Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i1.24.262
Year: 2025, Volume: 11, Issue: 1, Pages: 79-85
Original Article
Kevin Alfred Samuel1 , Shankar Gururaj Kollampare1 , Rakesh A Rai2
1Department of General Surgery, Father Muller Medical College, Mangalore, 575002, Karnataka, India,
2Professor and Unit Chief, Department of General Surgery, Father Muller Medical College, Mangalore, 575002, Karnataka, India
Address for correspondence:
Rakesh A Rai, Professor and Unit Chief, Department of General Surgery, Father Muller Medical College, Mangalore, 575002, Karnataka, India.
E-mail: [email protected]
Received Date:12 August 2024, Accepted Date:23 November 2024, Published Date:24 February 2025
Objective: To assess the effectiveness of Enhanced Recovery After Surgery (ERAS) protocol in patients undergoing colorectal surgery in reducing the length of hospital stay by early initiation of oral feeds and early mobilization. Methods: A total of 100 patients undergoing colorectal surgeries above 18 years of age for a period of 2 years i.e. from 2018- 2020 were included in the study after obtaining informed consent at a tertiary care medical college hospital. We compared the benefits of ERAS protocol in colorectal surgeries by dividing the study population as ERAS group and controlled group and were assessed using a structured proforma, parameters like type of surgery done, early initiation of mobilization, incentive spirometry and initiation of feeds were all assessed between the two groups. Results: the study population was divided into 2 group of 50 each, all the ERAS group of patients were mobilized on post operative day (POD) 1 or 2 irrespective of the surgery done and the mean duration was 1.2 days +/- 0.5 days and initiated with incentive spirometry from POD 1 with the mean duration being 1.02+/- 0.1 and the patients with laparoscopic surgery had a reduced pain and early recovery time and thus reduced the length of hospital stay in the ERAS group 5-8 days when compared to the control group 10-11 days. Conclusion: ERAS is a well-designed protocol and had a positive impact on its application in patients undergoing laparoscopic colorectal surgery in terms of decreasing the length of hospital stay.
Keywords: ERAS, Colorectal, Carcinoma, Laparoscopic surgery
In India, the annual incidence rates for colon cancer and rectal cancer in men are 4.4 and 4.1 per 100000, respectively. Risk factors for Colorectal carcinoma (CRC) can be broadly divided into genetic and environmental or lifestyle-related factors. Most CRCs are sporadic, although genetic factors increase the risk considerably. Although a highly common procedure with approximately 330,000 cases per year.1 The 5-year relative survival rate for CRC has increased moderately from 50% in the mid-1970s to 64% during 2009-2015.2 The high bacterial count within the colon and rectum results in the increased surgical site infection rate for these procedures and is the most frequently documented adverse event in colorectal patients during the 30-day post-operative period and also, hospital post-operative length of stay for these patients is extremely high (6-11 days on average), and about 23% of these patients are readmitted to the hospital within 90 days. 3
To improve outcomes for colorectal surgery patients, the Enhanced Recovery After Surgery (ERAS) protocol was developed by a Danish surgeon, Henrik Kehlet, in the 1990s. Also known as “Fast Track Surgery” the protocol involved a bundle of interventions that were focused on expediting recovery & improve perioperative outcomes of the patients by 4 Several Meta-analyses conducted on ERAS studies generally show a decrease in the incidence of post-operative complications, and a significant decrease in length of hospital stay (LOS). Varadhan et al reviewed 6 randomized control trial (RCT) studies and found significant reductions in length of stay LOS and complication rates. 5 Nicholson et al reviewed 38 RCTs and concluded that there were significant reductions in LOS and risk of all complications within 30 days. 6 Greco et al reviewed 16 RCTs and reported as ERAS reduced overall morbidity and LOS without increasing the readmission rate.7 In 2009 the ERAS group published the guidelines for enhanced perioperative surgical care. It was a consensus review of perioperative care based on evidence available for each element of the multimodal pathway. 8
There are several key elements that make up any ERP. These elements are diverse & varied and include a multidisciplinary team approach to patient care. The key elements include: preadmission information and counselling, selective bowel preparation, carbohydrate loading and avoidance of preoperative fasting, avoidance of pre-anesthetic medication, avoidance of nasogastric tubes, thoracic epidural anesthesia, short-acting anesthetic agents, avoidance of sodium and fluid overload, short incisions, maintenance of normothermia intraoperatively, standard early mobilization, non-opioid oral analgesia and Nonsteroidal anti-inflammatory drugs (NSAIDs), prevention of postoperative nausea and vomiting, stimulation of early gut mobility with early enteral nutrition, early removal of catheters and drains.
Not all ERPs include all the above elements. It is the combination of elements rather than any one specific element that is important when developing and establishing any ERP.
This was a prospective study conducted in Department of General Surgery, Father Muller Medical College, Mangalore, Karnataka, India from November 2018 to August 2020 to evaluate the effectiveness of enhanced recovery after surgery protocol in patients undergoing colorectal surgery. The objective of the study being to determine whether perioperative fluid management, early enteral nutrition, early mobilization, and avoidance of drains & urinary catheters accelerated the postoperative recovery and reduced the length of hospital stay in patients after colorectal surgery. The source of the data was collected from patients who underwent colorectal surgery in the Department of General Surgery, Father Muller Medical College, Mangalore, Karnataka, India.
The study was conducted according to the ethical standards required after obtaining ethics committee clearance (EC No: FMMCIEC/CCM/631/2018). Patients of either sex, aged >18 years, who were planned for colorectal surgery electively and are willing to give a written informed consent were included in the study. A detailed information sheet about the study with the methodology, risk and benefits from ERAS protocols were provided to the patients in two languages (English/Kannada). Patients were given the choice to refuse/withdraw their consent anytime from the study. Patients were divided into ERAS group and non-ERAS group by random sampling. The inclusion criteria of the study being: patients above 18 years of age, patients undergoing elective colorectal surgery (open/laparoscopic), and benign & malignant diseases of the colon. The exclusion criteria were pregnant women, emergency surgery due to bowel obstruction caused by colorectal cancer, bowel perforation with peritonitis and patient not willing to consent for the study.
ERAS group of patients had a pre-operative family and patient counselling session where the diagnosis of the patient & the plan of action, the roles played by each of the family members & the patients were explained and written informed consent for the same was taken. Patients preoperatively had reduced fasting time. Mechanical bowel preparation was avoided in all patients except patients undergoing ultra-low Anterior Resection who were provided with mechanical bowel preparation. Venous thromboembolism prophylaxis was given preoperatively and postoperatively. Pre-medications were avoided in patients in ERAS group prior to surgery.
Intraoperatively, patients were actively warmed with an external warmer to avoid hypothermia. Patients underwent surgery under general anesthesia with insertion of an epidural catheter to provide postoperative analgesia in the ERAS group. Patients were selected for laparoscopic or open surgery based on the general condition of the patient and the stage of the disease and willingness of the patient to undergo laparoscopic surgery. Resection and anastomosis were done using linear staplers & endo-staplers (Healthium Medtech Limited, Bangalore, India) for the open & laparoscopic surgery respectively. Nasogastric tubes and drains were avoided in ERAS group, only placed when excessive dissection and increased blood loss was expected. Antiemetic prophylaxes were given only to the high-risk category group. Fluid management in the study group was done as per body weight of the patient and a neutral fluid balance was maintained in the body.
Postoperatively patients in ERAS group were provided analgesia through epidural and later converted to oral medications. Oral feeding in the study group was initiated within the first or second POD, Study group patients were mobilized on first or second POD and given incentive spirometry. Discharge of the patients were based on the following criteria: tolerating oral solid diet, passage of stools/stoma functioning, pain control with oral medication and independent mobility. Complications post procedure like Intestinal leaks, surgical site infection, cardiorespiratory compromise, pressure sores, deep vein thrombosis (DVT), & death were closely monitored and recorded.
Non-ERAS group patients were evaluated, pre- and post-operative care was given according to the traditional surgical protocols as per institution standards. Preoperatively non-ERAS group patients were kept on fasting overnight and initiated with IV fluids from early morning. Mechanical bowel preparation was given to all the patients. Pre-medications were given to the patient before surgery.
Intraoperatively patients were given general anesthesia with or without epidural anesthesia. Nasogastric tubes and drains were placed in all patients intra-operatively. Post-operatively patients were kept nil per oral until the passage of flatus/appearance of bowel sounds. Patients were mobilized on POD 3-4. Drains were removed only after the total drain output was less than 50cc for 48 hours. Ryle’s tube was removed after appreciation of bowel sounds and if tolerating liquids. Foley’s catheter was removed once the patient was fully ambulating. Discharge criteria were similar to that of the ERAS group and complications rates & length of hospital stay was also noted. All the parameters were evaluated and compared with ERAS group and results were analyzed.
For categorical variables, descriptive statistics such as frequency & percentages were used and for continuous variables mean & standard deviation were used. Unpaired t test was used to find the difference between the groups for continuous data. Fisher’s exact test was used to find the difference between ERAS and non-ERAS group for categorical data. P<0.05 was considered significant. SPSS version 23 was used to analyze the data. Level of significance: * p<0.05 was considered significant; ** p<0.01 was considered highly significant; ***p<0.001 was considered to be very highly significant. p>0.05 was considered non-significant.
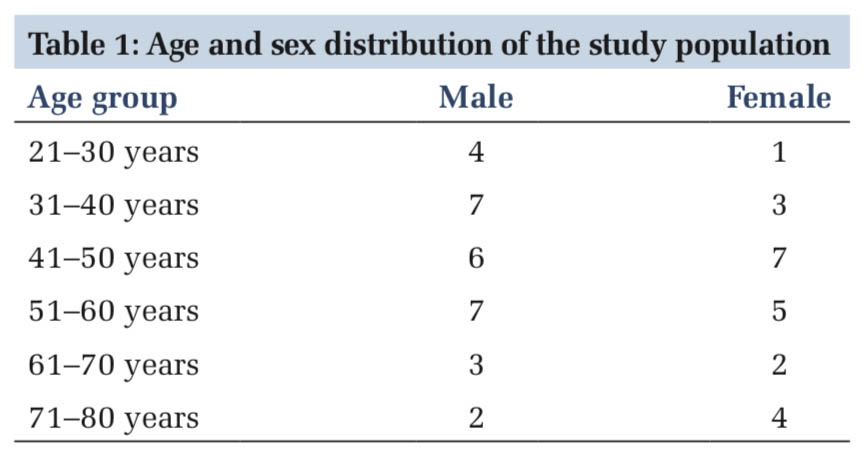
The study included 50 patients in each group (ERAS and non-ERAS). ERAS group had 26 males and 24 females, and the non-ERAS group had 27 males and 23 females comparable to each other with age, the mean age in the ERAS group was 61 years and the non-ERAS group was 63 years (Table 1).
|
Sl. No. |
Study groups |
Gender of the participants |
Age (SD) |
Statistics |
|
|
Male |
Female |
p value |
|||
|
1 |
ERAS |
26.0 |
24.0 |
61.30 (12.5) |
>0.05* |
|
2 |
non-ERAS |
27.0 |
23.0 |
63.58 (11.8) |
|
*Fishers exact test showed non-significant difference in gender & age between the groups (P>0.05). SD: Standard Deviation
Post-operatively all the ERAS group patients were initiated with oral feeds within 1 or 2 days, the mean duration of initiation of oral feeds being 1.3 days +/- 0.5 day. But in the non-ERAS group, oral feeds were initiated 3-5 days after the surgery with the mean duration being 3.9 days +/-0.7 days and when compared, these values were statistically very highly significant with the p value of <0.001 (Table 2). This reduced the occurrence of complications like paralytic ileus, intestinal leaks, intra-abdominal infections, and surgical site infections in the ERAS group when compared with the non-ERAS group (Figure 1).
|
Sl. No.
|
Study parameters
|
Study groups
|
Statistics
|
||
|
Non-ERAS |
ERAS |
T value |
p value |
||
|
1. |
Early oral nutrition |
3.9±0.7 |
1.3±0.5 |
21.112 |
<0.001 |
|
2. |
Early ambulation |
3.2±0.6 |
1.2±0.5 |
18.995 |
<0.001 |
|
3. |
Breathing exercises |
2.8±0.5 |
1.02±0.1 |
23.657 |
<0.001 |
Statistical test used: Fischer’s exact test. Level of significance: * p<0.05 was considered significant; ** p<0.01 was considered highly significant; ***p<0.001 was considered to be very highly significant. p>0.05 was considered non-significant.

All the ERAS group of patients were mobilized on POD 1 or 2 irrespective of the surgery done and the mean duration was 1.2 days +/- 0.5 days. In the non-ERAS group patient’s ambulation was initiated after 2-3 days post-surgery with the mean duration being 3.2 +/- 0.6 days and the results when compared were statistically very highly significant with the p value of <0.001 (Figure 2). ERAS group patients were initiated with incentive spirometry from POD 1 with the mean duration being 1.02+/- 0.1. Whereas, in the non-ERAS group patient’s breathing exercise were initiated 2-3 days post-surgery and the mean duration for initiation of breathing exercise were 2.8 days +/- 8 days and the results when compared to each other were statistically very highly significant with p value of <0.001 (Figure 2). No drains, adequate analgesia (non-opioid) and early catheter removal in the ERAS group added a plus point in the early mobilization of the patient and prevented catheter associated urinary tract infections, early mobilization thus reduced the occurrence of complications like DVT, pneumonia, pulmonary embolism in the ERAS group (Figure 2).

With the implementation of the ERAS protocol, we can clearly establish that early enteral feeding and early mobilization helps in reducing the complication rates in patients undergoing a major colorectal surgery and thus reducing the length of the hospital stay that is 7 days in the ERAS group and 12 days in the non-ERAS group with a p value of <0.05 (Figure 3) which is statistically significant.

ERAS group of patients who underwent laparoscopic resection of colorectal tumor were initiated with oral feeds from POD 1 and discontinued iv fluids from POD 1-2 by strictly following with these protocols, such as (a) limiting opioid administration (b) use of minimally invasive surgery, (c) Avoiding nasogastric tube (d) maintaining fluid balance with goal-directed fluid therapy, which limited the duration of postoperative ileus when compared to the non-ERAS group. In the non-ERAS group, patients were treated with traditional methods with delayed initiation of oral feeds and nasogastric tube insertion. In the non-ERAS group, 19 out of 50 patients had postoperative ileus and required intervention whereas the ERAS group, none of the patients had paralytic ileus.
A study by Petrelli NJ et al. 9 reported that the factors related to failure of early feeding was blood loss during the operation in open cases, on the contrary Rohatiner T et al conducted study in elderly patients undergoing colorectal surgery and reported that use of laparoscopic surgery was associated with early initiation of postoperative feeding. 10 A multicenter study by, Zhuang CL et al commented on encouraging patients to drink when free of nausea after the surgery and initiation of oral diet can usually be started within 4 hours after surgery, 11 on the contrary Padhi S et al suggested on discontinuation of intravenous fluid by POD 1 and should be restarted only if clinically indicated at a rate of 25–30 ml/kg per day with 70–100 mmol sodium/day, and potassium supplements (up to 1 mmol/kg/day). 12
Randomized study by Ortiz H et al, reported that early oral feedings in patients undergoing colorectal surgery had significant improvement in the patients general condition and decreased need for enteral nutrition.13 El Nakeeb A et al who conducted a RCT, also concluded that early oral feeding helps to improve the general condition of the patient and reduces morbidity, complications and helps in early discharge from the hospital. 14
Meta-analyses 15, 16 also demonstrated that early (<24 hour) oral feeding accelerated gastrointestinal recovery time and decreased the hospital length of stay. The rate of complications and mortality were also decreased with early feeding. A randomized trial conducted in patients undergoing open surgery reported no significant differences in any outcomes (post-operative ileus and length of stay). 17 But on the contrary study by Lee TG et al demonstrated the benefits of early oral feeding were more in laparoscopic surgery with an ERP. 18
A Cochrane review of 81 studies after major abdominal surgery reported that patient’s chewing gum had faster return of bowel sounds and were able to pass flatus and had bowel movements earlier.19 Studies with various agents like laxatives & oral bisacodyl, oral magnesium oxide have been tested for efficacy and have reported to be beneficial in reducing duration of post-operative ileus in patients undergoing colorectal surgery.20 Studies reported that oral coffee administration in patients undergoing colorectal surgery reduced the incidence of post-operative ileus. 21 Another RCT revealed significant decline in post-operative ileus with de-caffeinated coffee administration than with caffeinated coffee in patients undergoing left-sided laparoscopic colectomy. 22
ERAS group of patients were mobilized from POD 1 and were initiated with breathing exercises when compared to the non-ERAS group, where mobilization was initiated only after 2-3 days of surgery. When compared, the ERAS group had lesser incidence of pneumonia, DVT and other complications. Studies report that prolonged bed rest is associated with higher risk of pulmonary complications, thromboembolic complications. Hence early mobilization within 24 hours, 8 to 10 hours per day by POD 1 is required for colorectal surgery with ERP to reduce these complication rates. 23 Colorectal Patients in ERPs meet mobilization targets sooner compared with conventional care due to active family support and aggressive physiotherapy & reduced pain. 24 Observational study reported that adherence to active mobilization by patients in ERP are in range of 28% to 69% and was a significant predictor of earlier discharge in most studies. 25 An international multicenter RCT comparing goal-directed mobilization versus usual care in ICU setting reported the impact of mobilization in reducing the pulmonary complications and also thrombo-embolic phenomenon. 26 On the contrary lack of early mobilization after major abdominal surgery has been associated with risk of developing pulmonary complication. 27
Silva et al reported patients with supervised early mobilization POD1 plus breathing exercises after an upper/lower GI surgery had the shortest hospital stay. 28 Ahn et al conducted a study with colon cancer surgery patients with supervised in-patient exercise program including core, stretching, to conventional care and reported that the exercise group had shorter hospital stay and shorter time to pass flatus. 29 But on the contrary, a randomized trial evaluating the benefits of walking and out of bed activities after colorectal surgery in ERP reported that there was no effect on hospital stay or complications. 27
ERAS group of patients have a reduced LOS with the mean duration of hospital stay to be around 6.74 +/- 0.74 when compared to the non-ERAS group of patients whose mean duration of hospital stay was 11.2 +/- 1.8. The reduced length of hospital stay in ERAS group is attributed to the early oral feedings and active mobilization, which helped in the avoidance of complications in the patients leading to faster recovery & early discharge from the hospital.
ERAS being a multi-modal approach enables the patient to recover earlier, reduces the post-operative complication rates and hence decreases the length of hospital stay significantly. Thus, reducing the hospital costs. It’s evident that ERAS pathways have a positive impact on the patient’s quality of life during and after the hospital stay, which is of even greater importance. ERAS principles also emphasized the need for early oral nutrition and early mobilization, avoidance of nasogastric tube, early removal of drains/catheter are the key factors in the prevention of post-operative complication of paralytic ileus, DVT, pulmonary thromboembolism, aspiration pneumonia, urinary tract infection which are the major predictors for extending the hospital stay and increase in cost factors for successful implementation of ERAS.
Subscribe now for latest articles and news.