of our current lockdown, to endure handle another better in more healthy and productive ways.
The path ahead The CoV appears to be here to stay, and some say COVID-19 may never go away, even with a vaccine[28] Periodic exacerbations of its occurrence are predicted, which may probably involve lockdowns in waves. Responsibility of maintaining positive physical and mental well-being rests both on us and on our environment. For several, work from home may become the new norm, needing to strike a work life balance. This would entail moderating working hours, attending to relaxation, entertainment, exercise, maintaining relationships with family and friends, timely and healthy eating, sharing domestic chores, learning new hobbies, and overall in leading healthy lives. Such patterns must also be sustained over time to be effective and productive.
The media have an immense responsibility in maintaining positive mental health. The public totally depend on newspaper and television for honest and responsible reporting of news, failing which negativity will spread. Information concentrated on reporting and enhancing negative events will encourage a strong nihilism in people. Pathways to care for COVID infection need to be communicated with no ambiguity, with people being given alternate pathways should one fail, making diagnostic, and treatment options clear. They need to be kept abreast of the latest protocols for quarantine and treatment. Realistic and where possible positive information about the inputs made by all governmental and non-governmental agencies toward testing for the virus, availability of trained medical personnel, protective gear in hospitals and hospital beds must be shared on media. Psychological well-being must be addressed, with an emphasis on maintaining positive mental health, information about which can be imparted by professionals, with provision of help lines. Uncertainty disarms people and makes them helpless and vulnerable. We need to remember that stress post lockdown will be immense and each person will be called on to cope to the best of his ability. A planned approach for dealing with the lockdown will go a long way in promoting coping in one and all.
The nCoV 2019 is a pandemic of extremely vast proportions. Almost all continents have been faced with this infection that is claiming numerous lives. In these difficult health and economic times, it is but natural that people are disturbed and develop psychological distress. This study mainly evaluates the degree of psychological distress in Urban India. All subjects in our study (18 and above) experienced psychological distress due to several factors. It is thus important for the government to have policies in place to help handle these issues. The phenomenon of lockdown has been predicted to be cyclic, imposing on us the responsibility to maintain physically and psychologically well during this period, and prepare for another, should we be called upon to do so.
We thank Mr. Manjunath Sharma for his guidance in data analysis. We thank Dr. Kshamaa H G for her contribution in writing the article.
Subscribe now for latest articles and news.