Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.412
Year: 2026, Volume: 12, Issue: 2, Pages: 223-226
Case Report
Matsyangna Singh 1, Rajeev Kumar Ranjan 2, Anjali Bharti 1, Shalini Singh 3
1Senior Resident, Department of Radio-diagnosis, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand, India.
2Associate Professor, Department of Radio-diagnosis, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand, India.
3PG II, Department of Radio-diagnosis, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand, India.
Address for correspondence: Matsyangna Singh, Senior Resident, Department of Radio-diagnosis, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand, India.
E-mail: [email protected]
Received Date:18 December 2025, Accepted Date:25 April 2026, Published Date:15 June 2026
This report describes a rare case of incidentally detected intralobar pulmonary sequestration in an elderly male, accurately characterized using contrast-enhanced multidetector CT (CE-MDCT), including 3D-MPR and MIP imaging techniques. A 70-year-old male presented with generalised weakness and intermittent shortness of breath on exertion and a history of pulmonary TB four years ago (ATT defaulter). The chest radiograph revealed chronic fibrotic or post-infectious sequelae with volume loss in the left hemithorax. A homogeneous opacity was seen in the right lower zone, obscuring the right hemidiaphragm medially. Further CECT Chest demonstrated a well-defined soft tissue density lesion measuring approximately 9.9x7x3.9 cm in the anterior basal segment of the right lower lobe with no bronchial connection. The lesion showed a systemic arterial supply, with the feeding artery originating from the right renal artery and venous drainage into the right superior pulmonary vein. These findings were better appreciated on the maximum intensity projection (MIP) images, facilitating an accurate characterization of the lesion. Thus, a definitive diagnosis of intralobar pulmonary sequestration was established. The patient remained clinically stable and exhibited no significant symptoms attributable to the sequestration; thus, surgical management was deferred, and he was discharged with a plan for scheduled follow-up. CE-MDCT allows concurrent assessment of anomalous vessels and lung parenchymal lesions, making it a highly effective technique with a strong potential to become the diagnostic method of choice for pulmonary sequestration.
Pryce first described the term pulmonary sequestration (1946)[1], classifying it into two types [Table. 1][1, 2]. It is an uncommon congenital lung malformation which has a non-functioning lung segment that is devoid of normal trachea-bronchial communication and receives its arterial supply from a separate abnormal systemic artery. Clinically, intralobar sequestration most often presents in childhood or early adulthood (typically before 20 years of age)[1, 2] with recurrent pneumonia involving the same pulmonary segment. Additional presentations include fever, persistent productive cough, hemoptysis, dyspnoea and chest or back discomfort.
| Feature | Intralobar Sequestration (ILS) | Extralobar Sequestration (ELS) |
|---|---|---|
| Incidence | More common | Less common |
| Pleural covering | Pleura of the adjacent normal lung is shared | Has its own separate pleural covering |
| Arterial supply | Aberrant systemic artery (commonly from thoracic or abdominal aorta) | Aberrant systemic artery (commonly from abdominal aorta) |
| Venous drainage | Into pulmonary veins | Into systemic veins (azygos, hemiazygos, IVC) |
| Age at diagnosis | Usually childhood or early adulthood (<20 years) | Often in infancy |
| Common location | Posterior basal segment of lower lobes (usually left) | Between left lower lobe and diaphragm; may occur subdiaphragmatically |
| Associated anomalies | Rare | Common |
A minority of patients are asymptomatic, and the anomaly is identified incidentally. However, incidental detection in the elderly is exceedingly uncommon and may pose a significant diagnostic challenge[2-4]. Surgical excision is the treatment of choice, with generally favourable outcomes[3]. We report a rare case of an incidentally discovered intralobar pulmonary sequestration in an elderly male.
A 70-year-old male presented with complaints of generalised weakness and intermittent exertional dyspnoea for past four years. There was no associated fever or cough. He suffered pulmonary tuberculosis four years ago but was a treatment defaulter (left ATT after one month). Routine laboratory investigations did not show any significant abnormality except anaemia. There was no history of any co-morbidity, addiction, major surgical illness, hemoptysis, or recurrent chest infections. A chest radiograph was done for further evaluation.
The chest radiograph [Fig. 1] revealed heterogeneous opacification involving the left mid and lower lung zones associated with fibrobronchiectatic changes, irregular architectural distortion and upward deviation of the left hilum. The left hemithorax had features of volume loss, including mediastinal and tracheal shift towards the left, crowding of ribs and elevated left hemidiaphragm. Fibrobronchiectatic changes were noted in the right mid zone. Homogeneous opacity was seen in the right lower zone, obscuring the right hemidiaphragm medially; differential considerations included consolidation or a lung mass.

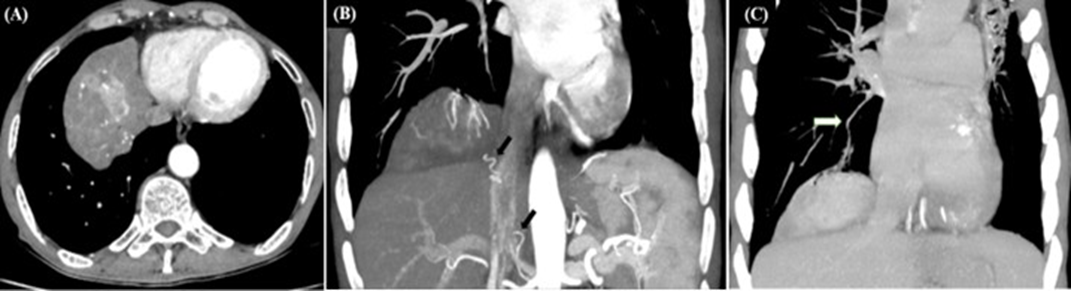

The CECT Chest demonstrated a well-defined heterogeneous soft tissue density lesion measuring 9.9x7x3.9 cm (APxTRxCC) in the anterior basal segment of right lower lobe extending to the diaphragmatic pleural surface ([Fig. 2]A). Few internal calcific foci were seen. The lesion showed no significant post-contrast enhancement, and no bronchial communication was identified. Notably, the lesion showed systemic arterial supply with the feeding artery (2-3 mm in diameter) arising from the right renal artery and coursing superolaterally. The venous drainage was into the right superior pulmonary vein. Also, it demonstrated focal hypervascularity (likely due to systemic perfusion). These vascular features were more clearly delineated on the maximum intensity projection (MIP) images, facilitating accurate characterization of the lesion ([Fig. 2]B, C). Based on the above imaging findings, a diagnosis of intralobar pulmonary sequestration was established. Additional findings included fibrobronchiectatic changes involving bilateral upper and left lower lobes, predominantly affecting the left upper lobe, along with left lung volume loss [Fig. 3], likely sequelae to old infection. As the patient remained clinically stable and exhibited no significant symptoms attributable to the sequestration, surgical management was deferred, and he was discharged with a plan for scheduled follow-up.
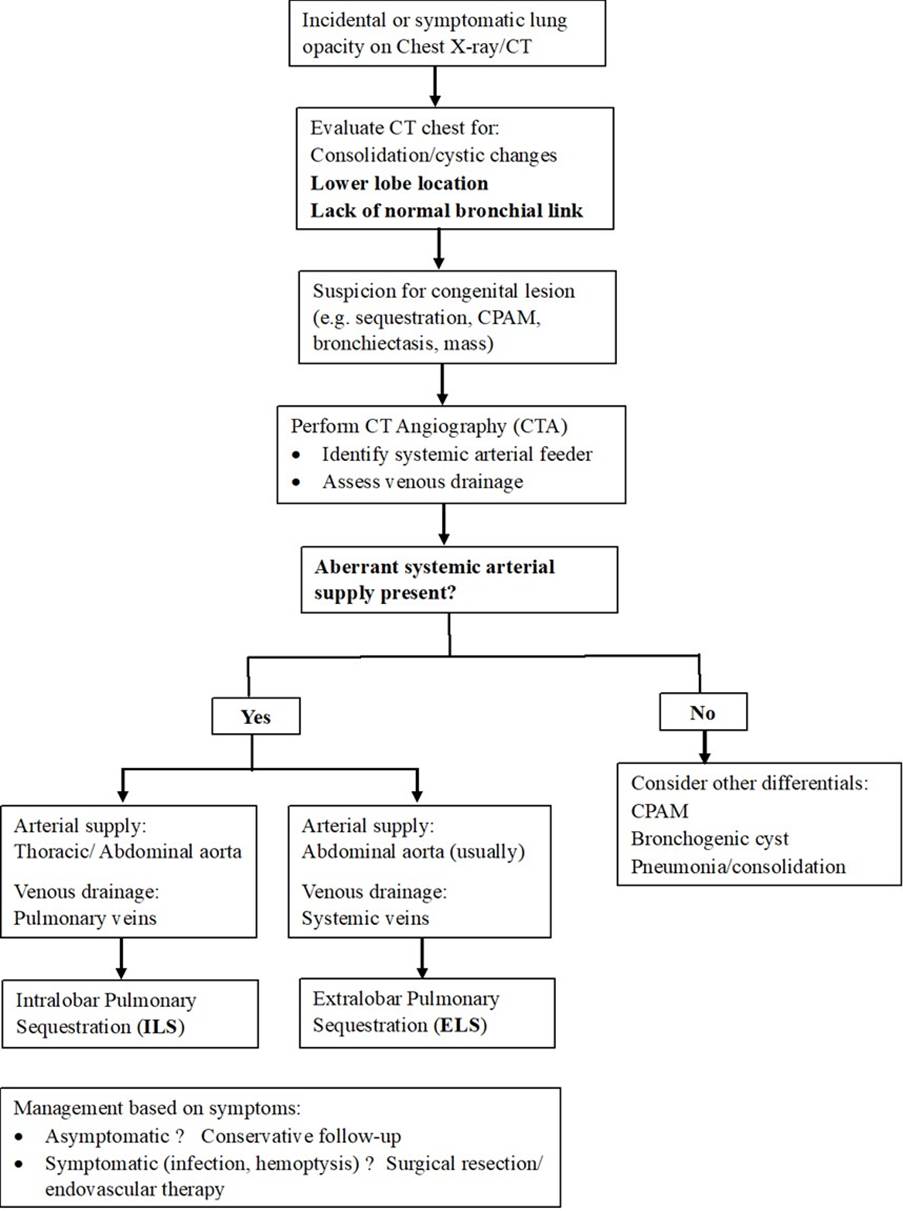
Incidental detection of pulmonary sequestration in the elderly is rare and may pose a significant diagnostic challenge[3]. This case highlights that meticulous evaluation of the characteristic imaging findings of pulmonary sequestration enables confident diagnosis and helps to avoid misinterpretation (see [Fig. 4], Flowchart).
On imaging, pulmonary sequestration usually appears as a lower-lobe consolidation or mass. It can also manifest as focal atelectasis, cyst, bronchiectasis, or a well-defined lesion containing air–fluid levels. The differential diagnoses include persistent pneumonia, congenital pulmonary airway malformation (CPAM), bronchogenic cyst, pulmonary arteriovenous malformation, Scimitar syndrome or lung abscess[3, 4]. Demonstration of a systemic arterial supply is the key diagnostic feature. Lesions are often hypervascular due to systemic perfusion (also noted in this case), and superimposed infection may produce adjacent consolidation or inflammatory neovascularization[3].
Digital subtraction angiography (DSA) was traditionally the preferred modality for demonstrating pulmonary sequestration and its anomalous systemic arterial supply[3, 4]. However, CE-MDCT now offers accurate, non-invasive vascular evaluation[3]. CE-MRI provides a reasonable alternative, but its limited assessment of lung parenchyma and airways, along with higher cost and reduced availability remain important considerations[3]. In our case, CE-MDCT with 3D multiplanar reconstructions (3D-MPR) and maximum intensity projection (MIP) imaging techniques were sufficient for the diagnosis and for defining key anatomic features relevant to surgical planning.
In elderly patients, pulmonary sequestration may remain clinically silent; or it can present with recurrent infections or radiological features that closely mimic pulmonary malignancy. So, the accurate imaging diagnosis is crucial, particularly in this age group. Contrast-enhanced multidetector CT (CE-MDCT) has now emerged as a reliable, non-invasive alternative to the traditional diagnostic modalities, allowing precise delineation of the anomalous vascular supply. Also, it enables concurrent assessment of anomalous vessels and lung parenchymal lesions, making it a highly effective technique with strong potential to become the diagnostic method of choice for pulmonary sequestration.
Conflicts of interest: The authors have no conflicts of interest to disclose.
Funding: None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Acknowledgment: The authors would like to thank Dr Nitish Kumar, Department of Radiodiagnosis, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand, India for facilitating data collection and access to patient.
1. Intralobar sequestration: radiologic-pathologic correlation.. RadioGraphics. 1997; 17 (3). Available from: https://doi.org/10.1148/radiographics.17.3.9153708
2. Webb WR, Higgins CB. Thoracic imaging: pulmonary and cardiovascular radiology. 2nd ed. Philadelphia: Elsevier; 2011.
3. Intralobar pulmonary sequestration in elderly woman: a rare case report with emphasis on imaging findings. Radiology Case Reports. 2016; 11 (3). Available from: https://doi.org/10.1016/j.radcr.2016.05.004
4. Chakraborty RK, Modi P, Sharma S. Pulmonary sequestration. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532314/
Subscribe now for latest articles and news.