Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.014
Year: 2021, Volume: 7, Issue: 2, Pages: 85-89
Original Article
Ranita Roy Chowdhury1 , Sougata Kumar Burman1 , Jayeeta Mukherjee2 , Malabika Misra3 , Gairik Bera4
1 Associate Professor, Department of Obstetrics and Gynecology, College of Medicine and JNM Hospital, West Bengal University of Health Sciences, Kalyani, West Bengal, India,
2 Assistant Professor, Department of Obstetrics and Gynecology, College of Medicine and JNM Hospital, West Bengal University of Health Sciences, Kalyani, West Bengal, India,
3 Associate Professor, Department of Obstetrics and Gynecology, JIMS and Hospital, Kolkata, West Bengal, India,
4 Post Graduate Trainee, Department of Obstetrics and Gynecology, College of Medicine and JNM Hospital, West Bengal University of Health Sciences, Kalyani, West Bengal, India
Address for correspondence:
Malabika Misra, Department of Obstetrics and Gynecology, JIMS and Hospital, Kolkata, West Bengal, India. Phone: +91-9830952305. E-mail: [email protected]
Background: Adequate antenatal care (ANC) services are the key to a healthy pregnancy outcome. Utilization of ANC services is of foremost importance in reducing maternal mortality and morbidity in India. ANC is one of the main components of maternal health. Low socioeconomic status, illiteracy, lack of awareness, and limited health-care options lead to underutilization of maternal health-care services.
Objective: The study is aimed to assess the utilization of ANC services in the recently delivered females.
Materials and Methods: The present study is a hospital-based cross-sectional observational study conducted in the Department of Obstetrics and Gynecology, COMJNM, from July 2019 to September 2019. All the patients admitted under a particular unit have been taken into account. A pre-designed and pre-tested structured questionnaire was administered to all the patients who had delivered in this tertiary care teaching hospital of Nadia district, West Bengal, India. The data were tabulated, analyzed, and presented in proportions.
Results: During the study, 305 rural and semi-urban, recently delivered females were interviewed.
Conclusion: In spite of persistent efforts of the Government of India to improve maternal and child health services in the rural parts of the country, the results reflect the areas of concern. There is an innate need is to upgrade the quality and accessibility of antenatal care service as well as public health awareness, especially in the remote areas/village areas.
KEY WORDS: : Antenatal care, maternal health, utilization of antenatal services.
Antenatal care (ANC) is the care of woman during pregnancy which can be provided by doctors, midwives, or health-care professionals. The primary aim of ANC is to achieve, at the end of the pregnancy a healthy mother and a healthy baby. Maternal mortality still remains a cause of concern in developing countries. About 810 women die from pregnancy or pregnancy-related complications around the world every day.[1] An estimated 295,000 women died during and following pregnancy and childbirth in 2017.[1] Most of these deaths occurred in low-income countries.[2] About 88–98% of the maternal deaths could have been avoided by proper care during pregnancy and labor.[3] Maternal care means ANC and should begin from the early stages of pregnancy. Women can avail ANC services either through a health-care center or health care workers where such services are provided by home visits. The World Health Organization recommends a minimum of four ANC visits to reduce the risk during pregnancy. The purpose of ANC services is early identification of high-risk pregnancies, monitor signs of complications, detect and treat preexisting and concurrent problems during pregnancy, provide counseling and advice on nutrition during pregnancy, personal hygiene, postnatal care, and newborn care related issues. Providing ANC during pregnancy is one of the most significant issues in lowering maternal morbidity and mortality.[4] Regular antenatal visits improve awareness about care during pregnancy and delivery. It gives the beneficiary and their families, familiarity with regard to proper maternal care facilities. This, in turn, help them to contact the health-care system during the time of crisis at the earliest possible time.[5] In India, the Reproductive and Child Health Program has a powerful impact on the health of both the mother and the baby RCH Program aims at providing antenatal checkups which include checking weight and blood pressure, immunization, iron, and folic acid (IFA) prophylaxis.[6] In India, the government provides these services through the health centers at and domiciliary visits by health care workers.
The former indicates the voluntary utilization of services by mothers and latter about the quality of care of the services. Nevertheless, ANC services are not uniformly distributed in the society.[7] The disparity between the rich and poor underserved communities is increasing.[8,9] Furthermore, differences exist between states, districts, and urban and rural areas of the same state. This could be due to underutilization of maternal health-care services due to poor accessibility, affordability, illiteracy, and social and cultural factors which significantly affect the maternal and child health in the general population.[10,11] This paper is based on observations related to knowledge, perceptions, and utilization of ANC services among women of age 15–45 years.
administered for this purpose. Detailed history of the females including sociodemographic profile and information regarding utilization of ANC services such as time of registration of pregnancy, number of antenatal visits, immunization status against tetanus, consumption of IFA tablets, and basic pregnancy investigations. The data thus collected were tabulated, analyzed, and expressed in percentage for categorical variables.
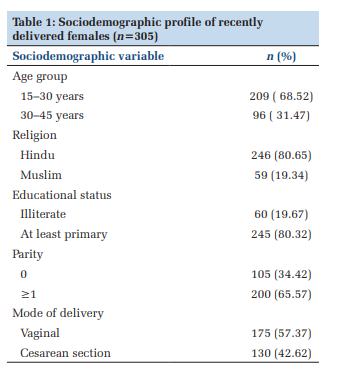
During the tenure of the study, 68.5% of females were in the 15–30 years age group while the rest 31.47% were more than 30 years. About 80.65% were Hindus while 19.34% were from Muslim families. Around two-third of the patients were parous while 80.32% of the females had primary school education or primary school dropout. Majority of them about 57.37% were delivered vaginally while 42.62% had undergone cesarean section (Table 1).
Table 2 and Figure 1 gives us an idea about the utilization of ANC services. The results reveal that 88.52% had registered after 12 weeks of gestation and only 11.47% before 12 weeks of pregnancy. In comparison to National Family Health Survey, data significantly less number of women are registered in the 1st trimester.[13] Majority 64.59% had undergone more than 4 visits while 65.57% had taken IFA tablets. Immunization status of TT was more than 98% while hemoglobin reports were available for more than 96% of the study group. Venereal disease research laboratory (VDRL), hepatitis B antigen, and human immunodeficiency virus (HIV) reports were available with more than 85% of the females whereas anti-hepatitis C virus (HCV) with only 46.8% of them. Blood grouping, postprandial glucose, and urine estimation were present in a good proportion of patients. The percentage of females with the first trimester ultrasound was 9.83%. A total of 6 patients (1.96%) did not seek for ANC at all.
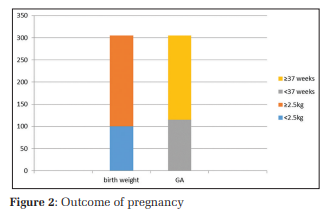
The pregnancy outcome has been illustrated through a bar graph Figure 2 showing the proportion of low birth weight and preterm against those weighing >2.5 kg and >37 weeks of gestation. Thus, this implies that majority of the patients delivered at term with an average size baby. Seven of the babies delivered were very low birth weight and two macerated stillborn.
Pregnancy requires quality care and specialized care. It is generally agreed to be a preventive activity. Poor utilization of antenatal services reflects cultural and socioeconomic constraints as well as perceptions regarding accessibility of facilities and quality of care. ANC is meant to promote good health in women by prevention, early detection of complications, and treatment of adverse maternal and perinatal outcome. Majority of the females 80.65% were Hindus similar to results by Kakati et al. and the predominantly within 30 years of age.[14] At least 80% of them went to primary school out of which many might have been a school drop out against 19% who were completely illiterate. Age of marriage, parity, and mode of delivery are not statistically significant variables to affect the antenatal visits.[12]
Only 11.47% of beneficiaries registered before 12 weeks of gestation which is incongruent with previously published data.[14] Similarly, Gupta et al. in an earlier study reported only 9.9% of the females being registered in the first trimester.[15] Threefourths (64.5%) of the participants had more than 4 antenatal visits which are similar to that reported earlier.[15] It is documented that early registration leads to better utilization of ANC. It explains early registered females avail four or more antenatal visits. Thus, promoting early pregnancy registration has a positive impact on the maternal health in the long run. National Family Health Survey data show that 58.6% had antenatal check-up in the first trimester and 51.2% of women had at least four ANC visits.[13] The results have further revealed that 98% of them had received both doses of tetanus. Bhimani et al. [16] and Dubey et al. [17] in their studies reported 82% and 75% of the subjects fully immunized with two doses of tetanus in their respective studies. Intake of IFA tablets among the participants has been quite high of about 65% compared to the previous studies by Bhimani et al. which were 48% but similar to the study conducted by Kakati et al. who reported 71.6% intake of IFA. About 96% and 93% of the respondents had undergone hemoglobin estimation and blood grouping, respectively. VDRL and hepatitis B reports were available with 87.8% of the females while hepatitis C was present with 46% of them which is consistent with a previous study.[18] About 91.8% of them availed the HIV test and urine examination during ANC. A postprandial or fasting plasma glucose estimation was present in 81.9% of females while only 9.83% had undergone first trimester ultrasound. A less number of the first trimester registration significantly affect the number of antenatal visits which, in turn, affect the proportion undergoing laboratory investigations and first trimester ultrasound. Among the various variables in relation to ANC visits, age groups, religion, literacy status, type of family, and occupation of the mother were found to be statistically significant in an earlier study.[12]
Lack of knowledge about the significance of antenatal services usually results in inadequate utilization of maternal health services. Literacy, awareness campaigns, and women empowerment have a significant impact on early and proper utilization of ANC services.[15] The previous studies revealed a significant association of utilization of ANC with age, religion, place, mode of delivery, and parity.[14] Similar studies reported a greater participation of literate women in maternal health-care delivery system compared to their illiterate counterparts.[13,15-18]
The study lacks generalization as this was a crosssectional observational study conducted in a teaching hospital with tertiary care facility.


Proper ANC is the only way to reduce maternal mortality and morbidity as the complications of pregnancy can either be prevented or be detected early by timely antenatal checkup. General awareness in society should be raised on the importance of the first trimester visits as well as the number of ANC visits, particularly among the pregnant women and their family members. There is a common misconception among the society is that pregnancy is a physiological event so it needs negligible medical support. Therefore, they are least bothered about regular checkup. Emphasis should further be on easy accessibility, reduction in cost, supporting pregnant women of extreme age and backward societies, follow the recommendations of ANC care and timely identification, and more vigilant care of high risk cases. Ministry of Health and Health Care Services, ANC professionals, and community level health workers have an important task in raising consciousness on this matter.
Subscribe now for latest articles and news.