Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2017.v03i02.006
Year: 2017, Volume: 3, Issue: 2, Pages: 23-26
Case Report
Archana Randale1, Sanjay Parate2, Saroj Meshram1, Shilpa Tathe1
1Assistant Professor, Department of Pathology, Government Medical College & Superspeciality Hospital, Nagpur, Maharashtra, India,
2Professor and Head, Department of Pathology, Government Medical College & Superspeciality Hospital, Nagpur, Maharashtra, India
Address for correspondence:
Dr. Archana Randale, 301, Siddesh Pratiksha, 29 Ganesh Colony, Ring Road, Pratap Nagar, Nagpur - 440 022, Maharashtra, India. Phone: +91-9860130404. E-mail: [email protected]
Cystic adenomatoid pulmonary malformation (CAPM) is a congenital abnormality of lung which is rare in adults. Here, we report a case of 46-year-old female presented with dyspnea on exertion. Chest radiograph and computed tomography scan showed a single cyst in the posterior segment of right upper lobe in parahilar region with radiological diagnosis of bronchogenic cyst. However, the intrapulmonary location and the absence of cartilage in the cyst wall with multiple adjacent microscopic cysts were conclusive findings of Type I CAPM. Surgical resection is the treatment of choice to prevent future infections such as aspergillosis and potential risk of malignant transformation.
KEY WORDS:Adult, bronchogenic cyst, cystic adenomatoid pulmonary malformation.
Cystic adenomatoid pulmonary malformation (CAPM) is considered as developmental hamartomaous lesion characterized by bronchiolar maturation disturbance.[1] Occurrence in adult is very rare and the pathogenesis is still unknown.[1,2] Disease may remain asymptomatic presenting as incidental finding or can have varied clinical presentation as repeated infections, hemoptysis to lung carcinoma.[1,3]
Here, we report a case of Type I CAPM presenting as expansile cystic mass in upper pulmonary lobe in 46-year-old female patient.
A 46-year-old female patient was admitted with a history of dyspnea on exertion along with an episode of hemoptysis a month prior. There was no history of fever, cough, or weight loss. On examination, there was decreased air entry in right midzone. Rest of the general and systemic examination were normal.
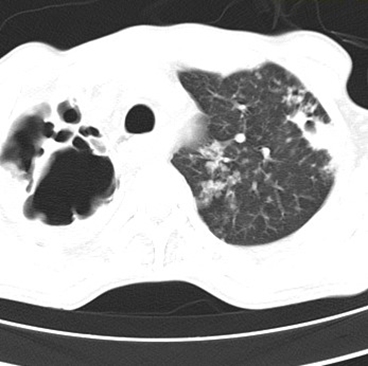
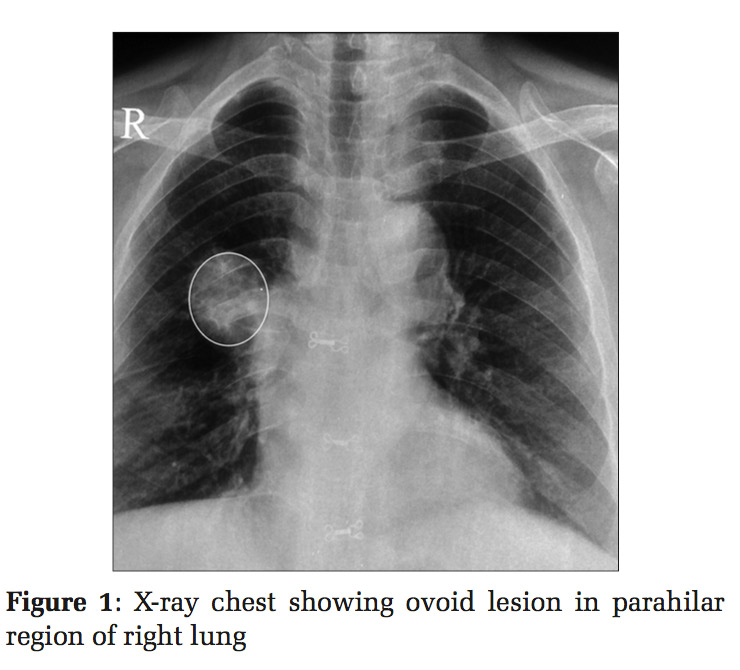
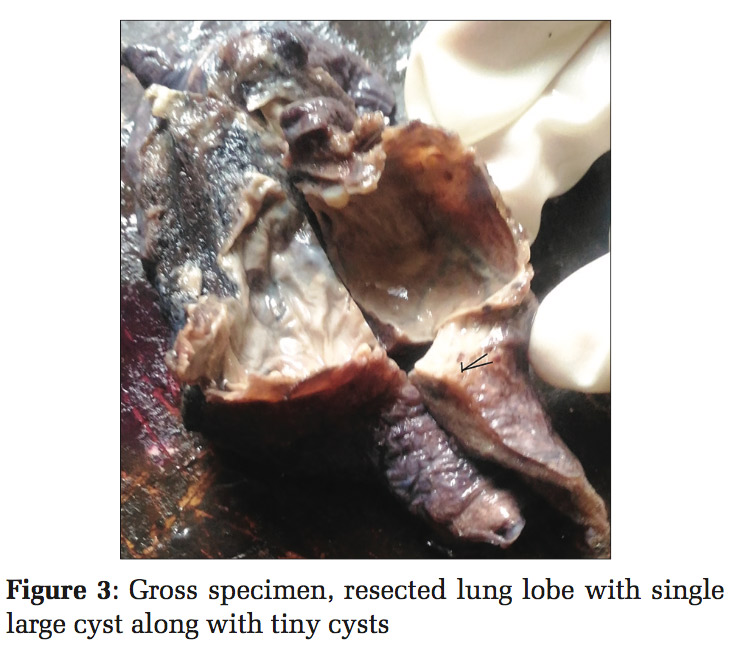
Chest radiograph revealed well-defined ovoid lesion in right parahilar region [Figure1]. Subsequent computed tomography (CT) thorax showed a round well-defined homogenous non enhancing lesion in the parahilar region of posterior segment of right upper lobe measuring 3.9×3.9 cm with no wall calcification [Figure 2]. Both radiological investigation suggested diagnostic possibility of an intrapulmonary bronchogenic cyst.
Other investigations such as bronchioloalveolar lavage and post-bronchoscopic sputum examination for acid-fast bacilli were negative.
CT-guided fine-needle aspiration cytology was done from lesion does not revealed any atypical cells.
Based on this clinical and investigation data, patient was subjected to surgical resection of the affected lung lobe.
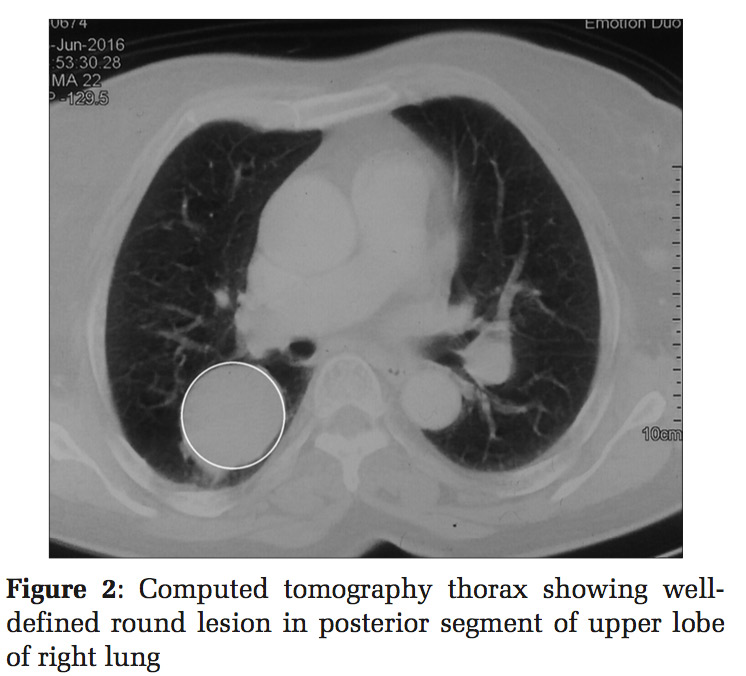
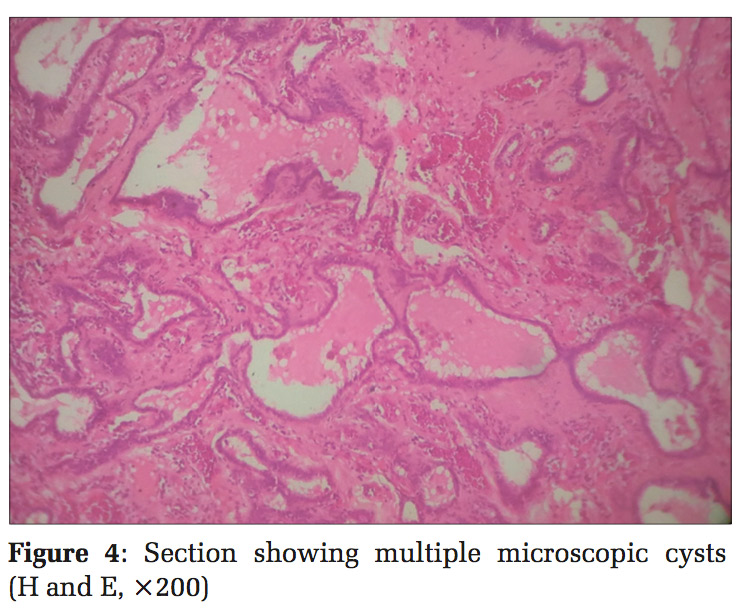
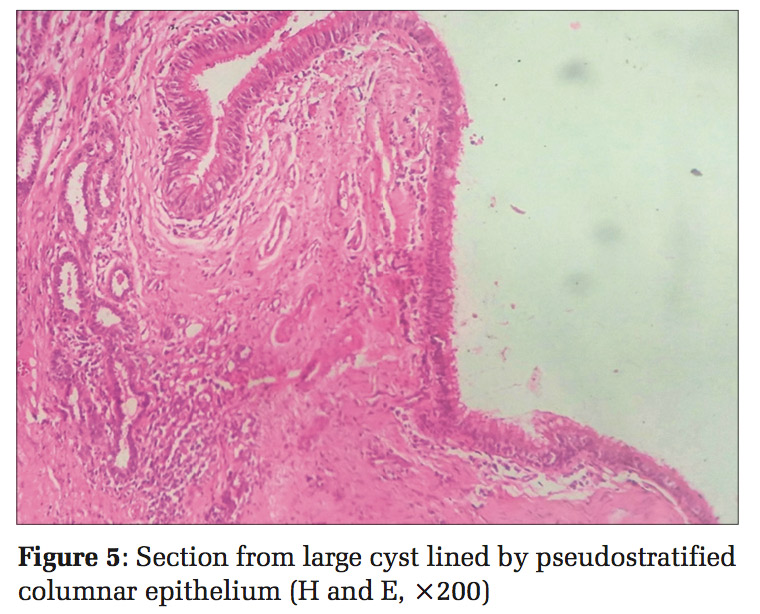
We received a single resected lobe of the lung measuring 8×6×5 cm with large cystic cavity already cut open measuring 4 cm in diameter. Inner side of cyst wall was smooth. 2-3 tiny cysts adjacent to larger cyst also noted [Figure 3]. Microscopic examination of the sections from the larger cyst wall showed lining by pseudostratified ciliated columnar epithelium. Whereas multiple microscopic cystic spaces were seen lined by cuboidal to columnar epithelium. Smaller cysts were filled in by pink proteinecious material. There was absence of coal pigment in cystic areas along with cartilage, smooth muscle, and mucous glands. There was no evidence of granuloma formation or any other specific pathology in the cyst wall orsurroundinglungtissue[Figures4and5].The histomorphological diagnosis of Type I CAPM was given. The patient had uneventful post-operative period.
Cystic adenomatoid malformation is a rare cystic lung lesion formed as a result of anomalous development of airways in fetus with incidence of 1 in 25000-35000 pregnancies.[2,4,5] Majority are recognized in neonates and infants with respiratory distress and very few present later in adult life.[4]
The classical histological finding of CAPM is normal pulmonary alveoli are replaced by cyst which composed of adenomatoid hyperplastic bronchioles.[6] Three morphological varieties have been described depending on the size and number of the cyst.[6,7]
Our case met with the diagnostic criteria of Type I CAPM showing one cyst larger than 3 cm diameter with 2-3 tiny cysts in its periphery. Larger cyst was lined by pseudostratified columnar epithelium along with multiple microscopic adenomatoid cysts.[2,7,8] Our patient was a female aging 46 years. According to de Sousa et al.[1] CAPM in adults occur with the mean age of 53.4 years with more of female frequency, mirroring our findings.
A single large cyst in an adult has to be differentiated from more commonly occurring pulmonary lesions such as intralobar sequestration, bronchogenic cyst, lung abscess, and bronchiectasis.[2]
Radiological diagnosis offered in our case was bronchogenic cyst. However, bronchogenic cyst has mediastinal location predominantly and only one-fourth cases of bronchogenic cyst are intrapulmonary.[9] They are usually unilocular and contain bronchial cartilage, smooth, and mucosal glands histologically which were lacking in our case. Bronchogenic cyst usually do not communicate with alveoli while adenomatoid malformation do.[1]
Intralobar sequestration is diagnosed during operative procedure, identified by the presence of anomalous blood supply to the affected lobe. Destruction of lung parenchyma along with the presence of inflammatory response and fibrosis in the wall is the feature of lung abscess. Post-infectious bronchiectasis usually occurs bilaterally and show honeycombing of lung with pleural changes which are lacking in CAPM. Microscopically bronchiectasis show the presence of cartilage in the wall, marked suppurative inflammation and sqaumous metaplaisa of lining epithelium.[2,10]
Due to risk of malignant transformation and recurrent respiratory infections including aspergillosis, lobectomy is the treatment of choice.[1,4,11]
CAPM in adults is rare form of cystic pulmonary lesions with uncertain radiological findings. Hence, surgical resection with histopathological examination is must confirm the nature of the lesion as well as to prevent infection and the potential risk of malignant transformation.
Subscribe now for latest articles and news.