Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i2.24.103
Year: 2024, Volume: 10, Issue: 2, Pages: 162-168
Original Article
Sanjeev Kumar Shukla1 , Somesh Mehra1 , Prabhat Pant2 , Shahzad Ahmad3 , Govind Singh4
1Multidisciplinary Research Unit, Government Medical College, Haldwani, Nainital, Uttarakhand, India,
2Department of Pathology, Government Medical College, Haldwani, Nainital, Uttarakhand, India,
3Department of ENT, Government Medical College, Haldwani, Nainital, Uttarakhand, India,
4Department of Biochemistry, The Autonomous State Medical College Society (ASMCS), Firozabad, Uttar Pradesh, 283203, India
Address for correspondence:
Sanjeev Kumar Shukla, Multidisciplinary Research Unit, Government Medical College, Haldwani, Nainital, Uttarakhand, India.
E-mail: [email protected]
Received Date:28 March 2024, Accepted Date:30 May 2024, Published Date:17 June 2024
Background: Graves’ disease (GD) is an autoimmune disorder with genetic predisposition and CD40 plays a pathogenic role in various autoimmune diseases. A single nucleotide polymorphism (SNP) at position –1 of the Kozak sequence of the 5 untranslated region of CD40 gene of exon 1 has been reported to be associated with the development of GD. Objective: The aim of the present study was to investigate whether CD40 gene polymorphism confers susceptibility to GD in Kumaon region. CD40 gene polymorphisms were studied in GD patients (n=50) and healthy control subjects without anti-thyroid autoantibodies or a family history of autoimmune disorders (n=50). Material and Method: CD40 gene polymorphisms were studied in fifty GD patients and fifty healthy control subjects. All samples collected from STG Hospital, Haldwani, Nainital. A C/T polymorphism at position –1 of the CD40 gene was measured using the polymerase chain reaction restriction fragment length polymorphism. Results: There was no significant difference in allele or genotype frequency of the CD40 SNP between GD and control subjects. There was a significant decrease in the TT genotype frequency in the GD patients, who developed GD after 40 years old, then those under 40 years of age. These data suggest that the SNP of CD40 gene is associated with susceptibility to later onset of GD. Conclusion : The CD40 gene was a new susceptibility gene for GD within certain families because it was both linked and associated with GD.
Keywords: Autoimmune Diseases, Pathogenesis, Diagnosis, Therapy
Graves' disease (GD) is the most common organ-specific autoimmune disorder with 0.5% of the population affected and patients are predominantly 40-60 years old 1. Although the etiology remains to be elucidated, GD is hypothesized to be the result of a complex interaction between genetic and environmental factors 2. The two genetic loci have a substantial influence on GD susceptibility, namely the major histocompatibility complex (MHC) and the cytotoxic T lymphocyte antigen-4 (CTLA4) gene, which are located on chromosomes 6p21 and 2q33, respectively 3. These loci may account for up to half of the inherited susceptibility to GD and seven putative GD loci have been identified by linkage studies using anonymous (short tandem repeat/microsatellite) genetic markers, with evidence suggestive of linkage to GD on chromosomes 5q31–q33, 8q24, 14q31, 18q21, 20q11, Xp11 and Xq21 4. These genetic linkages, there has been little advance in knowledge about the pathogenesis of GD, with the exceptions of CTLA4 and possibly thyroglobulin (8q24) 5. The actual susceptibility genes within these genomic intervals have yet to be determined. One region of linkage to microsatellite genetic markers is located on chromosome 20q11 and has been termed the GD2 locus. The GD locus encompasses a broad chromosomal region of approximately 20 cM, however, Tomer and colleagues have used a recombination mapping approach to narrow down the region likely to contain the susceptibility gene 6, 7.
CD40 is a member of the tumor necrosis factor receptor superfamily member 5, gene symbol TNFRSF5), expressed predominantly on B lymphocytes, monocytes, antigen presenting cells and thyrocytes 8. Interaction of CD40 with its ligand induces a polarized release of cytokines from the activated helper T cell, which locally promotes differentiation of T cells into TH2 cells 9. The deviation of immune response to the TH2 pathway by CD40 might result in driving thyroid autoimmunity in the direction of GD, and could influence the production of stimulating thyrotropin receptor antibodies (TSHRAbs) in B cells from Graves’ patients. thyroidal CD40 overexpression augmented the production of thyroid-specific autoantibodies, leading to more severe experimental autoimmune GD 10. Therefore, CD40 may play an important role in the pathogenesis of GD.
CD40 is expressed on the surface of B lymphocytes and other antigen presenting cells and has a key role in determining T-cell responses to antigen presentation and B-cell immunoglobulin isotype switching 11. CD40 knockout mice have been shown to have decreased numbers of regulatory T cells and increased T-cell autoreactivity 12 suggesting a potential role for CD40 in autoimmunity. The X-linked hyper-immunoglobulin M (IgM) syndrome, in which the CD40-ligand is defective, is characterized by immunodeficiency and an increased risk of autoimmune diseases 13.
Thyroidal CD40 overexpression augmented the production of thyroid-specific autoantibodies, leading to more severe experimental autoimmune GD. Therefore, CD40 may play an important role in the pathogenesis of GD. Human CD40 gene, a functional C/T polymorphism (rs1883832) in the Kozak sequence of the 5' UTR has received much attention 14.
GD patients with a polymorphism of the Kozak consensus sequence in the 5-untranslated region (5UTR) of the CD40 gene may be associated with GD 15. GD appears with Korean subjects to confirm the association of this CD40 5UTR polymorphism with GD, but not with Hashimoto’s thyroiditis 16. This study also investigated the association between gene polymorphism SNP study between patients and control group compare with clinical and laboratory data association with CD40 SNP could be related to the development of GD in Kumaon population.
Case control study was carried out on fifty individuals, divided into fifty GD patients
The normal control group contained fifty (seventeen male and thirty-three female), apparently healthy individuals. They were selected randomly from relatives of patients and other volunteers. They were free from symptoms and signs of family history of thyroid disease and no goiter on examination; they had normal thyroid functions and were negative for thyroid autoantibodies and no any chronic diseases such as DM, cardiac diseases, heart diseases, hypertension, renal diseases or others. All cases completed detailed included the essential information, i.e., age, sex, family history, medicine history, and any other relevant information.
The inclusion criteria for the healthy control group were as follows: (1) There was no abnormality in medical history, physical examination, blood glucose examination, blood pressure, blood lipids and other biochemical tests through inquiry. (2) The subjects and other immediate family members over three generations had no autoimmune diseases including GD
It contained fifty patients with GD (Eleven male and thirty-nine female), patients were selected and diagnosed from by specialist doctor team in tertiary care referral hospital, ENT Out Patient Department in Dr. Susheela Tiwari Government Hospital, Haldwani, Nainital, Uttarakhand. The GD was diagnosed by: (1) documented clinical and biochemical hyperthyroidism requiring treatment, (2) a diffuse goiter, (3) presence of TSH-receptor antibodies. For all subjects, phenotype was determined with the clinician blinded to the individual’s genotype.
Blood samples were collected, from the ante median cubital vein of the subjects using disposable plastic syringes with all aseptic precautions. Blood was transferred immediately in to a dry clean plastic test tube with a gentle push to avoid hemolysis. Blood was collected in EDTA vial (Levram Lifesciences Silvassa, India) from both control group and infectious group for molecular research studies. The research was done in the Multidisciplinary Research Unit (DHR-ICMR, New Delhi), Government Medical College, Haldwani, Nainital, Uttarakhand, India
Genomic DNA was isolated from human blood samples by using genomic DNA extraction kit (GeneJET Genomic DNA Purification Kit, Thermo Fisher Scientific, USA) as per the manufacturer’s instructions using centrifuged (Eppendorf 5424R, Germany). After extraction, DNA samples (working) was stored at 4°C for 7 days before spectrophotometric (analysis and then stored in a freezer at −20°C (Vestfrost, Denmark). DNA concentration and purity were measured by ultraviolet (UV) spectrophotometry using an Eppendorf Bio spectrophotometer (Eppendorf, Hamburg, Germany) using 1 µL of each sample. The spectra were recorded wavelength range of 220–830 nm.
DNA was analyzed by agarose gel electrophoresis (Bio-Rad Mini Gel Electrophoresis Unit, USA) using 0.8% agarose gel (Ameresco USA). Electrophoresis was performed using 10X TBE Buffer (Tris-borate-EDTA) (Thermo Scientific, USA) buffer containing 1 μg/ml of Ethidium Bromide (EtBr) (VWR Amresco Life Science, USA) and a constant voltage of 100 V for 50 min using PowerPac Universal (Bio-Rad Laboratories, USA). The DNA bands were visualized and images were acquired using Gel Doc XR+ Imaging system (Bio-Rad Laboratories, USA).
Oligonucleotide primers were synthesized (Eurofins Genomics India Pvt. Ltd., Kerala, India), CD40 gene polymorphism 17 Polymerase Chain Reaction (PCR) to amplify the polymorphic regions by primer of 5’UTR of CD40 gene Forward, 5'-CCTCTTCCCCGAAGTCTTCC-3 and Reverse, 5'-GAAACTCCTGCGCGGTGAAT-3' size of PCR product 302 bp. The primers for the PCR were as follow by first PCR master mixture was prepared. Reactions were performed in a 25 μl volume containing 12.5 μl of the DreamTaq PCR master mix (2x) Thermo Fisher Scientific, USA (containing DreamTaq DNA polymerase, 2X DreamTaq buffer, 0.4 mM of each dNTP and 4 mM of MgCl2), 0.5 μl each of 10 ng/μl forward and reverse primers (Eurofins Genomics India Pvt Ltd, Kerala, India), 11 μl of nuclease free water (Thermo Fisher Scientific, USA) and 0.5 μl of positive controls or nuclease free water for no template controls (NTC) per 25 μl of reaction mix in 0.2 ml flat cap PCR tubes (Axygen Scientific, USA). The mixture was overlaid with mineral oil and subjected to PCR amplification and PCR conditions for amplification of a 302 bp (Figure 1) fragment of CD40 gene polymorphism, 35 cycles of PCR consisting of denaturing for 30 sec at 95°C, annealing for 30 sec at 55°C, extension for 1 min at 72°C and a final extension for 10 min at 72°C using the program temp control Thermal cycler System (Applied Biosystems ProFlex PCR System, USA).
The PCR products of CD40 gene were digested by 0.1 U of Sty I (Thermo Fisher Scientific, USA) at 37°C for 2.5 hours. Sty I digest the PCR fragment 99 bp from the 3'-end, which serves as a control for assessing whether digestion is complete. It also digests 129 bp from the 5'-end of the fragment when the C nucleotide is present producing a 74 bp fragment. The digested PCR products were electrophoresed on 3% agarose gels to separate the fragments.

The laboratory data were expressed as means ± standard deviation (SD). Statistical analysis was performed using the Statistical Package for the Social Science program (SPSS for Windows, latest Version 10.3). In this study, a two-tailed P-value less than 0.05 was considered significant.
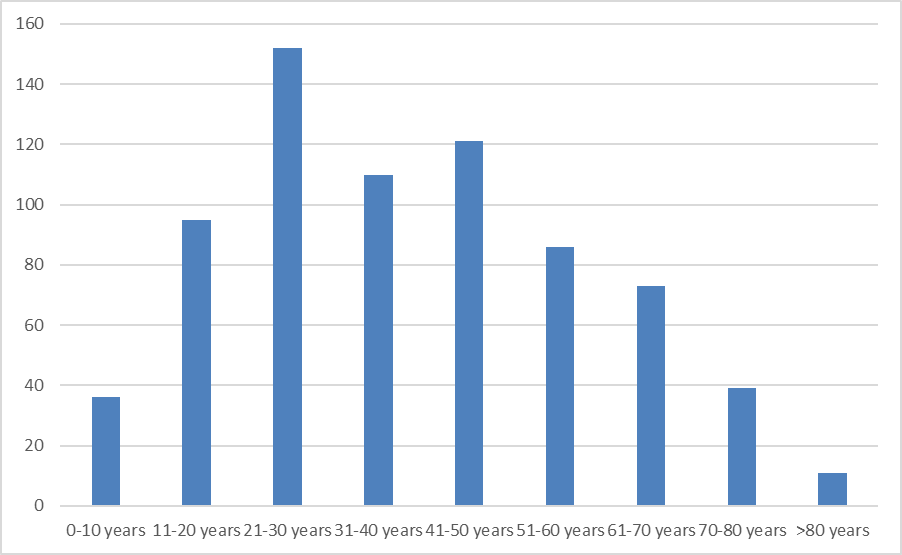
A summary of selected characteristics, including age, gender, thyroid size and family history of Graves’ disease patients (n=50), and healthy individual (n=50) are presented in (Figure 2). The frequency matching variables were compared between the cases and controls. All individuals belonged to the Kumaon population. Graves’ disease patients mean ages (years ± standard deviation) 42.7±10.2 compare with healthy individual (41.2±11.2). However, the mean age of the GD group was slightly higher than that of the controls. Matching of gender was imperfect, the cases had a markedly higher percentage of female (78 %) than the controls (66%), due to GD predominantly affecting females and in GD patient’s male (22%) than the control (34%). The thyroid size of Graves’ disease patients was Normal (10%), First Stage (22%), Second Stage (36%) and Third stage (32%). Family history of graves’ disease patients in this study (60%) and without family history was (40%) graves’ disease patients. The genotype frequencies of Graves’ disease patients CD40 were 74% (CC), 22% (CT), and 4% (TT) and genotype frequencies of healthy individual 56% (CC), 30% (CT) and 14% (TT). The genotype frequencies of Graves’ disease patients the parameter of odds ratios (ORs) and 95% confidence intervals (95% CIs) was 4.11 (0.81-19.59) and the p value < 0.05. The genotype frequencies of Graves’ disease patients of Allele T (27%) and Allele C (73%) and genotype frequencies of healthy individual Allele T (22%) and Allele C (78%). The detailed genotype and allele frequency distribution of CD40 gene polymorphism were shown in Figure 3.


No correlation was obtained between genotype at any SNP and clinical phenotype, including the severity of GD, age at biochemical diagnosis of thyroid dysfunction, presence or absence of goitre on physical examination (defined as palpable or visible thyroid enlargement), biochemical severity of thyroid dysfunction at diagnosis determined from serum concentrations of T3, T4 and presence or absence of TSH and Anti-TPO study (data not shown).
Direct analysis of the CD40 gene as a susceptibility gene, using a newly identified microsatellite, important immunomodulatory gene demonstrated that the CD40 gene region was linked to GD and sequence analysis of the CD40 gene revealed a new SNP at position 21 in the promoter region of CD40 and locus on chromosome 20q11 that was linked with GD 18. Two other immune modulatory genes have also been shown to confer susceptibility to AITD: the HLA genes and the CTLA-4 gene 19. The mechanisms of induction of GD by these genes are uncertain. There is evidence that specific CTLA-4 polymorphisms are associated with exaggerated immune responses 20. Thus predisposing to autoimmunity in general, and that changes in HLA structure may change the binding properties of HLA in such a way that tolerance to certain self-antigens is not achieved 21. This could have been the result of environmental modulating factors, such as the dietary iodine content, it is possible that because several loci are involved in susceptibility to GD. The CD40 TNFR-5 gene is a member of the TNF receptor family, expressed predominantly on B cells and antigen presenting cells (APCs) and CD40 is a major costimulatory molecule that participates in the activation of T cells and induces B-cell differentiation, immunoglobulin production and isotype switching 22. CD40 ligand interactions can switch the immune response to the TH2 pathway and regulate humoral immunity 23. Therefore, CD40 is a likely positional candidate gene for GD. Moreover, in vivo blockade of CD40 suppressed the induction of experimental autoimmune thyroiditis, suggesting that CD40 may play a role in the development of AITD. The low relative risk conferred by the CC genotype of the CD40 promoter SNP, it is unclear whether the C allele is causative. The SNP identified is in the Kozak sequence of the CD40 gene and the Kozak sequence consists of the 6–8 nucleotides before and after the initiation codon and Changes in the Kozak sequence can cause major alterations in the initiation of translation of a gene (ATG) 24. Thus, it seems that the genetic susceptibility to AITD. The involves an interaction between immune regulatory genes and target tissue specific genes, as well as environmental factors. CD40 is an immune regulatory gene, but unlike other immune genes believed to confer susceptibility to autoimmune diseases, it is a gene driving humoral immunity 25. The CD40 gene may predispose to GD in a number of ways, for example: (1) increased expression of CD40 on APCs may amplify low-level autoimmune responses to thyroid antigens; (2) CD40 may be aberrantly expressed on thyroid follicular cells thus enabling HLA expressing thyrocytes to present thyroid autoantigens to T cells and initiate an autoimmune response 26. The SNP identified in the CD40 gene that was associated with GD and therefore it is likely to contribute to the development of GD. The mechanism by which changes in the CD40 genotype induce autoimmunity remains to be elucidated.
The important aspect of these findings is the analysis of the functional consequences of AITD susceptibility genes variants and the search for genotype-phenotype correlations. It is clear that in the near future new susceptibility genes for AITD and the mechanisms through which they contribute to the disease development will be identified. This will enable the rapid identification of those individuals, who are at higher risk for AITD before the clinical symptoms. Hopefully, these new discoveries will also be reflected in improved therapeutic targets and novel treatments in the near future. Gene therapy is a promising treatment option for a number of diseases and is gaining more and more importance regarding treatment of autoimmune disorders, thyroid specific genes, susceptibility genes, environmental factors and immunological synapse genes.
Genetic diagnoses are increasingly reached by next generation sequencing approaches, and diagnostic samples are increasingly studied with transcriptomic and proteomic methods which provide a wealth of information regarding the genetic background of the proband and the molecular pathways involved in the pathogenesis. Therefore, we propose a vision in which the globality of this information is taken advantage of, for the construction of a personalized precision medicine for rare disease patients
The application of molecular biology to the study of AITD has undoubtedly made the significant progress in determining the complex factors that lead to the development of AITD. Future studies on genetic and epigenetic variations will make it possible to quantify the precise effect of specific susceptibility genes and/or epigenetic variation in estimating the heritability. The relationship between susceptibility genes, environmental factors and epigenetic modulation results in breakdown the self-tolerance leading to AITD.
I appreciate the supporting staff of Multidisciplinary Research Unit and who contributed to this research work. I am thankful to ENT Department and supporting staff for given patient’s information and blood samples for this study. I acknowledge to Central lab of Dr. Susheela Tiwari Government Hospital, Haldwani for collection of control samples. I am highly grateful to Department of Health and Research, Ministry of Health & Family Welfare, New Delhi, India for funding of this research and also appreciative to Principal, Government Medical College, Haldwani, Nainital, Uttarakhand for given research place for this work in Multidisciplinary Research Unit laboratory.
I am highly grateful to Department of Health and Research, Ministry of Health & Family Welfare, New Delhi, India for supporting fund.
This study received ethical approval from the GMC Haldwani 9754/GMC
Subscribe now for latest articles and news.