Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i1.25.208
Year: 2026, Volume: 12, Issue: 1, Pages: 30-36
Original Article
Maheen Nazir 1, Ghulam Mohammad Bhat 2, Sheikh Tousia 1, Ishfaq H Bhat 3
1Assistant professor, Postgraduate Department of Anatomy, Government Medical College, Srinagar, Jammu & Kashmir, 190010, India.
2Professor and Head, Postgraduate Department of Anatomy, Government Medical College, Srinagar, Jammu & Kashmir, 190010, India.
3Assistant professor, School of Commerce, Narsee Monjee Institute Management Studies, Navi Mumbai, Maharashtra, India.
Address for correspondence:
Ghulam Mohammad Bhat, Professor and Head, Postgraduate Department of Anatomy, Government Medical College, Srinagar, Jammu & Kashmir, 190010, India.
E-mail: [email protected]
Received Date:03 June 2025, Accepted Date:06 October 2025, Published Date:27 March 2026
Introduction: Bullying has been a problem across different professions, but only recently has the phenomenon been acknowledged as a serious issue, particularly in medical education. Healthcare providers and medical students are a special population when it comes to bullying. Given the negative consequences of bullying on the mental health and well-being of victims, it is vitally important to understand the reasons that trigger the emergence and development of this social phenomenon. However, the literature on this in India is limited. This study aimed to assess the prevalence and forms of bullying, its effects, and risk factors among healthcare professionals across India. Methods: A cross-sectional study was conducted among 541 participants, including students, residents, nurses, and faculty of Government Medical and Paramedical colleges of Jammu and Kashmir, India, using a pre-validated questionnaire based upon “The Workplace Aggression Research Questionnaire (WAR-Q)” It captured data on demographics, experiences of specific negative behaviours, sources of bullying, its impacts and awareness of policies. Logistic regression was employed to analyze the data. Results: 63.4% reported experiencing at least one bullying behaviour in the past year. Verbal abuse, humiliation, and academic or clinical exploitation were most commonly faced. Bullying negatively impacts mental health, performance, and persistence. Seniors and consultants were key perpetrators. Awareness of anti-bullying policies was low. Conclusion: This first study in Kashmir focused on workplace bullying among healthcare professionals, revealing a high prevalence of this issue. Urgent, multifaceted interventions centered on systemic reforms, accountability, accessible reporting, and cultural shifts are warranted to address this issue.
Keywords: Bullying, Ragging, Medical Education, Verbal insults, Humiliation, Social exclusion, Workplace-based harassment
Bullying and harassment in medical education have become a concerning global issue receiving increasing attention in recent years [1, 2]. This mistreatment encompasses repeated aggressive behaviours that harm victims physically, psychologically, or professionally, reflecting abuse of power differentials in the medical hierarchy [3]. Several studies have revealed alarming prevalence rates, with 42% to as high as 93% of medical participants reported experiencing at least one bullying behaviour during training [4]. Types of bullying include physical harm, verbal insults, humiliation, social
exclusion, abusive hazing rituals, cyber-bullying, sexual harassment, and academic sabotage or exploitation. Key perpetrators tend to be senior students, residents, and in some cases, faculty [5]. Association has been demonstrated between bullying victimization and higher risks of depression, substance abuse, attrition, suicide ideation, and erosion of professionalism and competence among medical trainees [6, 7]. Thus the problem undermines student welfare while also negatively impacting the quality of graduating physicians [2].
Recently, in India, extreme bullying cases resulting in severe injuries or deaths have brought some attention to this issue [8]. Nationwide regulations were enacted such as the 2009 UGC Prohibition of Ragging in Higher Education Institutions Regulations that aim to curb ragging through strict monitoring committees, reporting systems, and punitive measures [9]. However, there remains limited literature on the nature and impacts of bullying experienced by India's large medical student population. Of the few small studies conducted, bullying
prevalence was 31-45% among samples of medical students [10, 11]. Disturbingly, over 75% of West Bengal students reported facing threats, and physical or psychological harm [12]. Qualitative findings also reveal normalized verbal abuse and hazing rituals that erode medical students and medical professionals' mental health and confidence in India [13]. This initial evidence indicates the need for updated national data.
Moreover, India’s complex socio-cultural environment characterized by rigid hierarchies and various axes of oppression likely exacerbates bullying risks, especially for disadvantaged groups [13]. There are also rising student depression and suicide rates linked to high stress, discrimination, and dissatisfaction in India’s medical training culture [14, 15]. Hence elucidating this issue is an urgent first step toward impactful reforms. Promoting the well-being of medical professionals will nurture competent, ethical physicians to advance India’s healthcare. With over 550,000 doctors-in-training, [15] the far-reaching implications underscore the necessity and timeliness of this study.
Forms and prevalence of Bullying: Varied bullying behaviours inflicted on medical professionals in India evident in the literature include physical assault, sexual harassment, verbal abuse, humiliation rituals, and academic exploitation [13, 16]. Qualitative insights reveal normalized practices ranging from seniors forcing juniors to run errands, public stripping, and financial extortion to signs of physical harm. Meanwhile, rates of self-reported bullying across prior regional surveys ranged from 31%-75% [17, 18]. Notably, 75% of West Bengal medical students reported facing threats, and physical or psychological harm [12]. Another study shockingly found that 52% of Kolkata students experienced physical ragging and 90% underwent humiliation rituals that left psychological scars [18]. However others estimate lower bullying rates, highlighting the need for updated national prevalence data through standardized methodology [10].
Key perpetrators and associated factors: Senior students and residents were the most commonly cited bullies across studies in Indian medical schools [13, 16]. Potential socio-demographic factors like gender, rural background, minority status, and academic performance perceived as risks for ragging victimization remained unexplored in the Indian context [4, 5].
Impacts of bullying on victims: Global evidence links bullying with higher depression, substance abuse, and attrition risks among medical students. Similar impacts are speculated but empirical data in the Indian context is lacking barring a few non-generalizable qualitative studies [13, 16]. One study disturbingly found medical students trivializing peer suicides as outcomes of failure to cope with permissible ragging, indicative of grave normalization [19].
Research gaps: The bullying research conducted previously solely focuses on prevalence with centralized samples. Forms of abuse are also described vaguely without measurement. The roles of gender, hierarchy, academic pressures, or institutional cultures remain unprobed in perpetrating toxic environments. Rigorous studies quantifying specific bullying behaviours and their mental health correlations are warranted [5]. Platforms allowing anonymous testimonies could help uncover the problem’s magnitude. Lastly, more implementation analyses of preventive strategies are needed to strengthen policy responses. The global call for zero-tolerance of abuse in medical education needs resonance in India to safeguard future doctors’ welfare.
Preliminary evidence indicates widespread bullying in Indian medical schools. The culture of trivializing mistreatment enables severe physical, sexual, and mental abuse that can have tragic consequences for students not conforming to expected hierarchies. Understanding this complex phenomenon and its impacts through forthcoming in-depth mixed-method studies is the first step toward creating ethical, safe educational environments for nurturing competent Indian physicians. The stakes for India’s healthcare ecosystem warrant urgent action by regulators to curb ragging and uphold standards of dignity for these vulnerable trainees [5]. These research gaps suggest a need for more comprehensive research that: explores the "why" behind bullying- investigates the root causes of bullying behaviour, such as power dynamics, social hierarchies, academic pressure, and personal factors; examines the impact of bullying- study the short-term and long-term consequences of bullying on victims, including mental health, academic performance, and career trajectories; investigates the effectiveness of interventions- evaluate the efficacy of existing anti-bullying programs and develop more targeted and effective interventions, and employs diverse sampling methods- include data from a wider range of medical schools including paramedical colleges to ensure a more representative understanding of the issue [10, 13]. By addressing these limitations, the present research can provide a more nuanced and comprehensive understanding of bullying in Indian medical schools, leading to more effective prevention and intervention strategies.
This study analyses bullying among healthcare professionals in Jammu and Kashmir. Specific objectives were determining prevalence, understanding impacts, identifying risk factors, and assessing anti-bullying policy awareness to shape interventions promoting dignity and inclusion.
This prospective cross-sectional study utilized an online questionnaire survey methodology to assess bullying experiences among 541 healthcare professionals including students, residents, nurses, and faculty of Government Medical and Paramedical colleges of Jammu and Kashmir, India. The project was cleared by the Institutional Review Board vide communication: IRBGMC/ANAT 321, dated 20/08/2022. As the study was a questionnaire- based survey and a purposive sampling approach was employed, the potential for selection bias was reduced by making the survey more confidential and anonymous. The questionnaire link was disseminated using WhatsApp (Facebook Inc., California, USA). The questionnaire was divided into three sections. Section A consisted of 5 items covering participants' demographic information, The survey captured self-reported data at a single point to determine prevalence and patterns. The design aligned with objectives to estimate workplace bullying prevalence and experiences, using a predesigned questionnaire “Based upon the Workplace Aggression Research Questionnaire (WAR-Q)” [20] WAR-Q is a tool designed to assess workplace aggression. It's not specifically focused on bullying, but it can be adapted to help identify potential risk factors contributing to a bullying environment. The WAR-Q can be a valuable tool in assessing workplace bullying risk by helping organizations understand the broader context within which bullying might occur. The questionnaire captured data on demographics, experiences of specific negative behaviours, sources of bullying, its impacts, and awareness of policies. The participants were from diverse demographics including undergraduate students, senior residents, paramedics, and faculty members to examine bullying across roles. Participants were invited to voluntarily self-report their experiences through an online survey. Informed consent was obtained from all participants. Anonymity was ensured through data encryption and confidentiality protocols.
Data from the filled questionnaires were extracted and exported to Microsoft Excel 2016 (Microsoft Corp., Redmond, WA). The data were cleaned and then exported to Statistical Package for Social Sciences (SPSS), version 22 (IBM Corp., Armonk, NY) to determine prevalence, associated factors, impacts, and awareness. In the study, logistic regression was employed to analyze factors associated with bullying victimization among healthcare professionals. This method was appropriate as the dependent variable—whether a participant experienced bullying—was binary (yes/no). Logistic regression enabled identifying and quantifying relationships between independent variables, such as role, background, education level, and workload, and the likelihood of experiencing bullying. By calculating odds ratios, the analysis highlighted significant predictors, such as junior roles and high workloads, which increased vulnerability to bullying. The justification for using logistic regression lies in its ability to handle categorical outcomes and provide clear insights into the strength and significance of associations, thus aiding in understanding the key factors contributing to workplace harassment.
Frequency distributions, cross-tabulations, and logistic regression examined patterns in experiences, impacts, and suggestions. This cross-sectional study included 541 participants, with 55.8% (n=302) males and 44.2% (n=239) females. Participants spanned from year one through five, representing 17% to 21% of the sample. The majority were aged 26-30 years (48.6%, n=263) and were urban residents (71.2%, n=385). Overall, 63.2% (n=342) of participants reported experiencing ≥1 bullying behavior in the past year. Prevalence was highest among first-years (81%) versus 49% in final-years. No major gender differences existed (males - 62%; females 64%). Participants of rural backgrounds reported slightly higher bullying (69%) than urban participants (61%).
| Parameters | Number | Percentage | |
|---|---|---|---|
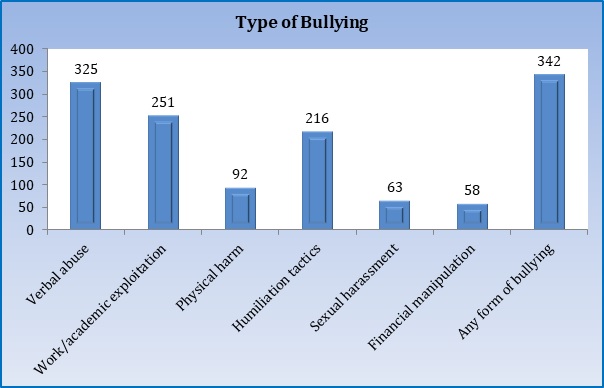
| Type of Bullying (n=541) | Verbal abuse | 325 | 60.1 |
| Work/academic exploitation | 251 | 46.4 | |
| Physical harm | 92 | 17.0 | |
| Humiliation tactics | 216 | 40.0 | |
| Sexual harassment | 63 | 11.6 | |
| Financial manipulation | 58 | 10.7 | |
| Any form of bullying | 342 | 63.2 | |
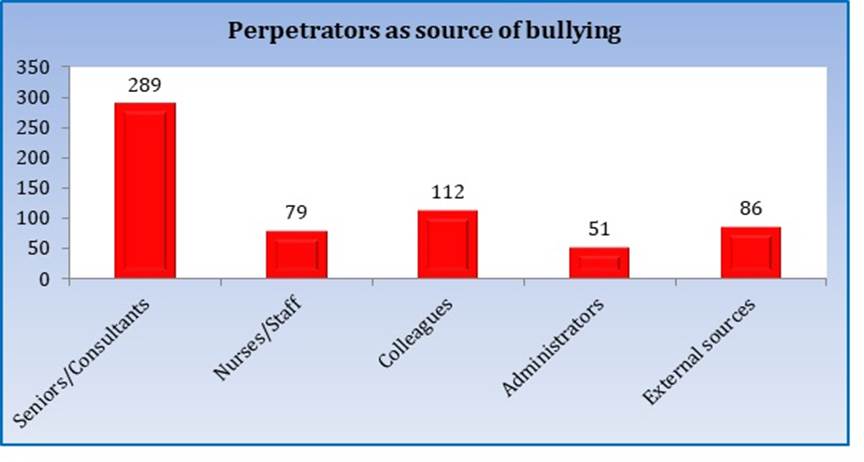
| Perpetrators as the source of bullying (n=342) | Seniors/Consultants | 289 | 84.5 |
| Nurses/Staff | 79 | 23.1 | |
| Colleagues | 112 | 32.7 | |
| Administrators | 51 | 14.9 | |
| External sources | 86 | 25.1 | |
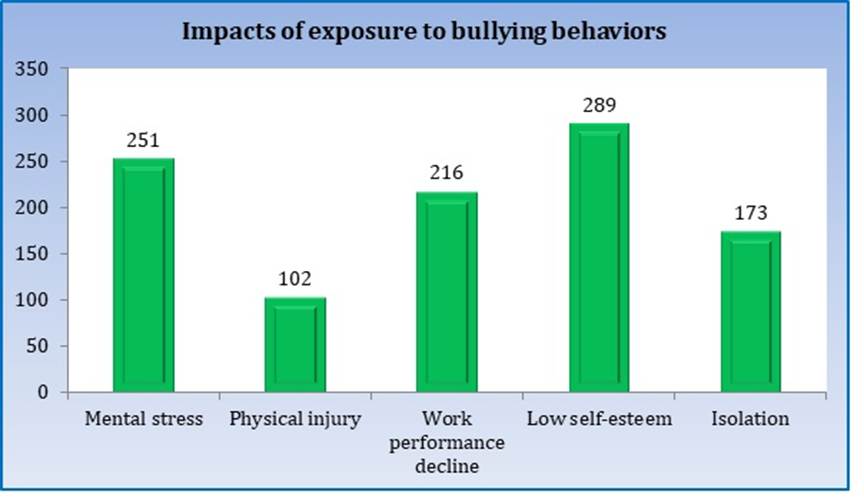
| Impacts of exposure to bullying behaviours (n=342) | Mental stress | 251 | 73.4 |
| Physical injury | 102 | 29.8 | |
| Work performance decline | 216 | 63.2 | |
| Low self-esteem | 289 | 84.5 | |
| Isolation | 173 | 50.6 | |
[Table. 1], [Fig. 1] show bullying behaviour among respondents, perpetrators identified as the source of bullying behaviour, and impacts faced due to exposure to bullying behaviours. As shown, the most commonly faced bullying behaviours were verbal abuse (60.1%, n=325), humiliation (40.0%, n=216), academic exploitation (46.4%, n=251), physical harm (17.0%, n=92), and sexual harassment (11.6%, n=63). 28% reported facing weekly recurring incidents indicative of normalized environments. 74% of victims (n=251) reported mental stress. 84% (n=289) described damaged self-confidence and 63% (n=216) reported negative academic performance. 30% (n=102) sustained physical injuries due to bullying acts. 84% of victims (n=289) identified seniors, 51% (n=173) identified residents as bullies. 27% implicated faculty while 15% reported administrators.
Only 46% were aware of anti-ragging policies and under 20% knew about complaint mechanisms. Over 35% were uncertain about anonymity assurances and 70% had not witnessed punitive actions - indicating poor visibility of implemented redressal frameworks.
[Fig. 2] shows the logistic regression analysis of factors associated with the increased likelihood of bullying victimization. It shows junior roles and high workload as major factors for falling victim to bullying. 46.4% of the participants were generally aware that anti-bullying policies exist in their workplace, but the specific details and consequences may be less clear (66.2%).
Bullying can have devastating effects on victims, leading to emotional distress, decreased self-esteem, and even physical health problems. It can also negatively impact the bullies themselves, increasing their risk of engaging in antisocial behavior later in life. The present cross-sectional study conducted among 541 participants including students, residents, nurses and faculty at a medical college in Jammu and Kashmir provides the first focused analysis of workplace bullying in this setting. Key findings, interpreted in light of comparisons with prior studies, affirm concerns around normalized abuse carrying adverse consequences - warranting prompt action.
A workplace bullying prevalence of 63.4% determined through this study exceeds rates of 31-45% noted in other Indian surveys [11, 12].
| Study | Setting | Prevalence | Key Forms | Impacts | Perpetrators | Policy Awareness |
|---|---|---|---|---|---|---|
| Present Study (2024) |
Government Medical
|
63.4% | verbal abuse, humiliation tactics, and academic exploitation |
Mental stress Physical injury Work performance decline Low self- Isolation |
Seniors, residents and faculty | 46.4 % |
| Artino et al., (2010) [13] |
Medical school, USA | 59% | Public humiliation, verbal abuse | Depression, anxiety | Residents, nurses | 18% |
| Nagata-Kobayashi et al., (2006) [14] |
Nursing school, Japan | 34% | Verbal abuse, isolation | Psychological distress | Senior nursing students | 14% |
| Baldwin Jr et al., (1998) [15] |
Dental school, UK | 36% | Belittling, physical threats | Fear decreased confidence. | Senior students and faculty | 29% |
| Sheehan et al., (1990) [16] |
Medical school, Australia | 84% | Verbal harassment, humiliation | Burnout, suicidal ideation | Residents, nurses, faculty | 19% |
| Owoaje and Ndubusi (2010) [17] |
Medical schools, Nigeria | 80% | Physical assault, sexual harassment | Physical injury, depression | Fellow students and residents | 31% |
| Frank et al., (2006) [18] |
Medical schools, USA | 69% | Verbal abuse, humiliation | Anxiety, depression | Attendings and residents | 23% |
| Rees CE and Monrouxe LV (2011) [19] |
Medical School, New Zealand | 71% | Belittling comments, isolation | Stress, low self-esteem | Consultants, nurses | 28% |
It also surpasses the highest global estimate of 59% across American medical schools [21]. These discrepancies could reflect underreporting in smaller samples or variations in assessed behaviours. Nevertheless, frequent exposure reported by over a fourth of respondents signals unsafe environment. Higher vulnerability among juniors as evident through 81% prevalence among first-years aligns with prior research identifying power dynamics as enabling forces [14]. Comparable gender trends match other coeducational medical schools wherein marginal differences existed between males and females - unlike Asian nursing colleges demonstrating higher risks in female predominance [22, 23]. These patterns reiterate the ubiquitous nature of toxicity in medical training hierarchies across roles and demographics. However specific forms of bullying can be discriminatory, necessitating disaggregated data. The majority of observations imply healthcare providers in a more senior capacity (consultants/clinical faculty/supervisors) as being the main perpetrators of bullying in healthcare settings. The high prevalence of bullying points towards a lack of awareness or concern by concerned stakeholders
including the professional regulatory bodies, which can make the perpetrators potentially authoritative figures within their institutions/workplace [24]. A study in Tanzania, it was found out that 34.7% and 28.7% of students had directly experienced bullying and witnessed bullying respectively [25].
Predominant bullying behaviours encompassed verbal abuse, humiliation tactics, and academic exploitation - aligning with student testimonies across India [14, 15]. However underreporting of sexual misconduct cannot be ruled out. Disturbingly though, 17% of physical assault success rates below 10% in prior Asian studies - indicating extreme normalization of violence [3, 22]. These behaviours left deep psychological scars with three-fourth of respondents affirming mental health concerns and the majority struggling with confidence, performance, and persistence. Such trends resonate with literature on adverse mental health sequelae including depression, attrition, and suicidal risks associated with medical school bullying exposure [6, 14]. While comparable empirical outcome data remains scarce in India and is limited to speculations, 30% of physical injuries and stress corroborate with qualitative insights on ragging driving student distress.14 Potential long-term professionalism erosion warrants deeper investigation - though linked with mental health impacts [22]. Overall, these trends emphasize the human costs of unchecked abuse transcending short-term harms.
As established through global evidence, seniors were identified as primary aggressors by the majority of victims [3, 14]. Their enabling position to exercise unchecked authority without accountability due to skewed power balances and unquestioned hierarchy traditions sustains toxicity. However, consultant and administrator roles in 14% of cases highlight system-wide culpability. Potentially, juniors face heightened vulnerability due to pressures to comply for survival - explaining a stronger likelihood among rural, lower-educated groups. Though conjectured based on caste, gender, and other marginalizations, intersectional risk factors are yet to be examined [5, 14]. Paralleling research across India, under 50% of participants exhibited awareness of regulations despite stringent prohibitions - indicating superficial implementation [11]. Poor visibility of complaint channels and actions against perpetrators sustain a culture of abuse by signalling impunity. Such trends question purported crackdowns after extreme ragging cases, suggesting the need for transparency in monitoring and justice delivery [10]. Overall, persistent high bullying rates in Jammu and Kashmir with corrosive impacts across echelons of the medical education hierarchy mirrors concerns voiced through emerging Indian literature. Prevailing environments enabling abuse require systematic reforms upholding equity and accountability at a national scale - though localized cultures warrant context-specific redressals. Strengthening policy prohibitions with accessible reporting, victim support, and cultural recalibration can protect the dignity of medical trainees.
Workplace bullying is largely driven by stressful work environments and toxic organizational cultures, as described by the work environment hypothesis and strain-based mechanisms. Stress and unresolved conflicts allow negative behaviors to escalate, often with little accountability. Cyberbullying—a persistent, electronic form of aggression—poses additional unique challenges, as traditional anti-bullying strategies may not fully address its complexities [27-28].
Effective measures include:
Causality cannot be established due to the cross-sectional design, which only captures data at a single point in time. Self-reported responses may be biased, limiting accuracy and obscuring true relationships. The study’s single-region scope restricts generalizability, while possible selection bias exists as individuals with harassment experiences may have been more likely to participate, though anonymity aimed to reduce this. Future longitudinal and multi-center studies, including marginalized groups, are needed to clarify causal pathways and develop targeted interventions.
Bullying in Indian medical education is alarmingly common, affecting wellbeing and academic success. Renewed attention to policy implementation, reporting infrastructure, and cultural change is necessary to promote safety and dignity in medical institutions.
1. Neglect as an undefined and overlooked aspect of medical student mistreatment: A systematic review of the literature. Medical Teacher. 2023; 45 (12). Available from: https://doi.org/10.1080/0142159x.2023.2218982
2. Beyond mistreatment: Learner neglect in the clinical teaching environment. Medical Teacher. 2019; 41 (8). Available from: https://doi.org/10.1080/0142159x.2019.1602254
3. Medical student mistreatment: understanding ‘public humiliation’. Medical Education Online. 2019; 24 (1). Available from: https://doi.org/10.1080/10872981.2019.1615367
4. Medical Student Mistreatment. JAMA. 2016; 316 (21). Available from: https://doi.org/10.1001/jama.2016.17752
5. Bullying in the Education Workspace in India. international journal of engineering technology and management sciences. 2023; 7 (3). Available from: https://doi.org/10.46647/ijetms.2023.v07i03.113
6. Postgraduates′ Perceptions of Preparedness for Work as a Doctor and Making Future Career Decisions: Support for Rural, Non-traditional Medical Schools. Education for Health. 2010; 23 (2). Available from: https://doi.org/10.4103/1357-6283.101489
7. The Prevalence of Medical Student Mistreatment and Its Association With Burnout. Academic Medicine. 2014; 89 (5). Available from: https://doi.org/10.1097/acm.0000000000000204
8. Addressing unprofessional behaviors in the clinical learning environment: lessons from a multi-year virtual, intergenerational, interdisciplinary workshop. Medical Education Online. 2024; 29 (1). Available from: https://doi.org/10.1080/10872981.2024.2316491
9. Assessment of the Prevalence of Medical Student Mistreatment by Sex, Race/Ethnicity, and Sexual Orientation. JAMA Internal Medicine. 2020; 180 (5). Available from: https://doi.org/10.1001/jamainternmed.2020.0030
10. Resilience and self-compassion among persons with depressive disorders: Prerequisite for a positive mental health approach. Journal of Family Medicine and Primary Care. 2023; 12 (8). Available from: https://doi.org/10.4103/jfmpc.jfmpc_2270_22
11. Psychological autopsy of 101 suicide cases from northwest region of India. Indian Journal of Psychiatry. 2008; 50 (1). Available from: https://doi.org/10.4103/0019-5545.39757
12. Chakraborty C, Chatterjee C, Chaudhuri A. Ragging in medical colleges of West Bengal - A student's perspective. IJCMR. 2022:9(3).
13. Second-year medical students’ motivational beliefs, emotions, and achievement. Medical Education. 2010; 44 (12). Available from: https://doi.org/10.1111/j.1365-2923.2010.03712.x
14. Medical student abuse during clinical clerkships in Japan. Journal of General Internal Medicine. 2006; 21 (3). Available from: https://doi.org/10.1111/j.1525-1497.2006.00320.x
15. Unethical and unprofessional conduct observed by residents during their first year of training. Academic Medicine. 1998; 73 (11). Available from: https://doi.org/10.1097/00001888-199811000-00019
16. A Pilot Study of Medical Student 'Abuse' Student Perceptions of Mistreatment and Misconduct in Medical School. JAMA. 1990; 263 (4). Available from: https://doi.org/10.1001/jama.1990.03440040072031
17. Sexual Harassment Experiences of Female Graduates of Nigerian Tertiary Institutions. International Quarterly of Community Health Education. 2010; 30 (4). Available from: https://doi.org/10.2190/iq.30.4.e
18. Experiences of belittlement and harassment and their correlates among medical students in the United States: longitudinal survey. BMJ. 2006; 333 (7570). Available from: https://doi.org/10.1136/bmj.38924.722037.7c
19. Medical students learning intimate examinations without valid consent: a multicentre study. Medical Education. 2011; 45 (3). Available from: https://doi.org/10.1111/j.1365-2923.2010.03911.x
20. Aggression in the Workplace: A Social-Psychological Perspective.. Counterproductive work behavior: Investigations of actors and targets.. 2005; Available from: https://doi.org/10.1037/10893-001
21. Self-harm Among Hispanic Adolescents: Investigating the Role of Culture-Related Stressors. Journal of Adolescent Health. 2014; 55 (5). Available from: https://doi.org/10.1016/j.jadohealth.2014.05.017
22. Bullying among healthcare professionals and students: Prevalence and recommendations. Journal of Taibah University Medical Sciences. 2023; 18 (5). Available from: https://doi.org/10.1016/j.jtumed.2023.02.011
23. The State of Academic Bullying Among Medical Students in Tanzania: Prevalence, Forms and Associated Factors. A Cross-Sectional Study. Journal of Medical Education and Curricular Development. 2024; 11 Available from: https://doi.org/10.1177/23821205241301928
24. Workplace bullying as an organizational problem: Spotlight on people management practices.. Journal of Occupational Health Psychology. 2022; 27 (6). Available from: https://doi.org/10.1037/ocp0000335
25. Workplace bullying as an organisational issue: Aligning climate and leadership. Work & Stress. 2022; 36 (2). Available from: https://doi.org/10.1080/02678373.2021.1969479
26. Cyberbullying across the Lifespan of Education: Issues and Interventions from School to University. International Journal of Environmental Research and Public Health. 2019; 16 (7). Available from: https://doi.org/10.3390/ijerph16071217
27. Nursing Intervention for Preventing Cyberbullying and Reducing Its Negative Impact on Students: A Scoping Review. Journal of Multidisciplinary Healthcare. 2023; 16 Available from: https://doi.org/10.2147/jmdh.s400779
28. Cyberbullying and mental health: past, present and future. Frontiers in Psychology. 2024; 14 Available from: https://doi.org/10.3389/fpsyg.2023.1279234
Subscribe now for latest articles and news.