Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v8i3.22.274
Year: 2022, Volume: 8, Issue: 3, Pages: 236-245
Original Article
Suchismita Sarkar1 , Dinesh Badyal2 , Ritu Sharma3 , Manoj Patki4 , Taskin Khan5 , Loveena Oberoi6
1Associate Professor, Department of Anatomy, Shri Atal Bihari Vajpayee Government Medical College, Faridabad, 121004, Haryana, India,
2Professor, Department of Pharmacology & Medical Education, Christian Medical College, Ludhiana, India,
3Associate Professor, Department of Obstetrics and Gynaecology, Government Institute of Medical Sciences, Greater Noida, 201310, Uttar Pradesh, India,
4Associate Professor, Department of Social Medicine, Zoram Medical College, Mizoram, India,
5Associate Professor, Department of Ophthalmology, Hamdard Institute of Medical Sciences & Research, 110062, New Delhi, India,
6Professor, Department of Microbiology, Government Medical College, Amritsar, Punjab, India
Address for correspondence:
Suchismita Sarkar, Associate Professor, Department of Anatomy, Shri Atal Bihari Vajpayee Government Medical College, Faridabad, 121004, Haryana, India.
E-mail: [email protected]
Received Date:25 February 2022, Accepted Date:13 July 2022, Published Date:28 November 2022
Background: The one thought that has taken precedence over the conscious cognition of the cerebral cortex of Indian medical educators is how to implement the Competency Based Medical Education (CBME) program. A revolution that has occurred after 21 odd years, indeed should captivate the change leaders of health professions education. COVID -19 pandemic has posed on medical educators, who enthusiastically implemented the CBME curriculum from 2019 in India, an uphill struggle to understand, apply and eradicate the challenges in effectively implementing the newer elements of the CBME curriculum. A number of newer elements namely Foundation course, Early Clinical Exposure, Electives, Integration, and Learner Doctor Method of clinical clerkship, have been introduced into the new undergraduate medical curriculum. Health professions educators in India, being beginners in implementing these newer elements of the revolutionary 2019 CBME curriculum, it is pertinent to answer the queries that tickle the minds on how to implement and address the anticipated challenges and where to look for solutions. Aims: The authors aim to address some of these queries by giving ready to use templates, guided stepwise breakup of implementation, experience based solutions to the challenges, for various newer elements. They elaborate upon the opportunities of a positive change that medical education in India so direly needs. Conclusion: The stumbling blocks in implementing such a dynamic and thoroughgoing program needs the due contemplation to navigate successfully as directed by the National Medical Commission or erstwhile Medical Council of India.
Keywords: Foundation course, Electives, Integration, Early clinical exposure, Clinical clerkship
India, is a country with a 562 operational medical colleges as of 2020, to meet the doctor population ratio as per recommendations of World Health Organisation (WHO). The annual output of 84649 MBBS students, achieving the current doctor patient ratio at 1:1456 under the aegis of the erstwhile Medical Council of India (MCI).1, 2 Thus, was the call for a reform in Indian medical education to set its standards that match the global health professions education norms. The traditional Indian medical education focused on imparting instructional strategies irrespective of how the product i.e. the learner turned out at the end 5 and half years of education. The need of the hour was an outcome based approach where the outcome/ product is the guiding force behind curricular decisions, and the processes to attain these become secondary. Hence, competency based curriculum can be seen as an appropriate outcome based approach introduced in the Indian medical curriculum.3
The rationale for choosing competency based curriculum (CBC) for affecting an Indian medical graduate, can be summed up by the following themes:
Outcome focused approach with accountability of attaining all essential competencies.
Emphasis on abilities required to cater to needs of the Indian society, not just acquiring requisite knowledge.
Depreciate the value of time based training to insistence on developmental progression of abilities.
Advocating learner centred approaches in instructional strategies.
The last reform in the graduate medical education regulations was more than two decades back, in 1997. Amongst the strengths of the traditional curriculum were, it being time-tested and withstanding for past two decades, focussed on a strong foundation of the basic sciences' knowledge base, established teacher centered approaches to pedagogies and assessment methodologies that were built upon for years, and support received from peers for the learners during the graduation years.
The traditional curricula when evaluated against the global standards in medical education laid by the World Federation of Medical Education (WFME), observed the following – lack of integration of core basic sciences to the clinical subjects, with teaching occurring only in silos of the departments, over teaching and cognitive overloading in various subjects leading to repetition of topics throughout the curriculum , inadequate practical skills of graduates at the end of curriculum, despite strong knowledge base from post-graduation entrance oriented approach to graduate medical education, and graduates having poor self-directed and lifelong learning skills for continuing professional development in their fields. Hence, when the weakness outweighed the strengths, came the recommendations by an expert group commissioned by the WHO. 5, 6 The board of governors of the apex regulatory authority erstwhile MCI, gave the recommendations in its Vision 2015 document to transition to a competency based graduate and postgraduate curricula.7 This foresight of the health education policy-makers came into effect with the launch of Graduate Medical Education Regulations 2019 (GMER, 2019). 4 In this article we review the newer elements of the competency based undergraduate curriculum in India and discuss the strategies for implementation, opportunities for learner centered learning and challenges to effectively implementing the newer elements.
The GMER 2019 continued the traditional duration of four and half years, followed by one year compulsory rotatory internship, for the undergraduates. However, it introduced a number of new teaching learning elements:
Foundation Course
Early clinical exposure
Electives
Alignment and Integration
Learner – doctor method of clinical training
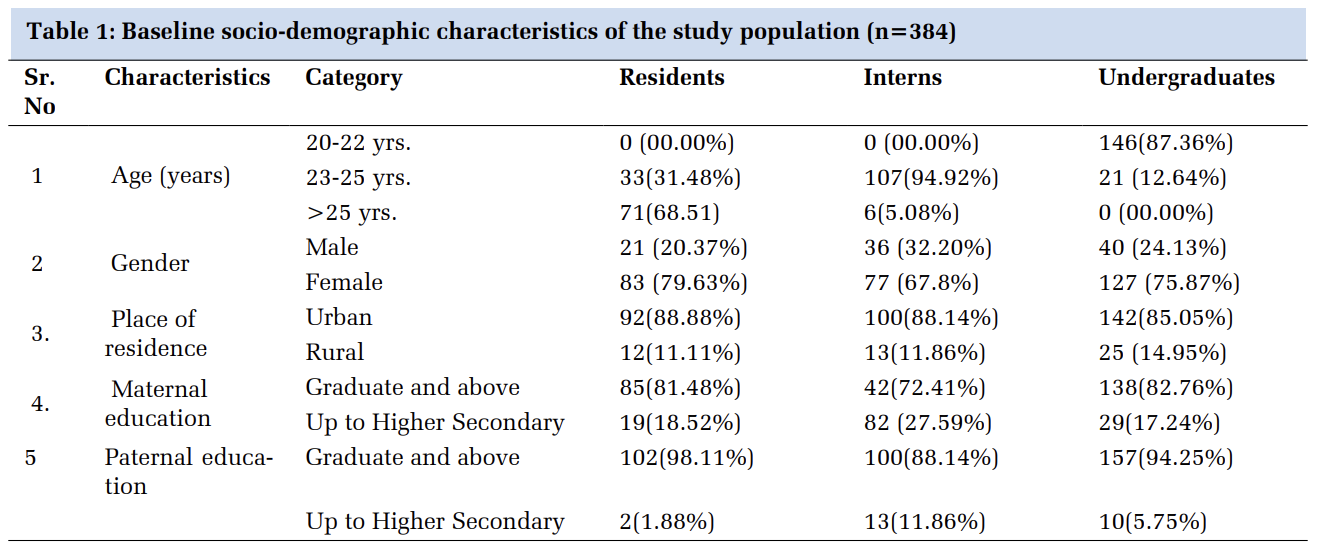
Foundation course is a one-month-long program envisaged to create a smoother transition from high school into the medical college, acting as a period of acclimatization and familiarization. Such initiatives should be carried out to prevent ‘doctor burn out’ akin to lack of proper induction into the medical career, recognising the steep learning curve during this transition period.8, 9 The foundation course elaborated into six modules of Orientation, Skills, Field visit to Community Health Centre, Professional Development including Ethics, Sports and Extracurricular activities, Computer Skills, and Language enhancement program.10 Figure 1 shows a suggestive timetable template to organise this one month foundation course to exact the hourly utilization of the 175 hours allocated by the NMC/MCI to conduct it. The topics covered in these sessions should include more of interactivity rather than passive delivery of the instruction accomplishing the learning by doing paradigm. The Table 1 shows the examples of interactive lesson plans for two of the Foundation course ‘shows how level’ competencies, from the basic skill and enhancement of Language, communication and computer skills module.

|
COMPETENCY NUMBER 1 |
DOMAIN |
LEVEL |
OBJECTIVES |
|
FC 5.1 Demonstrate ability to communicate with patient and families, be aware of barriers to communication and appropriate ways to respond |
C |
SH |
At the end of the session student should be able to FC 5.1.1 Describe the basic components of good communication skills FC 5.1.2 Differentiate between good communication and bad communication FC 5.1.3 Discuss the impact of good and bad communication FC 5.1.4 Describe various barriers to good communication FC 5.1.5 Reflect on doctor patient interactions in different case vignettes. |
|
CONDUCT OF SESSION |
T-L METHOD |
TIME |
INFRASTRUCTURE REQUIREMENTS |
|
INTRODUCTION |
Interactive lecture |
15 min |
Audio visual aids |
|
TYPES OF COMMUNICATION |
Patient video pre-recorded |
15 min |
Audio visual aids |
|
DEMONSTRATION: Bad communication Good communication |
Different case scenarios of doctor- patient interaction given and Role play enacted |
Prep - 20 min Role play – 40 min Discussion – 10 min |
Students divided into small groups of 10 each with one facilitator. Students prepare for the bad and good communication in each scenario. Every group enacts out the scene Debriefing in small groups with discussion from the facilitator |
|
WRAP UP |
Reflect |
20 min |
White board, Flipped charts, Markers |
|
ASSESSMENT |
Formative Assessment |
||
|
COMPETENCY NUMBER 2 |
DOMAIN |
LEVEL |
OBJECTIVES |
|
FC 2.5 Demonstrate proper hand washing and use of personal protective equipment (PPE) |
|
SH |
FC 2.5.1 Demonstrate correct techniques of Hand washing. FC 2.5.2 Demonstrate correct techniques gloving/degloving, FC 2.5.3 Demonstrate correct techniques disinfection and sterilisation |
|
CONDUCT OF SESSION |
T-L METHOD |
TIME |
INFRASTRUCTURE REQUIREMENTS |
|
INTRODUCTION |
Interactive lecture |
15 min |
Audio visual aids |
|
TECHNIQUES OF HAND WASHING DONNING AND DOFFING OF PPE |
Patient video pre-recorded |
15 min |
Audio visual aids |
|
DEMONSTRATION: HANDWASHING USE OF PPE |
Demonstrate Observe Assist and Perform (DOAP) |
Prep - 20 min DOAP – 40 min Discussion – 10 min |
Students divided into small groups of 10 each with one facilitator. The facilitator demonstrates the correct technique and then the helps the students perform the technique, and gives feedback on improvement. Arrangements for handwashing area should be made available to conduct the session. |
|
WRAP UP |
Reflect |
20 min |
White board, Flipped charts, Markers |
|
ASSESSMENT |
Formative Assessment |
||
Early Clinical Exposure (ECE) module allows the learner to understand the clinical application and context of the basic sciences knowledge during the preclinical years. The three main elements of ECE include :Basic Sciences correlation; Clinical skills; and Humanities. 11 It involves active, experiential learning with clinical case scenario discussions with faculty giving the learner the requisite context to the basic sciences education. The medical humanities is introduced to explore how as humans we can engage with specific experiences of patients, doctors, health, illness, and suffering.12, 13 The clinical experience can be given in the classroom settings with discussion on paper cases, patient videos of examination, role plays on patient interviewing skills etc. Few of the experiences can also be planned in the primary health care facility at the community level or in the hospitals wards, depending upon the availability and affordability at the time of conduct. Table 2 is an example of a lesson plan of an ECE session of 3 hours in classroom setting that was conducted by one of the authors for phase I MBBS students in a North Indian medical college.
|
ECE MODULE ANATOMY |
|
Topic of Basic Science Correlation: Peripheral nerve injuries of upper extremity |
|
Goal - The student must be able recognize the relevance of anatomy of the peripheral nerves (ulnar, radial, and median nerves) in the presenting symptomatology of peripheral nerve injuries patient. |
|
Competencies expected:
|
|
Objectives: At the end of the ECE module I MBBS student shall be able to:
|
|
Learning Experiences: Total time: 3 hours Introduction and instruction to students: 20 mins. Exposure to clinical context and discussion: 90 mins (Three Clinical Case Scenarios) Summary and conclusion: 10 mins Reflection: 30 mins Assignment: 30 mins |
|
Formative assessment: Submit assignment on the topic anatomical basis of peripheral nerve injuries. (Subjective write up) |
|
Reflections can be structured using the following guiding questions:
|
|
Program Evaluation: Feedback from students to evaluate for improvements in the module 1. How helpful has the ECE module been in improving your knowledge about peripheral nerve injuries ? 2. Which components of the program helped you to learn? 3. Did the ECE module make learning basic science subjects more interesting? 4. Are you motivated to read further on this topic as a result of participating in ECE? 5. Suggest changes in the program that will help you learn still better. |
To inculcate inquiry based experiential learning, into the MBBS curriculum, so the students are exposed to research at an early stage in the field of their choice, is the essence behind this module. This will be implemented for the first batch of MBBS 2019-20 under the CBME curriculum, in the year 2022 tentatively, before the commencement of MBBS phase III part 2. It is to be conducted into two compulsory block sessions of one 4 weeks duration each. For Block 1 session, the students have to choose from Pre and Para-clinical subjects e.g. join ongoing research projects in these departments. The purpose of block 2 is to provide the learner an explorative experience with guided clinical experience in a specialty of choice.14
The following can be used as ‘nine determine steps’ as a prerequisite for planning each of the blocks in electives by the institutions and departments:
Determine the Venue: Explore all the possible options for electives in the institution.
Determine the Number of Students : It is also pertinent to determine the number of students (5-10) in all the places that have been finalised for the electives.
Determine the Guide: Identify the faculty responsible for the coordination, organisation and execution of the electives from each of the places for electives.
Determine the Module: The faculty preceptor from the individual departments then should chalk out the 4 week module with well-defined learning objectives that they expect students to acquire during the block posting of the electives.
Determine the Timetable: The schedule of the activities that the students need to undertake should be mapped out precisely in a monthly timetable.
Determine the Learning Resources: The learning resources should also be sketched out on print for the students before the actual elective block posting starts.
Determine the Infrastructural Requirements: To organise a month long effective elective program, it is pertinent for the faculty preceptors and the departments to arrange for the training of the stakeholders, availability of resources, and sensitization of the staff etc.
Determine the assessment of learning: The formative assessment methods should be available for the students before the block rotations. For assessments logbook records, portfolio entries, project reports, demonstration of skills acquired ,guide’s report etc. should be included.
Determine the structure of program evaluation: Every new program should be evaluated for refinement during future such organisations.
All these steps need to be defined before the electives and should be displayed by the institutions for the students. This will help them to make an informed decision about which specialties to choose from to get an authentic student driven learning to experience.
Integration is to unify different disciplines to correlate the contextual learning between basic and clinical sciences and to cross interdisciplinary boundaries to scaffold the knowledge base for the learners for specific topics. A variety of ways can be applied to implement the processes of correlation across disciplines as highlighted in the regulations laid by the apex regulatory authority for Indian medical education. With an example of Tuberculosis (Disease specific topic), we have tried to explain the intricate differences in the various types of integration that need to be implemented (depicted in Figure 2):

Temporal Coordination/ Alignment — Organising the same phase subjects timetable in a way, to align the organ based or disease based instruction across disciplines to go side by side. The different subjects of the same phase teach the same system topics in that time period. Example: Final year MBBS departments of Medicine, Paediatrics, Obstetrics and Gynaecology could teach tubercular disorders simultaneously achieving their specific learning objectives.
Shared/ Joint development of module — Learning objectives from different subjects tackled in a joint teaching session. Example: In second year of MBBS, a joint session between Microbiology, Pathology and Pharmacology on the Tuberculosis causing agent, the pathophysiology, and Antitubercular drugs, combined as a single session.
Correlation — A separate integrated teaching session is introduced into the curriculum, taking bits from various topics. Example: Linker Case of Tuberculosis integrating across all phases achieving learning objectives from different disciplines.
Nesting — The facilitators target the learning objectives from other disciplines within their own subject domains. Example: In a second year MBBS class in Pharmacology on Antitubercular drugs, could include the learning objectives of the National Tuberculosis Control Program from Community Medicine.
It is pertinent to achieve alignment in the teaching of the various phases to the maximum extent possible. Integration should be done horizontally (across same phase subjects) and vertically (across different phase subjects) by ways of sharing, correlation, and nesting to the extent of 20% of the total number of hours allocated to each discipline. 15
Learner Doctor method of clinical training is a novel approach which is based on immersive experiential learning in longitudinal patient care. It starts from first year of MBBS with ECE sessions and hospital and community orientation visits. This continues throughout the rest of the medical curriculum with ascending complexities of bedside discussion by the faculty preceptors with the students. The learners get an empirical understanding of the value of healthcare team by being a part of the team from second year onwards. They track the progress of inpatient admissions individually till they are discharged to become apprised to the patient care continuum. A number of frameworks have been developed to teach and evaluate the learning during clinical clerkship.16
The authors propose a suggestive plan based on the guidelines provided by the NMC, for carrying out Learner Doctor method of Clinical training for the Indian scenario, to be researched and evaluated further. Figure 3 shows the suggestive plan for conducting the clinical clerkship program for every phase of the MBBS curriculum. 17 Since for the phase I, the clinical clerkship program is conducted by ECE, visits to the community and orientation visits to the hospital, the pictorial representation of the plan includes from phase II to phase III part II.

The newly launched CBME curriculum has posed a number of challenges to the stakeholders and the institutions. Stakeholders who have felt the brunt of this change the most are the students and the teachers. One of the primary concerns that have been felt, amidst the students across the country, is the uncertainty introduced with the revised curricula. With the COVID pandemic hitting the world in the first year of implementation of this curriculum, times have never been so testing for the country at large.
To organise the plethora of student centred approaches to be conducted in small groups activities, introduced by the CBME, the faculty number seem to be the bottleneck that the institutions feel at large. Ideally the recommended faculty to student ratio for small group activities should be of 1: 10-15, but institutions are struggling to achieve this ratio with the existing faculty. To meet the ideal ratio, infrastructural requirements equipped with audio-visual aids for conducting simultaneous small group activities for batches ranging from 10- 25 (for medical colleges having intake of 100 to 250 MBBS students) has become the piped dream. The newer elements in specific require meticulous planning ahead to implement them effectively. Foundation course has seen topics that are out of the comfort zone of faculties who have to learn, unlearn, and relearn, to effectuate them.
Conducting a three-hour early clinical exposure by the preclinical faculty, and assessing the learning of students contextual experience, has become a sisyphean task. Integrated module seems good on paper but the interdepartmental coordination for this integration seems unfathomable. Learner doctor method of training that has not taken off the runaway in predominant medical colleges due to the ongoing pandemic that hit the medical education at its core. And a futuristic challenge perceived for the electives, would be managing the flow of students by the institutions who are opting for external rotation to other centres placed outside the campus.
The MCI/ NMC has meticulously planned plenty faculty development programmes across the country in the format of ‘train the trainers’ to reduce the uncertainty caused by the revised curricula. They have provided with a number of learning resource materials, well explained modules, online videos etc. to conduct these newer elements of the CBME curriculum. These faculty development programme initiatives till December 2018 across the 10 nodal and 12 regional centres, have conducted 904 pre-revised Basic Course Workshops, 520 revised Basic Course Workshops and 273 workshops on Attitude, Ethics and Communication module. These have begun much before the implementation of the CBME curriculum to equip the educators across the country in this smoother transition.18
The key to organising these elements successfully is advanced organisational designing of these newer elements. An openness to ideas and sharing of action plan amongst various medical institutions, can make these concerted efforts rewarding. Incentivisation of faculty, who strive to make the cut through educational innovations and scholarships should be promoted with accolades and awards in educational excellence at national level. These motivate development of an educational culture of ingenuity, creativity and dynamism amongst the medical fraternity, that would drive home the must desired change.
Educational leaderships at the medical institutions of the country should embrace the transition, and instil amongst their faculty in a top-down approach, a sense of pride to witness and be a part of this revolution. The curricular governance team at the institutions should play the pivotal role in coordinating amongst the various committees to plan the timely implementation of these elements.
Educational scholarships of quite a few studies, depict that these elements have been successfully implemented at their institutions acting as a platform on which future research in this area can be conducted. The foundation course have been received well amongst faculty and students across the country. The key factors that have help in successful implementation of the foundation program are good collaboration, planning, and pioneering the change by the faculty. 19, 20 A comparative study done to establish the efficacy of organisation of the ECE sessions in the hospital or community settings corroborated that both were able to supplement the classroom teaching effectively and positively impacted the perceived medical training, demonstrating high satisfaction amongst faculty and students.21 Another study which started an integrated learning program for the phase I students, in neurosciences sessions, found student satisfaction from such a program amounting to 60% — 80% (Likert scale of good and excellent). Though they concurred that the majority students also felt that these interventions will help them in the clinical years but not in the summative examinations of the first year.22
The CBME has opened new arenas for the educators in India to explore the plethora of qualitative and quantitative research opportunities, which will inform us about the proper evaluation of these newer elements. As is said, that ‘Rome was not built in a day..’, the implementation of these elements should be considered a dynamic ongoing process of improvisation. This study is a step forward in this direction. It gives essential insights into the implementation of these newer elements as an extrapolation from the guideline platform laid down by the NMC. The modules and session plans shared in this work can be used by all to adapt into their curriculum. Creativity and innovation in generating the structured lesson plan for each of these elements, would be the essence to carry forward this work by all the revered medical educators across the country.
Subscribe now for latest articles and news.