Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.017
Year: 2021, Volume: 7, Issue: 3, Pages: 105-108
Case Report
Jitendra Wadhwani1 , Pradeep Kamboj2 , Kunal Arora3 , Himanshu Bansal3 , Namita Batra4 , Sumedha Vashishth5
1Assistant Professor, Department of Orthopaedics, Pt.B.D.S. PGIMS, Rohtak, Haryana, India,
2Senior Professor, Department of Orthopaedics, Pt.B.D.S. PGIMS, Rohtak, Haryana, India,
3 Junior Resident, Department of Orthopaedics, Pt.B.D.S. PGIMS, Rohtak, Haryana, India,
4 Junior Resident, Department of Obstetrics and Gynecology, Pt.B.D.S. PGIMS, Rohtak, Haryana, India,
5Assistant Professor, Department of Anaesthesiology, Pt.B.D.S. PGIMS, Rohtak, Haryana, India
Address for correspondence:
Jitendra Wadhwani, Assistant Professor, Department of Orthopaedics, Pt.B.D.S. PGIMS, Rohtak, Haryana, India. E-mail: [email protected]
Aim: Management protocol for orthopaedic trauma in term pregnancy. Background: Orthopaedic trauma is a leading cause of maternal mortality with an incidence of 1%. Management of pregnancy as well as fractures in the best possible way is still a grey zone in orthopaedic practice. Bilateral lower limb fracture in third-trimester pregnant patients is rare and poorly discussed in the literature. Case Description: We report a rare case of 35 year old pregnant patient who suffered from bilateral lower limb fractures following a road traffic accident which was managed in two stages, first stage being LTCS (low transverse Caesarean section) due to of fetal distress, and second stage being extramedullary plate fixation for right sided subtrochanteric femur fracture and external fixator application for open left fracture tibia and fibula. Conclusion: Damage Control Orthopaedics must be used along with multi-disciplinary approach. Instead of treating all pathologies in single sitting, planning two staged surgery was the most important factor in the management protocol. Clinical Significance: Our protocol will help lot of clinicians in managing these type of complicated situation where saving both mother's and fetal life is a priority.
Keywords: Pregnancy, Trauma, Fracture, LTCS
Trauma, affecting 7% of all pregnancies, is the leading cause of non-obstetric death in pregnant women, with an overall maternal mortality of 6% to 7%. Orthopaedic trauma constitute total 1% of all these mortalities.[1,2] It has been shown that fetal mortality ranges from 55% to 65% in major trauma cases. [1,2] There are reports in the literature about pregnancy and lactation osteoporosis associated fractures. [3]
We report management of a rare case of 37th gestation week pregnant woman who sustained post-traumatic bilateral lower limb fractures including open tibia and fibula fracture of left side and Subtrochanteric femur fracture of right side as well as anaemia and fetal distress. The management of patient was done as per ethical guidelines of the institutional ethics committee and in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Informed written consent was taken from the patient regarding use of her records for research and publication.
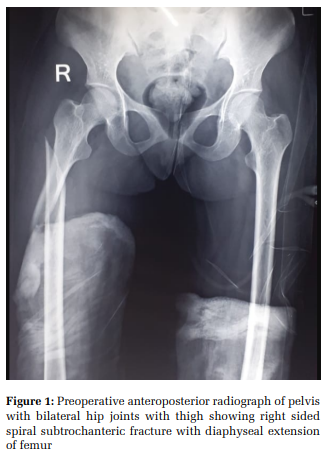
A 35-year Gravida 6 Para 5 woman at 37 weeks gestation with history of previous LTCS (low Transverse Caesarean section) five years ago, presented to the emergency with history of Road Traffic Accident. Her vitals were as follows [BP= 92/68 mm Hg, PR= 126/min, Spo2= 96% on room air, RR= 22/min] at the time of presentation. She was transfused 3 crystalloid (Normal Saline) units, 1 colloid (hydroxyethyl starch) unit and 2 units of whole blood. She was given inj Paracetamol 100ml for pain relief and inj Amoxicillin and potassium clavulanate 1.2gm for controlling infection. She was kept on continuous monitoring until her haemodynamic status stabilised. After 1 hour, the vitals were stabilised [BP= 116/76 mm Hg, PR= 98/min, Spo2= 96% on room air, RR= 18/min]. On general examination, pallor and pitting edema in bilateral lower limbs was present. On local examination, there was pain, swelling and deformity in the right thigh with 5×3 cm lacerated wound on the lateral aspect of left leg and ankle with deformity on the left leg. Both the lower limbs were splinted and kept elevated. Plain film radiography demonstrated a AO 32A1.1 subtrochanteric femur fracture on right side (Figure 1) with AO 42-A3 distal 1/3rd both bone leg open fracture on left side (Figure 2).
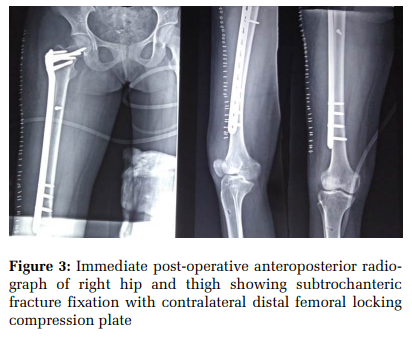
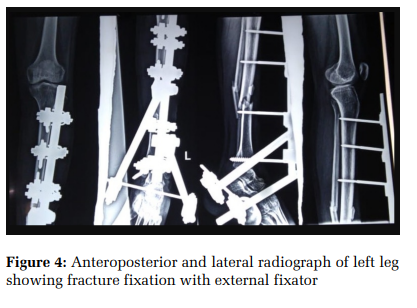
Her haemoglobin was 6.5gm/dl, suggesting severe anaemia. After detailed examination, the obstetric team identified a pregnancy with a singleton, term, fetus in the cephalic presentation. There was no other significant radiological findings. There were no other pregnancy associated complications like gestational diabetes, hypothyroidism etc, or any other pre-existing co-morbidities. The fetal heart tracing was suggestive of fetal distress due to drops in the fetal heart rate to 90 beats per minute. On vaginal examination, the cervix was dilated to 3 centimetres, 30% effaced, with intact membranes and vertex at -1 station. Artificial rupture of membranes was performed with resultant fluid being stained with thick meconium. The woman was immediately transferred to labour room, amnio-infusion was done and continuous cardio-tocographic fetal monitoring was done. During the labour bilateral long leg plaster of Paris splint was used to keep the fractures immobilised. The splintage also helped in examination of the perineal area by keeping the limbs abducted. Simultaneously 100% oxygen through mask was given and ringer lactate was started. In the setting of meconium stained amniotic fluid, prior LTCS and non-reassuring fetal tracing, the patient was taken for emergency repeat LTCS. Considering her haemodynamic status and anaemia, the decision of fractures fixation in same sitting was deferred and second surgery was planned. The baby was delivered by vertex presentation, the APGAR score at 1 minute and 5 minutes was 7/10 and 9/10, respectively, with normal arterial blood gas analysis. The new born did not had any fracture. She was transfused with three units of whole blood during and after the LTCS. Skeletal traction using upper tibial pin on the right side and above knee slab was given on left side after proper wound lavage following LTCS. The patient was planned for orthopaedic surgery 1 week after LTCS. Patient’s haemoglobin was optimised till 10 gm/dl before second surgery. Open reduction and internal fixation with interfragmentary screw and contralateral side. Distal Femoral Locking Compression Plate was done for subtrochanteric femur fracture (Figure 3) and across ankle external fixation for both bone leg fracture was done as a damage control orthopaedic measure (Figure 4). One unit whole blood was transfused after the procedure. The patient remained admitted for 5 days post operatively for wound care of left leg. She was later discharged on lactation safe antibiotics, analgesics and supportive treatment.
Trauma in pregnancy causes risk to life of mother as well as fetus. Damage Control Orthopaedics must be used along with multi-disciplinary approach. Instead of treating all pathologies in single sitting, planning two staged surgery was the most important factor which helped us in the management protocol, as doing single staged surgery could have put patient’s life in danger due to established anaemia, high volume blood loss, prolonged surgical insult.
Our protocol will help lot of clinicians in managing this type of complicated situation where saving both mother and fetal life is a priority.
Conflicts of Interest: None
Source of Funding: None

Subscribe now for latest articles and news.