Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2022.v8i1.8
Year: 2022, Volume: 8, Issue: 1, Pages: 1-7
Original Article
Kaushik Ishore1 , Ghosh Prabir2 , Abhijit Mukherjee3 , Santanu Hazra2
1Associate Professor, MJN Medical College, Coochbehar, West Bengal, India,
2Assistant Professor, Department of Microbiology, North Bengal Medical College, Sushrutanagar, Darjeeling, West Bengal, India,
3Associate Professor, NRS Medical College, Kolkata, India
Address for correspondence: Santanu Hazra, Assistant Professor, Department of Microbiology, North Bengal Medical College, Sushrutanagar, Darjeeling, West Bengal, India.
E-mail: [email protected]
Background: Incidence of hospital-acquired infection by Methicillin-resistant Staphylococcus aureus (MRSA) and Coagulase-negative Staphylococci (MRCoNS) continues to increase worldwide. Nasal carriage of Staphylococci plays an important role in the epidemiology and pathogenesis of hospital-acquired infection. They are usually introduced into the health care set up by a colonized or infected patient or health care workers (HCWs). Patients admitted to a critical care unit or intensive care unit have an increased chance of infection by these pathogens. Health care providers colonizing MRSA and MRCoNS may help in the transmission and spread of infection. Objective: To determine the prevalence of staphylococcal nasal carriage among HCWs working in intensive and critical care units of a tertiary care hospital and the antimicrobial susceptibility profile of the isolates. Result: One hundred and fifty nasal swabs were collected, 58 were from the nursing staff, 41 from doctors, and 51 were from other supporting staff. Samples from both anterior nares were collected using sterile cotton swabs, and cultured on mannitol salt agar. S. aureus and CoNS were identified by standard methods. Methicillin resistance was detected by cefoxitin disc. Of the 150 healthcare providers screened 31 (20.67%) were nasal carriers of S. aureus, 17 (11.33%) for MRSA, 81 (54%) harbored CoNS and 12 (8%) were MRCoNS. Conclusion: HCWs are the potential colonizers of MRSA and MRCoNS. They may serve as reservoirs and disseminators of MRSA and MRCoNS and should be treated with appropriate drugs. Regular screening of carriers is also required for the prevention of hospital-acquired infection.
Keywords: Nasal Carriers, Health care worker, Methicillinresistant Staphylococcus
Staphylococcus aureus remains one of the most important hospitals and community- acquired pathogen. Both methicillin-sensitive Staphylococcus aureus (MSSA) and MRSA have been implicated in a variety of hospital-acquired infections worldwide. Approximately 20% of healthy adults are persistent nasal carriers of this potential pathogen and 60%
Several studies have shown that elimination of carriage in the anterior nares, reduces the incidence of S. aureus infections.[2,10] Therefore, the knowledge of the frequency of nasal carriage of HCWs by S. aureus, MRSA, CoNS, and MRCoNS along with their antimicrobial profile is essential for proper control of hospital- acquired infections and antimicrobial stewardship. The present study was carried out to determine the prevalence of staphylococci nasal carriage among HCWs at a tertiary care facility and also the antibiotics susceptibility of the isolates.
A Cross-sectional, descriptive, hospital-based study was conducted for a period of two months (January – February 2020) in three pediatric ICUs (NICU, PICU, SNCU) and three adult ICUs (ICCU, CCU, RICU) of North Bengal Medical College and Hospital (NBMCH), India. All the healthcare personnel posted in these departments were targeted for data collection, but finally, the researchers could able to collect data from 150 subjects including doctors, nurses, technicians, sweepers (excluding the unwilling and absentee after 2 repeated visits).
Ethical approval was obtained from the Ethics Committee of North Bengal Medical College. Permission and co-operation of the college authorities and concerned departments were sought before data collection. The subjects were contacted at their workplaces during their duty hours, after briefing about the purpose and nature of the study and informed consent was obtained for interview and sample collection. Interviews of the subjects were done by using a pretested schedule. Sterile cotton swabs (Becton Dickinson Culturette Systems, Sparks, Md.) moistened with sterile normal saline was used to collect the specimens from both the anterior nares of the study subjects. The swabs were inserted into both anterior nares and rotated 5-6 times. The swabs were transported immediately to the Microbiology Laboratory for culture and further processes. Swabs were cultured on Mannitol salt agar and incubated at 37◦ C for 24 hours. The culture of the swabs and identification of S. aureus or CoNS was done by standard methods. Methicillin resistance for both the organisms was tested by Cefoxitin disc (30 µg) as per Clinical Laboratory Standards Institute (CLSI) guidelines.[11]
Antimicrobial susceptibility testing was performed by Kirby-Bauer disc diffusion method according to CLSI on Mueller-Hinton agar.[11] Zone sizes of each antimicrobial agent were recorded and interpreted as resistant, intermediate, or susceptible. Susceptibility was tested against the following 24 antimicrobials: penicillin (10 units), ampicillin, cloxacillin, co-amoxiclav, cephalexin, cefaclor, cefotaxime, amikacin, gentamicin (10µg), erythromycin (15 µg), tetracycline (30 µg), chloramphenicol (30 µg), clindamycin (2 µg), co-trimoxazole (1.25/3.75 µg), ciprofloxacin (5 µg), levofloxacin (5 µg), vancomycin (30 µg), linezolid (30 µg ), nitrofurantoin (300 µg ) and rifampicin (15 µg).
Collected data was checked for accuracy and completeness. Further, it was compiled and put in Microsoft Excel Sheet and analyzed using SPSS version 20 statistical software.
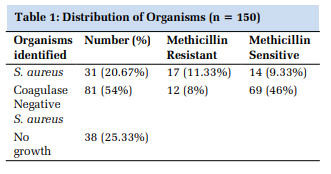
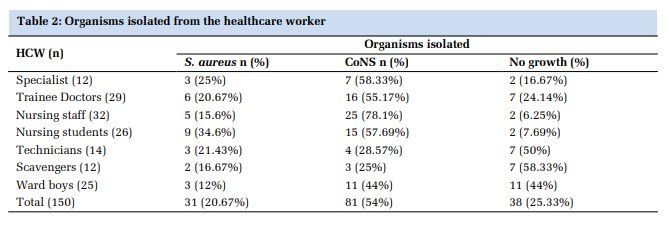
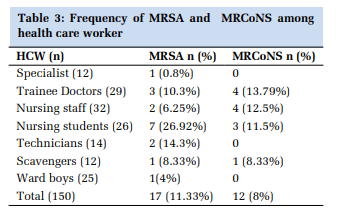
Out of 150 HCWs participating in the study, 49 (32.67%) were men, and 101 (67.33%) were women. Thirty-one (20.67%) were nasal carriers of S. aureus, 17 (11.33%) were MRSA, and 14 (9.33%) were methicillin-sensitive. Out of 81 (54%) CoNS isolates, 12 (8%) are MRCoNS and 69 (46%) were sensitive to methicillin. (Shown in Table 1 and Table 2) The frequency of carriage rate of S. aureus, MRSA, CoNS, and MRCoNS in various groups of staff members are given in Table 2 and Table 3. Twelve specialists participated in the study and 3 were a carrier for S. aureus, 1 for MRSA.
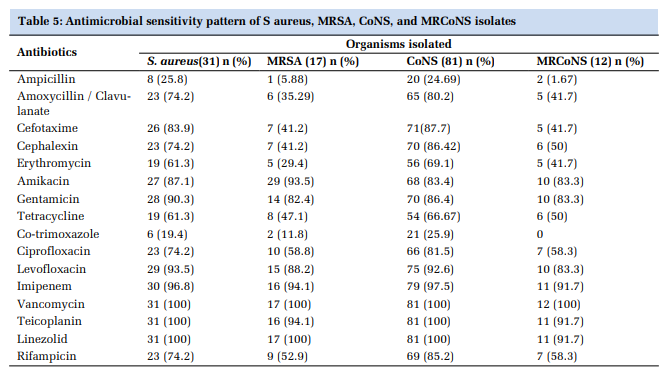
The highest carriage rate for S. aureus was seen in nursing students (34.6%). MRSA was isolated from anterior nares of 26.92% of nursing students, 14.3% of technicians, and 10.3% of postgraduate trainee doctors. MRCoNS was isolated from 20 scavengers, 13.79% of postgraduate trainee doctors, 12.5% of staff nurses, and 11.5% of nursing students. (Table 3) lowest was in the NICU. (Table 4) The susceptibility profile against the antibiotics tested of all the isolates i.e. S. aureus (n=31), MRSA (n=17), CoNS (n=81), and MRCoNS (n=12) is shown in Table 5.
In the present study, MRSA and MRCoNS represent a variable drug-resistant pattern. All the isolates obtained were universally susceptible to Vancomycin and Linezolid. More than 90% of S. aureus and CoNS were susceptible to Imipenem, Levofloxacin. MRSA and MRCoNS isolates show the highest resistance to Ampicillin, Co-trimoxazole, The resistance rate in MRSA isolates was more than that of MRCoNS.
Staphylococci are the major cause of hospitalacquired infections. MRSA and MRCoNS are resistant to all β-lactam antibiotics and are considered the most important cause of hospital-acquired infections around the world. The most effective way of preventing the spread of MRSA and MRCoNS in the hospital setting requires the detection of colonized HCWs and measuring the associated risk factors of colonization.[12] The rate of Methicillin resistance has increased considerably and according to different studies, 60 – 85% of strains are resistant to Methicillin.[13–15] With increasing Methicillin resistance these organisms are also becoming resistant to most other antibiotics in use. So, the detection of the prevalence of MRSA and MRCoNS in the healthcare setting has never been more important due to the increasing frequency of MRSA and MRCoNS over the years and the limited therapeutic choices available. Screening for the carriage of staphylococci is essential for hospital-acquired infection control practices. Eradication of nasal carriage of staphylococcal reduces the risk of spreading of infection in patients.[2,10]
In the present study, 20.67% and 54% of HCWs were nasal carriers of S. aureus and CoNS, respectively. A higher nasal carriage rate (33% and 48%) for S. aureus of HCWs has been reported in studies from Pakistan and Saudi Arabia.[16,17] Prevalence of nasal carriage of S. aureus in other countries is also different (16.8-56.1%).[2] The nasal carriage of CoNS among health care workers was 32.8% in the study by Agarwal et. al, however, Kaur and Narayan (52.14%) and Akhtar (73.3%) showed a higher prevalence.[18–20] This difference may be due, in part, to differences in geographical distribution, differences in the quality and size of samples, and the culture methods used to detect S. aureus or maybe the biological characteristics of the S. aureus strain and/or infection control practices.[21]
Out of 150 HCWs, the carriage rate for MRSA was 17 (11.33%) and 12 (8%) were MRCoNS. Varying rates for MRSA carriage by HCWs were reported in India (39.7%) and Pakistan (14%).[17,22] Alsulami SO et. al. also showed a higher nasal carriage of MRSA (24%) and MRCoNS (42%) among HCW.[12]
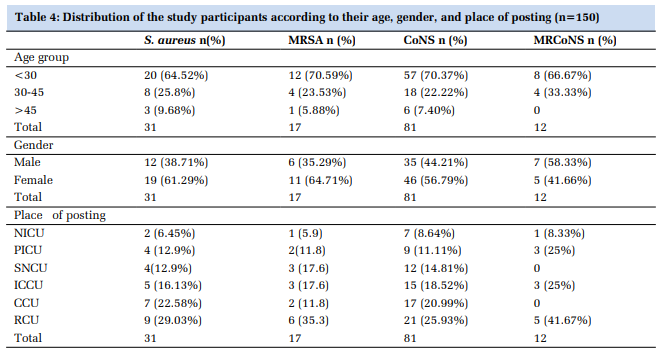
HCWs having direct patient contact have a higher carriage rate than those who have lesser contact. The carriage rate of S. aureus in HCWs like technicians (21.43%), staff nurses (15.6%), trainee doctors (20.67%), and nursing students (34.6%) was also high and can partially be related to direct patient contact. Carriage of CoNS is also high in nursing staff (78.1%), nursing students (57.69%), specialists (58.33%), trainee doctors (55.17%), and ward boys (44%). In this study, the frequency of MRSA and MRCoNS carriage varied between different departments. The prevalence was highest in RCU (35.3% & 41.67%), ICCU (17.6% & 25%), and SNCU (17.6%), which was close to the findings obtained by Altimbas et al.[23]
MRSA and MRCoNS nasal carrier rates were high (70.59% and 66.67%) in the age group below 30 years and less (5.88%) in the age group above 45 years. Female HCWs harbored bacteria significantly more often than males. However, Majumder et al in a study from this region showed no significant gender difference in the rates of nasal carriage.[24]
These findings were contrary to that observed in the study done in Saudi Arabia which showed a higher carriage rate in the extremes of age group.[25]
Various topical agents including; mupirocin, bacitracin, and fusidic acid ointments, and oral agents like; trimethoprim-sulfamethoxazole, ciprofloxacin, doxycycline, rifampicin, and clarithromycin have been used separately or in combination in different settings for eradication of S. aureus and MRSA nasal carriage in HCWs. Mupirocin, the agent recommended for eradication of staphylococcal nasal carriage, was not tested due to the non-availability of discs for susceptibility testing.[26] However, the role of intranasal application of mupirocin in eradicating colonization in patients who carry the organism at multiple body sites is doubtful.[27] Therefore, a broader range of antibiotics were tested for suitable therapy. Antimicrobial susceptibility for CoNS was also tested as CoNS nasal carriers can disperse these organisms in the environment.[27] In the present study, all the isolates including S. aureus, MRSA, CoNS, and MRCoNS were susceptible to vancomycin, and Linezolid. Imipenem, a broadspectrum antibacterial agent, also injectable and expensive, is mostly kept as a reserve drug for life-threatening infections, and has not been used in staphylococcal decolonization. Levofloxacin, a respiratory fluoroquinolone, remains the option that can be used for eradication of any of staphylococcal nasal carriage as it has a very good nasal penetration and its activity better than ciprofloxacin.[28,29] Whenever required in special settings like hemodialysis units to eradicate CoNS nasal carriage most of the fluoroquinolones can be used. Rifampicin, a firstline antituberculous drug also, has been used in various studies for the eradication of staphylococcal nasal carriage and has shown variable activity against S. aureus and MRSA.[30] However, due to the reason that S. aureus quickly develops resistance to rifampicin monotherapy,[31] and secondly being reserved as the anti-tuberculosis drug cannot be opted for decolonization.
The nasal carriage rate in HCWs for S. aureus, MRSA, CoNS, and MRCoNS was 20.67%, 11.33%, 54%, and 8 % respectively. Most of these MRSA & MRCoNS showed considerable resistance to routinely used antistaphylococcal antibiotics. Vancomycin is the only antibiotic to which all isolates were sensitive. More than 90% of isolates were sensitive to Linezolid and Teicoplanin. Regular careful monitoring and surveillance of Staphylococcal nasal carriage among health care workers is essential to reduce the burden as they are fast evolving into pathogens and treatment options are becoming limited.
Subscribe now for latest articles and news.