Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i2.24.17
Year: 2024, Volume: 10, Issue: 2, Pages: 227-230
Case Report
Apurva Shrivastava1 , B M Soumya2 , H R Chandrashekar3 , Supriya S Nandi1 , P Sameer Ahamed1
1Postgraduate, JJM Medical College, Davangere, Karnataka, India,
2Associate Professor, JJM Medical College, Davangere, Karnataka, India,
3Professor Emeritus, JJM Medical College, Davangere, Karnataka, India
Address for correspondence:
Apurva Shrivastava, Postgraduate, JJM Medical College, Davangere, Karnataka, India.
E-mail: [email protected]
Received Date:23 January 2024, Accepted Date:11 July 2024, Published Date:05 August 2024
This study presents a rare instance of cervical papillary adenofibroma, a benign biphasic neoplasm originating from glandular and fibrous tissue, occurring in a 43-year-old female patient. Most common site is the endometrium. Papillary adenofibroma arising from the cervix is an infrequent entity. Uterine adenofibromas were first described by Ober in 1959 as a form of mixed mesodermal tumor. Cervical adenofibromas was first described by Abell in 1971. Both the stromal and epithelial components are benign. Grossly, adenofibroma present as a papillary, polypoidal or sessile lesion that may protrude into the endocervical canal with cut surface showing multiple cysts imparting it a spongy appearance. Microscopically, they have a nodular surface with a lobulated papillary configuration. The tumor may recur if incompletely excised. Adenosarcoma and adenomyoma are important differential diagnosis. The clinical presentation, diagnostic procedures, gross appearance, microscopic architecture, and management strategies are elucidated in this case report. Emphasizing the significance of accurate diagnosis and tailored treatment, this case report underscores the importance of recognizing and managing such infrequent cervical tumors. Through this case report, our aim is to contribute to the existing medical literature on cervical papillary adenofibromas, shedding light on its clinical characteristics, diagnostic nuances, and management modalities for the benefit of clinicians and researchers encountering similar cases.
Keywords: Adenofibroma, Adenosarcoma, Benign, Cervix, Papillary, Rare
Papillary adenofibromas are infrequent benign biphasic neoplasms composed of mixed epithelial and mesenchymal components. These neoplasms arise commonly from the endometrium 1, 2. Cervical papillary adenofibromas is an exceedingly rare entity. However, they are morphologically like those arising from endometrium 1, 2. Peri- or postmenopausal females are most affected, although it can affect females of any age group 2. Patients mostly commonly present with abnormal uterine bleeding and or post-menopausal bleeding 2. Other less common clinical findings are abdominal pain, abdominal enlargement, or a polypoid tumor projecting from cervix 2. Pathologist’s opinion becomes extremely crucial in such cases as the diagnosis of papillary adenofibroma cannot be made only on clinical grounds.
Uterine adenofibromas were first described by Ober in 1959 as a form of mixed mesodermal tumor. Cervical adenofibromas was first described by Abell in 1971. Both the stromal and epithelial components are benign. Extrauterine sites commonly involved are breast and liver. Although these lesions are histologically benign, they tend to recur post incomplete excision, may locally invade, or involve/ transform to carcinosarcoma or adenocarcinoma 2, 3, 4.
In this case report we emphasize on its rarity and diagnostic challenges encountered in its identification, as it holds implications on the treatment planning and prognosis. A multidisciplinary approach involving gynecologists, pathologists, and radiologists in reaching a conclusive diagnosis and formulating an appropriate therapeutic strategy is of paramount importance.
A 43-year-old- woman, P6 L6 A1, was admitted to the gynecology clinic with the chief complaints of bleeding per vagina for about 3 months. Radiological findings revealed anterior wall sub serosal and intramural uterine fibroids with a bulbous cervix. Laboratory findings revealed moderate anemia. Patient underwent dilatation and curettage, and polypectomy was performed. The specimen was sent for histopathological examination.
Grossly, polypoidal soft tissue masses from cervix, largest soft tissue mass measuring 2.5x2cms and smallest mass measuring 1.5x1cm. External and cut surface of all the masses was grey white to grey brown
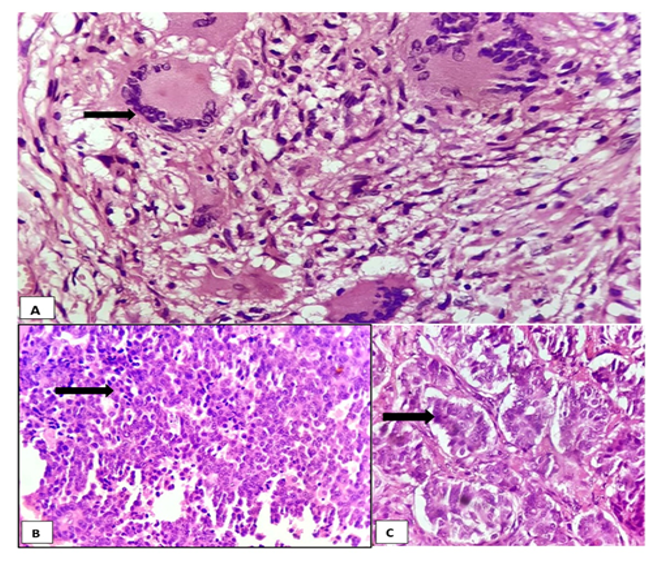
Microscopically, multiple sections studied showed a polypoidal mass composed of mixture of epithelial and stromal components. Epithelial component consists of benign irregular cystically dilated glands lined by endocervical type of epithelium, arranged in papillary growth with cystic spaces. The stroma is cellular and composed of dense fibroconnective tissue with minimal mitotic activity. A final diagnosis of Papillary Adenofibroma of Cervix on histopathological examination was made.



Adenofibroma of cervix is an extremely rare benign mixed mullerian tumor, consisting of both benign epithelium and mesenchymal components. Most commonly it arises from endometrium and only 10% arise from cervix 2, 3, 4.
Grossly, adenofibroma present as a papillary, polypoidal or sessile lesion that may protrude into the endocervical canal 2. In few cases a large adenofibroma may fill the endometrial cavity and enlarge the uterus. Size of these lesions may exceed 5 cm in diameter, can vary in size from 0.5 to 14 cm in dimension mimicking malignancy on clinical examination 2, 3. They are usually firm, rubbery, tan-brown, with punctate areas of hemorrhage noted on the cut surface. The presence of multi cystic appearance on multiple cut sections imparts a spongy or mucoid appearance to the tumor. Most lesions are superficial rarely invade the underlying stroma 2, 5, 6, 7.
Microscopically, they have a nodular surface with a lobulated papillary configuration. Broad, fibrous, relatively cellular fronds are formed. The surface is covered by flattened, nonspecific cuboidal epithelium that is rarely proliferative. Papillae can also be lined by columnar, mucinous, or ciliated glandular epithelium. Columnar mucinous cells and squamous differentiation occur focally in some tumors. The nuclei of the stromal cells are small, uniform, and bland. Mitotic activity is minimal or absent. Increased cellularity around entrapped glands are typically absent 2, 5, 6, 7.
Transvaginal color doppler ultrasonography delineates the lesion as a protruding polypoidal mass containing variably sized multi cystic components without pulsatile blood flow. In magnetic resonance imaging (MRI), sagittal T2-weighted images (T2WI) delineates the tumor and shows punctate heterogenous hyperintensity or islands of isointense-to-hypointense signals. Axial T1-wighted images (T1WI) outlines the tumor as hypointense signal with focal areas of high signal intensity with or without hemorrhagic foci. Contrast enhanced (T1WI) may show minimal tumor enhancement. Hysterofiberscopy shows a polypoidal red-yellow-white tumor protruding from endometrial cavity or cervix with a partially reticulated surface. Contrast-enhanced computed tomography (CT) demonstrates heterogenous low-attenuating multi cystic mass protruding from the endometrial cavity or cervix 8.
Adenosarcoma and adenomyoma are important differential diagnosis 7, 8. The hypercellular peri glandular stroma/typical mesenchymal cell peri glandular cuffing specific for adenosarcoma is absent in adenofibromas. Stromal cell atypia is absent or mild and markedly atypical mesenchymal cells are absent in adenofibromas. Histologically malignant heterologous elements, and myometrial invasion, are not present in adenofibromas. Mitotic figures are absent or rarely present 7, 8, 9. Adenosarcoma is diagnosed if stroma shows atypia, increased peri glandular stromal cells, invasiveness, and mitotic figures > 4/10 high power fields, wherein the histopathological morphology of adenomyoma is characterized by the tumor stroma being smooth muscle. Cervical adenofibroma and adenosarcoma share very similar histomorphology and the two differ mainly in the stromal component making a close confounder 7, 8, 10, 11. Compared to typical cervical polyps, stromal component of adenofibromas tends to be more fibrous and uniform than the stroma of a typical polyps. Histopathological morphology of cervical polyps is characterized by glands that have mucinous columnar epithelium with loose edematous stroma 7, 8, 9, 10, 11.
Adenofibromas have been associated with endometriosis, and some authors believe they represent a form of endometriosis with extreme smooth muscle metaplasia that is, endomyometriosis. Another differential to be kept in mind is carcinosarcoma. The pathological features of carcinosarcoma are malignant epithelium and malignant mesenchymal tissue 7, 8, 9, 10, 11.
Although adenofibroma is a benign tumor, it has been shown to invade the myometrium and pelvic veins, relapse and even metastasize. Local excision is curative, but the tumor may recur if incompletely excised. Hysterectomy is the preferred treatment, as adenofibromas may recur if incompletely curetted or excised. Wide excision via trachelectomy is an alternative treatment for cervical adenofibromas if fertility is desired, or if hysterectomy is contraindicated. Hysterectomy permits thorough sampling needed to exclude an adenosarcoma and ensures complete removal 7, 8, 9, 12.
Adenofibromas should be considered as a differential diagnosis of a patient with a cervical mass and abnormal vaginal bleeding without clinical evidence of malignancy 11. Although preoperative diagnosis using USG, MRI, CT, hysterofiberscopy and relevant clinical details can give a clue to diagnosis, but detailed histopathological study is required for a definitive diagnosis and to differentiate adenofibromas from adenosarcoma 11, 12, 13.
Subscribe now for latest articles and news.