Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i01.003
Year: 2016, Volume: 2, Issue: 1, Pages: 11-17
Original Article
Kusuma Puttaswamy1, Raja Parthiban2, Shameem Shariff3
1Post-graduate, Department of Pathology, MVJ Medical College & Research Hospital, Bengaluru, Karnataka, India,
2Professor, Department of Pathology, MVJ Medical College & Research Hospital, Bengaluru, Karnataka, India,
3Professor & Head, Department of Pathology, MVJ Medical College & Research Hospital, Bengaluru, Karnataka, India
Address for correspondence: Dr. Raja Parthiban, Department of Pathology, MVJ Medical College & Research Hospital, Hoskote, Bengaluru - 562 114, Karnataka, India. E-mail: [email protected]
Background: Prostatism is an ailment of the geriatric age group leads to a colossal morbidity worldwide. Benign prostatic hyperplasia followed by prostatic adenocarcinoma account for most of the cases of prostatic disease. The concept of geriatrics has not been well-established in India. With increase in life expectancy, better education and increased public awareness the specific diagnosis offered to men with prostatism would increase.
Objectives: The present study was done to determine the spectrum of pathological lesions in transurethral resection prostate (TURP) and needle biopsies from men with prostatism and to analyze the clinical and microscopic anatomy of the lesions encountered.
Materials and Methods: 2 years prospective study from September 2012 to August 2014 in the Department of Pathology, MVJMC and RH, rural Bengaluru on 62 cases of prostate biopsies in men with prostatism. The clinical and laboratory data of each patient were noted from the case records. The clinical and histomorphology findings of the pathological lesions encountered were analyzed.
Results: A total of 62 prostate biopsies were studied over a 2-year period which included TURP (88.70%) and needle biopsy specimens (11.30%). The most common pathology encountered was benign lesions constituting 80.6% (50 cases). Premalignant and malignant lesions constituted 19.4% (12 cases). Both benign and malignant lesions were common in the age group of 51-80 years and had presented clinically with frequency, hesitancy, and dysuria. Gleason’s score of 7 was the most common, seen in 36.3% of cases. Gleason score of 8 and 9 was seen in 27.2% cases each. One case of adenocarcinoma showed neuroendocrine differentiation.
Conclusion: More studies are needed in future to identify environmental and psychosocial factors contributing prostate disease. All prostate carcinomas encountered were of high-grade. Hence, screening of the rural population would have a definitely have a positive impact on the patient outcome.
KEY WORDS:Benign prostatic hyperplasia, prostatic intraepithelial neoplasia, prostatism, prostatic cancer, rural hospital.
IntroductionProstatism is a companion of the geriatric age group and is associated with prostatic disease that leads to significant morbidity worldwide.[1] Benign prostatic hyperplasia (BPH) followed by prostatic adenocarcinoma account for most of the cases of prostatic disease. With prostate carcinoma being the second most common diagnosed cancer in men,[2] a systematic investigation of an adult male with prostatism becomes very important. The concept of geriatric care has not been wellestablished in India and the situation is worse in rural areas. With increase in life expectancy, better education, increased population shift from rural to urban areas, the specific diagnosis offered to men with prostatism would increase.[3] The present study was done to determine the spectrum of pathological lesions in transurethral resection prostate (TURP) and needle core biopsies from men with prostatism in a rural hospital and to analyze the clinical and microscopic anatomy of the lesions encountered without taking into account findings of laboratory results. Materials and MethodsThis 2 years prospective study was done from September 2012 to August 2014 in the Department of Pathology, MVJMC and RH, Bengaluru following approval by the institutional ethics committee on 62 prostate biopsies on men with prostatism. All patients clinically suspected of having prostatism who underwent TURP or Tru-cut needle biopsy, were included for the study. Inadequate biopsies and patients previous diagnosed to have malignancy on histology were excluded. Relevant clinical data of each patient which included the age, presenting symptoms and provisional clinical diagnosis were noted from the case records. Laboratory findings were not analyzed in the present study. Biopsies were fixed in 10% formalin. If the quantity of the received TURP specimen was < 12 cc, the entire tissue was processed. In cases where the volume exceeded 12 cc, additional blocks were prepared for every additional 5 cc of tissue received. In the case of needle biopsies the entire tissue was processed. Paraffin-embedded tissue sections were prepared and 5 μ thick sections were cut and stained routinely with hematoxylin and eosin. Special stains like ZN were performed wherever necessary. The clinical and histomorphology findings of the pathological lesions encountered were analyzed.
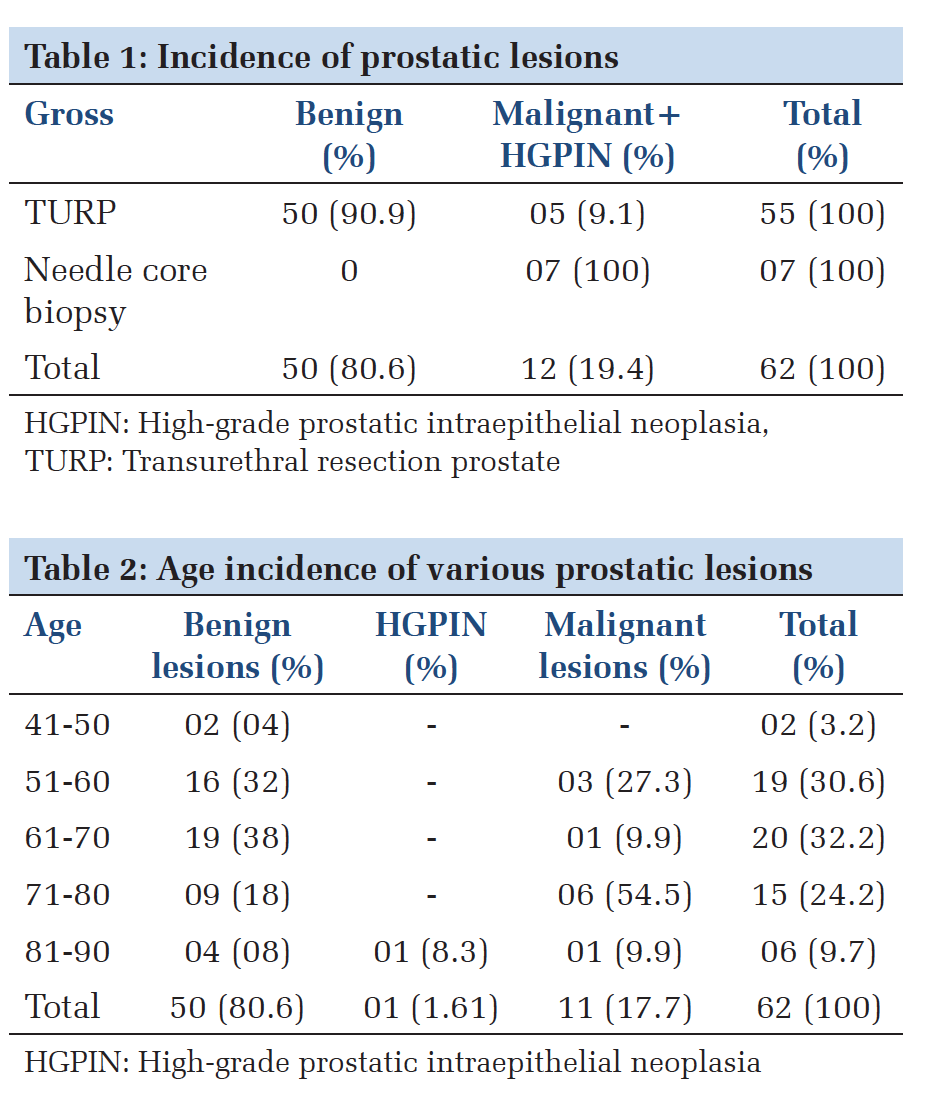
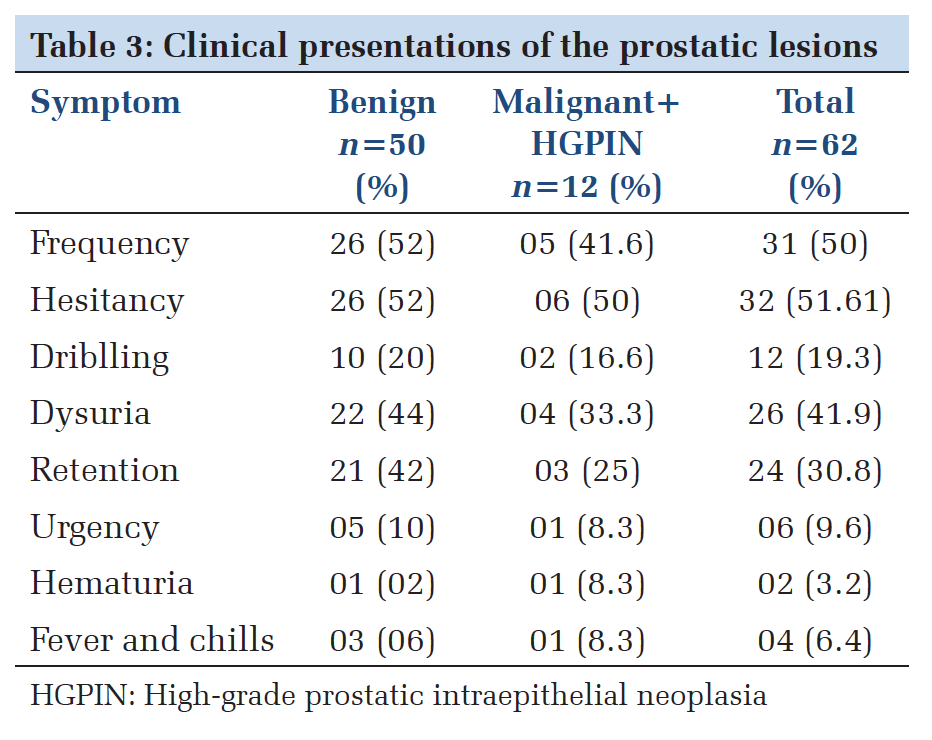
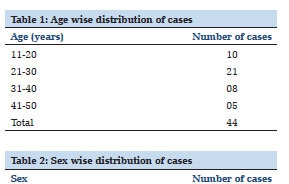
ResultsAbout 62 consecutive biopsies fulfilled the inclusion and exclusion criteria and were included for this study. The majority of the biopsies (55 biopsies, 88.7%) were TURP specimens while needle core biopsies constituted only 7 biopsies (11.3%).In the TURP specimen’s majority were benign lesions, while 9.1% biopsies displayed high -grade prostatic intraepithelial neoplasia (HGPIN) or prostatic malignancy. In the needle biopsies, all 7 cases showed a premalignant or malignant lesion (Table 1). Most of the cases (87%) in the present study were in the range of 50-80 years of age at the time of biopsy for symptomatic obstructive uropathy. The youngest case studied was 50 years while the oldest case was 81 years. Among 50 benign cases, majority belonged to the age group of 51-80 years with a mean of 66.1 years and of the 12 premalignant/malignant cases most were in the 71-80 years age group range with a mean age of 76.8 years. All the malignant cases were found to be high-grade on histology (Table 2). Frequency, hesitancy, dysuria, and retention were the most common clinical symptoms in both benign and malignant lesions. When both lesions were compared, hematuria was seen in 2% of benign lesions and 8.3% of malignant cases. While dysuria and retention were a more common finding among the benign cases accounting for 44% and 42%, respectively (Table 3).
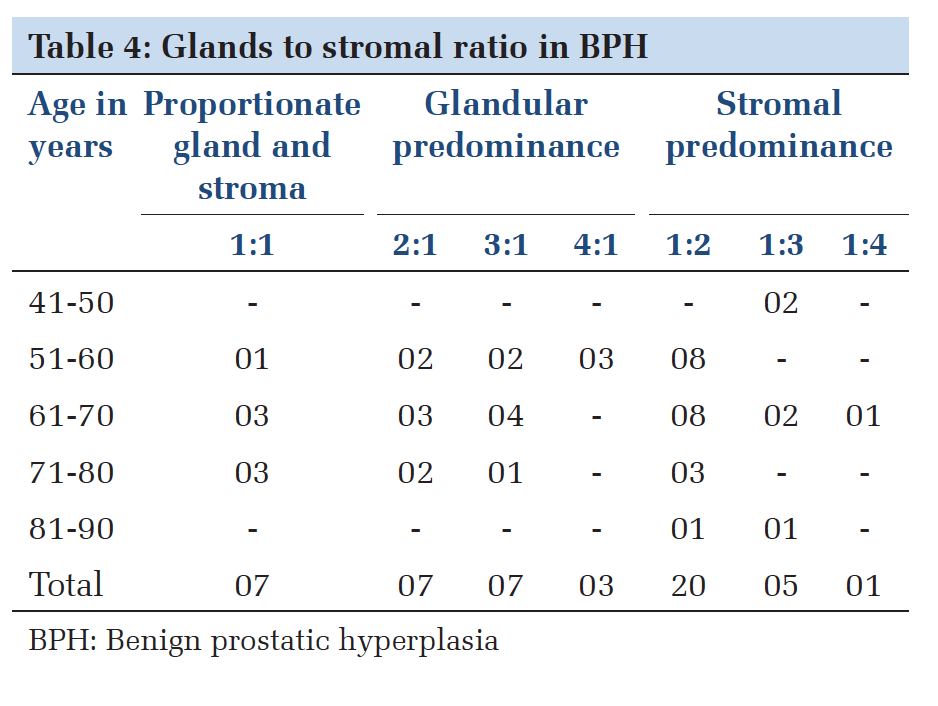
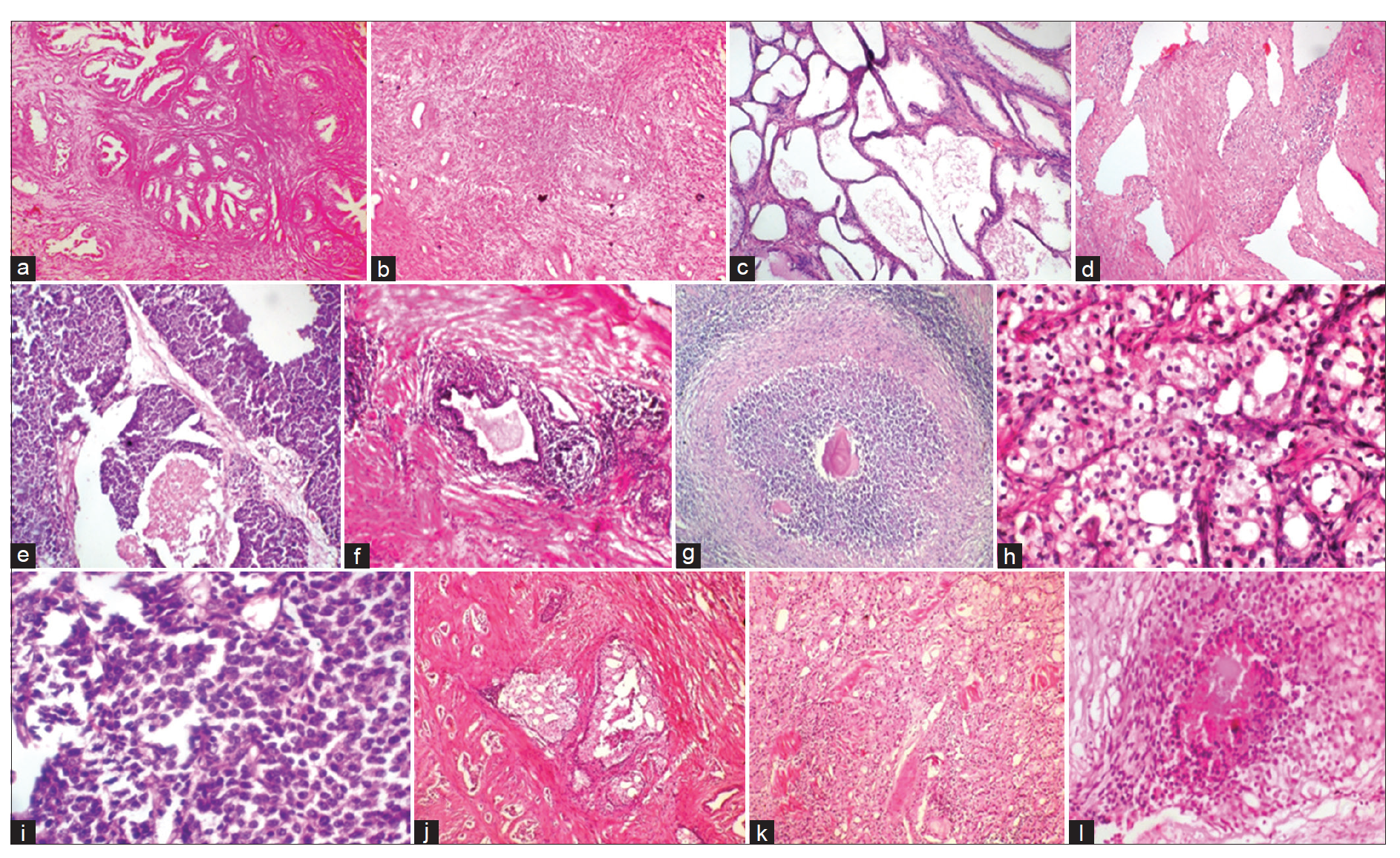
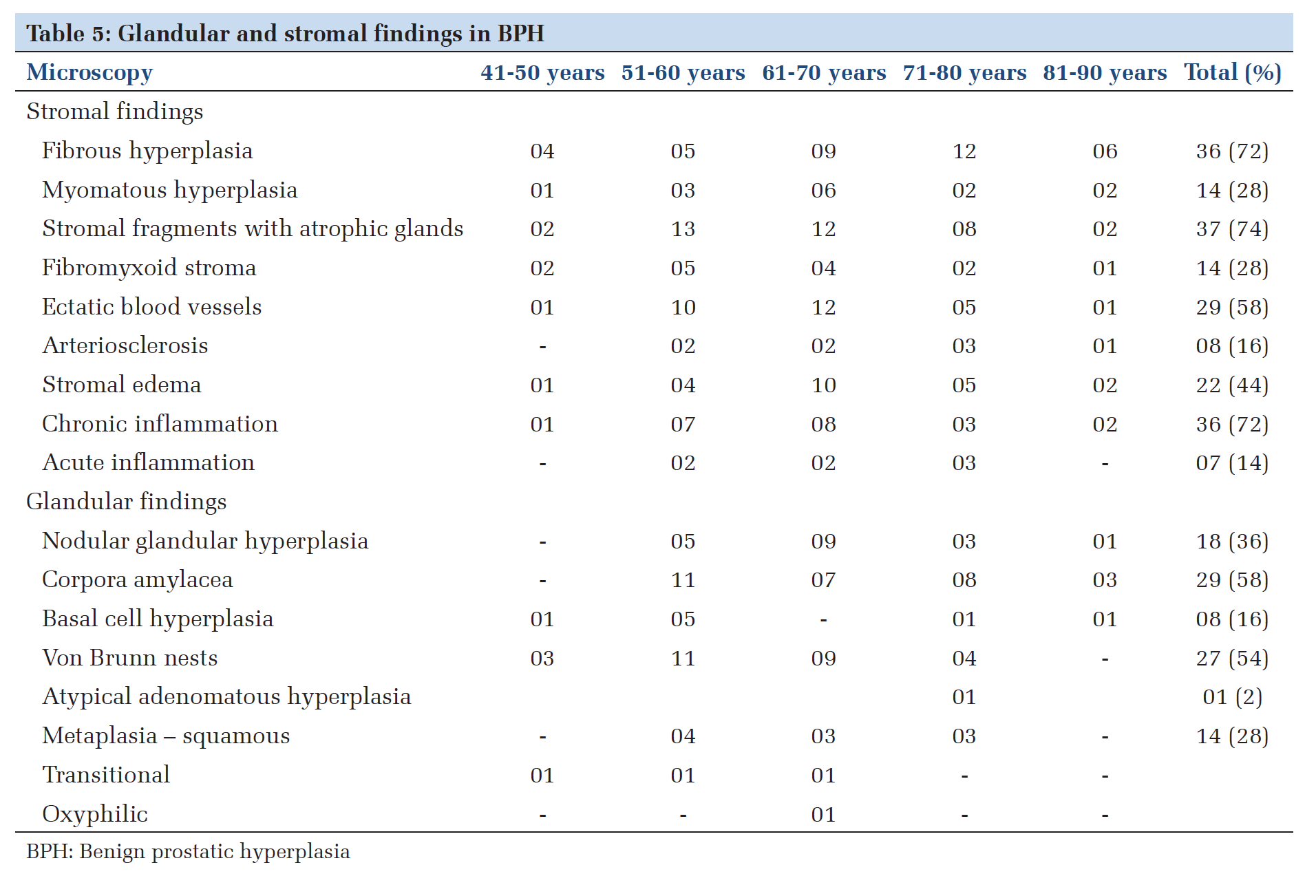
The cases of BPH were categorized into based on the predominant growth pattern as showed in Table 4. Stromal predominance was encountered more common followed by glandular predominance. In the 50 cases of BPH, various histopathological findings in the stroma were noted of which stromal fragments with atrophic glands; fibrous hyperplasia, chronic inflammation, ectatic stromal blood vessels, and stromal edema were commonly encountered. Features of arteriosclerosis were seen in 8 cases. Of the glandular findings corpora amylaceae, Von Brunn nests and metaplasias were commonly seen (Table 5 and Figure 1a and b). In the BPH cases, chronic prostatitis was seen in 72% cases. Two of these showed features of granulomatous prostatitis. Acute inflammation was seen in 14%. Rest of cases showed no inflammation. In the cases with chronic prostatisa moderate to severe degree of lymphocytic infiltrate which included formation of aggregates was seen 72% cases. The lymphocytic infiltrate was accompanied by eosinophils and plasma cells in 14% and 10%, respectively (Table 6 and Figure 1c-g). Among the precursor lesions, 5 cases (8%) of low grade prostatic intraepithelial lesion were identified in the 62 cases studied. Four were identified in 55 TURP specimens and one in 7 needle biopsies. Three out of 5 cases were identified in BPH.
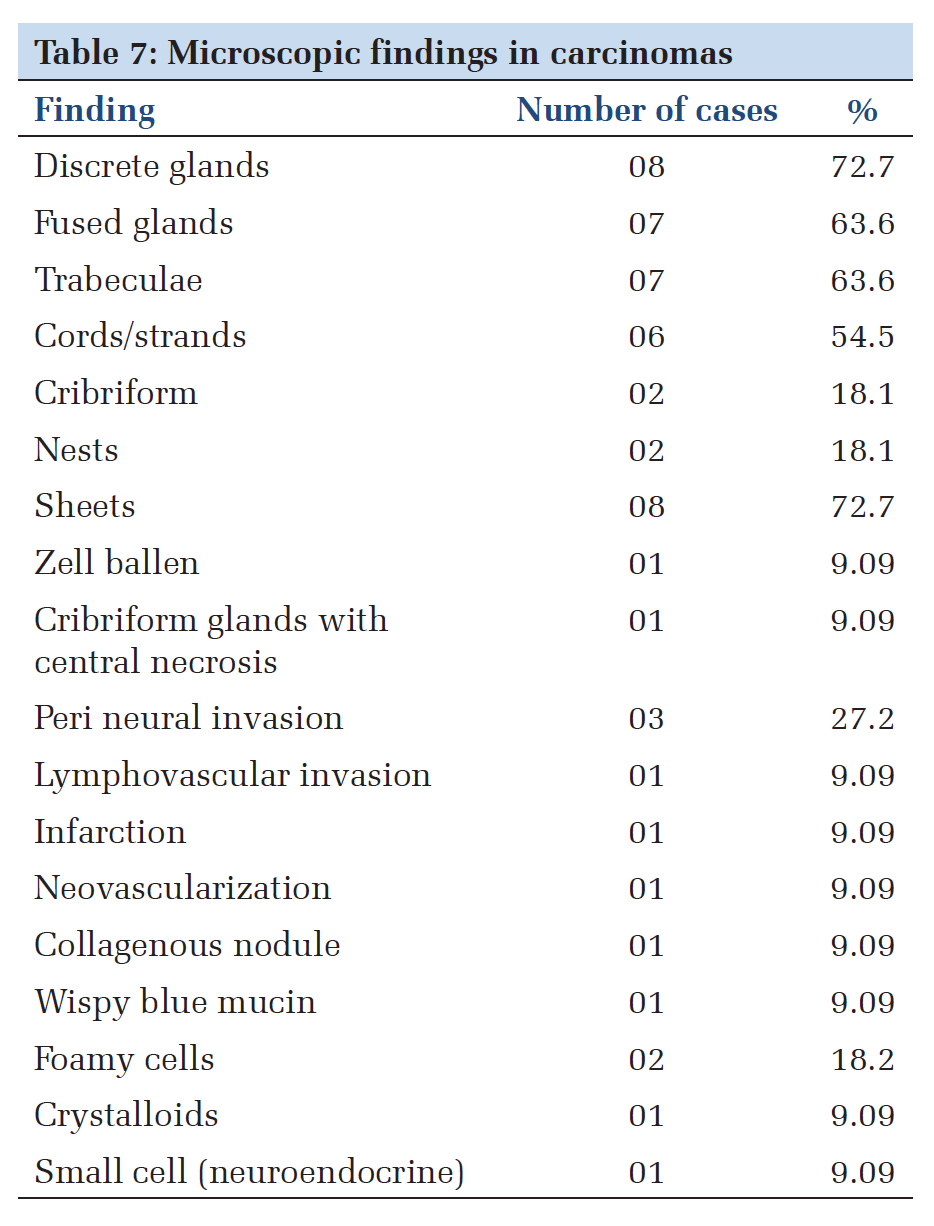
Whereas 1 case each was associated with HGPIN and malignancy. Of the 7 cases of HGPIN, 6 were associated with carcinoma (85%) of which 3 were seen in TURP and remaining 3 in needle biopsies. One case was isolated HGPIN seen on needle biopsy. 11 cases of prostatic adenocarcinoma were identified in the present study. All of them exhibited different growth patterns and were classified according to the predominant growth pattern and graded using the modified Gleasons system (modified ISUP 2005). In this study, the most common pattern seen was discrete arrangement of glands (72%) followed by fused glandular pattern (63.6%) and trabecular pattern (63.6%) of arrangement. One case of prostate carcinoma with neuroendocrine differentiation having features of both small cell component and gland formation was seen. Perineural invasion was noted in 3 (18.1%) cases (Table 7 and Figure 1h and i). Of the 11 cases of adenocarcinoma a Gleason score of 7 was found in 4 (36.3%) cases, followed by 3 cases each (54.4%) in Gleason score of 8 and 9, respectively. Only one case (9.09%) had a Gleason’s score of 10 (Table 8 and Figure 1j-l).
DiscussionTwo most common prostatic lesions BPH and carcinoma cause enlargement of the prostate gland with urethral constriction and various urinary symptoms.[4] In our study, the most common prostatic lesion was BPH accounting for 80.6% of the cases studied which is similar to other studies done in the Asian sub-continent by Aslam et al.[4] (87.5%) and Talukder et al.[5] (77.4%). Deshmukh et al.[6] in a study conducted on 226 cases found a higher incidence (91.6%) of BPH cases compared to our study. The difference could be due to the differences in the nature of biopsies studied with prostatectomies constituting a major portion of the biopsies studied by them. The incidence of isolated PIN detected on needle biopsy range from 0.7% to 20%, with the lowest incidence seen in screening programs.[7] In our study, 1 out of 7 cases where needle biopsy was performed (14.3%), showed isolated HGPIN. This finding is similar to findings by Bostwick and Cheng[8] who found isolated HGPIN in 16.5% of the needle biopsies. The incidence of HGPIN coexisting with prostatic adenocarcinoma was seen in 6 out of 11 cases (54.5%) which correlate with the finding of Anushree and Venkatesh[9] who found 6 of the 12 cases (50%) of prostatic adenocarcinoma to harbor HGPIN. McNeal and Bostwick et al.[10] in 1986 reported an incidence of 33% which is much less than our study. This could be due to criteria for diagnosis of HGPIN was not standardized during the period of their study. The incidence of prostatic carcinoma in biopsies by various studies range from 12.5% reported by Aslam et al.[4] to 24.3% reported by Sinha et al.[11] Carcinoma was identified in 17.7%, in our study. Thus, there is significant variation as to the reported incidence of malignancies in spite of similar cultural and demographic profiles. Sinha et al.[11] has suggested that in a vast and diverse country as India, caution should be exercised in extrapolating data obtained from one region of the country to the other. Anjorin et al.[12] has reasoned this disparity as to the study population, who may seek medical attention at different stages of disease. Since various studies like ours are hospital based and not population-based study, it may not be an accurate indicator of the true incidence of prostatic carcinoma in the society at large. Enlargement of prostate is age related process hence many men older than 50 years will have some histological evidence of BPH and would experience symptoms of urethral compression. In the present study, 88% of the cases were in the 50-80 years range, which is similar to the findings of Anushree and Venkatesh[9] who reported 90.44% of cases in this age range. In the present study, 90.8% of the 11 cases of prostatic carcinoma were found to be in the 50-80 age groups. These findings are similar to the age incidence reported by Anushree and Venkatesh[9] (100%) and Talukder et al.[5] (94.7%). In the present study, the most common symptom in the 62 cases studied was hesitancy (51.6%) and frequency (50%) followed by dysuria (41.9%) and retention (38.7%). These findings are in contrast to a similar study by Anushree and Venkatesh[9] done from an urban population of Bengaluru who found frequency to be the most common symptom accounting for 36.67% followed by difficulty in voiding (28%), acute retention (22%), and dysuria (17.3%). In the malignant cases, they found frequency (38.5%), incomplete voiding (38.5%), and dysuria (38.5%) as the most common symptom in cases that is similar to our study where frequency, retention and dysuria were the most common symptoms in 41.6%, 33.3%, and 25% of cases respectively. Though the manifesting symptoms appear similar there is a marked variation in the rate of incidences which could be due to the rural population studied by us where the level of education, understanding and differentiating one symptom from one another may be poor. BPH results from the proliferation of stromal smooth muscle, fibroblasts and epithelial cells in varying proportions. Briganti et al.[13] have suggested that BPH may be due to increased cell proliferation or decreased cell death. Other commonly encountered findings in BPH are metaplasias, inflammation, and atrophy. In the present study, BPH accounted for 80.6% of cases. Basal cell hyperplasia was seen in 16% of the cases with BPH, which is much higher than the incidence reported by and Garg et al.[14] (3.85%) and Mittal et al.[15] (5.4%). This could be because a higher number of cases studied by these authors. Prostatitis was a common finding in a majority of cases with BPH (86%). This finding is similar to a study by Anjorin et al.[12] who found prostatitis in 90%. Studies by Mittal et al.[15] (58%) and Garg et al.[14] (36.3%) have identified a lower incidence of prostatitis. These differences could stem from the management strategies followed at various institutes. Antibiotics and anti-inflammatory medications may modify the inflammatory pathology on a biopsy. Two cases of granulomatous prostatitis were identified in our study accounting for 4% of BPH cases. This finding is similar to the incidence reported by Garg et al.[14] (3.57%) and Mittal et al.[15] (1.62%). Both our cases showed no acid-fast bacilli. In the present study, metaplasias accounted for 22% of cases with BPH, which parallels with the incidence of prostatitis in our study. Mittal et al.[15] and Garg et al.[14] have reported a much lesser incidence of 3.24% and 0.82% of metaplasia with a corresponding lower incidence of prostatitis, suggesting a role of inflammation in the etiology of metaplasia. In the 50 cases with BPH, a common finding identified in our study (74%) was the finding of isolated predominantly stromal fragments with atrophic glands and ectatic blood vessels which have not been reported by other studies in the literature. The ectatic blood vessels may be feeder vessels related to the prostatic hyperplasia. Arteriosclerosis was seen in 8 cases (16%), who were in the age of 50-80 years which could be related to hypertension. Hypertension has been suggested by Briganti et al.[13] to be involved in pathophysiology of BPH. Epidemiological studies have documented that hypertensive men are more likely to develop BPH. The incidence of atypical adenomatous hyperplasia reported has been seen in 1.65% by Garg et al.[14] and 2.16% by Mittal et al.[15] which correlates the finding of 2% in our study. In the present study, a Gleason’s score of 7 was seen in 36.4%whichwas slightly less when compared to studies by Anushree and Venkatesh[9] (58.3%) and Shirish et al.[16] (52.2%). Talukder et al.[5] has identified majority of his cases (52.6%) with a Gleason’s score of 6. Low grade lesions were not encountered in our study probably because these lesions are usually asymptomatic. All of the cases in this study had a Gleason’s score of 7 or more. This could be because of a delay in accessing the health facility due to illiteracy and low socioeconomic status of the rural population studied. The common patterns in this study were sheeting pattern (72.7%), fused (63.6%) and angulated gland patterns (72.7%). This is in comparison to Garg et al.[14] who found angulated glands as the most predominant pattern (61.6%). This difference could be due to the higher grades of prostatic carcinoma and the lesser number of cases analyzed in the present study. |
ConclusionAs prostatic disease is common, more research is needed for prevention, early diagnosis and in giving therapeutic options for both patients and clinician. The importance of findings of stromal fragments with atrophic glands, ectatic blood vessels, and arteriosclerosis in BPH need to be analyzed in the future in a larger study sample. Only high-grade prostate carcinomas were encountered in our rural setup suggesting routine screening would lead to early detection and better patient management. |
Subscribe now for latest articles and news.