Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2017.v03i03.008
Year: 2017, Volume: 3, Issue: 3, Pages: 39-42
Case Report
Ashwini Bakde Umredkar1, Prajwalit Gaur2, Aarti Anand3, Sindhu Ganvir4, Mohsin Ansari5
1Associate Professor, Department of Radio Diagnosis, Government Medical College and Hospital,Nagpur, Maharashtra, India,
2Professor, Department of Radio Diagnosis, Government Medical College andHospital, Nagpur, Maharashtra, India,
3Professor, Department of Radio Diagnosis, Government Medical Collegeand Hospital, Nagpur, Maharashtra, India,
4Professor and Head, Department of Oral Pathology and Microbiology,Government Dental College and Hospital, Nagpur, Maharashtra, India,
5Post Graduate Resident, Department of Radio Diagnosis, Government Medical College and Hospital, Nagpur, Maharashtra, India
Address for correspondence:
Dr. Ashwini Bakde Umredkar, Department of Radio Diagnosis, Government Medical College and Hospital, Nagpur, Maharashtra, India 303, Plot No. 150/a, Prajakta Orchid Apartment, Pandey Layout, Nagpur, Maharashtra, India.
E-mail: [email protected]
Dentigerous cysts, also known as follicular cyst, are the most common developmental cysts of the jaws. It is the cystic degeneration of the enamel organ after the formation of tooth but before its eruption. Hence, it is frequently associated with crown of impacted tooth. Dentigerous cysts are the second most common odontogenic cyst and the most common developmental odontogenic cyst. We report a case of dentigerous cyst with angiomatous changes in an 11-year-old male. The patient complained of swelling in the upper left buccal region. Radiographically well-defined cystic lesion was noted in relation to a left impacted molar tooth. In this report, we discuss the radiological findings including the embolization of the vascular component which was very helpful in the surgical management of the patient. The cyst was enucleated with the removal of the impacted tooth. Histopathological examination confirmed the diagnosis of dentigerous cyst associated with angiomatous changes possibly revealing the process of angiomatous transformation. The patient remained asymptomatic, and no complications were noted.
KEY WORDS:Ameloblastoma, dentigerous cyst, impacted tooth.
Dentigerous cysts are the most common developmental odontogenic cysts, accounting for approximately 25% of all odontogenic cysts of the jaws. They are frequently noted as an incidental finding on radiographs because a majority of these cysts are asymptomatic and are most commonly associated with impacted mandibular third molars and permanent maxillary canines.[1,2] A dentigerous cyst presents as a well-defined radiolucent entity surrounding the crown of an impacted tooth. The border of the cyst is continuous with the cementoenamel junction of the impacted tooth.[3,4] This radiographic finding is pathognomonic for a dentigerous cyst. The occurrence of dentigerous cysts encompassing multiple teeth is uncommon. All of the reported cases to date have involved cysts localized to one quadrant of the jaws and have
encompassed adjacent teeth. As a dentigerous cyst enlarges, it displaces the affected tooth or teeth apically. Dentigerous cysts enlarge as a result of the accumulation of fluid between the crown of an unerupted tooth and the reduced enamel epithelium.
An 11-year-1-month-old male presented with swelling in the upper left buccal region for 3 months to the department of oral medicine and radiology.
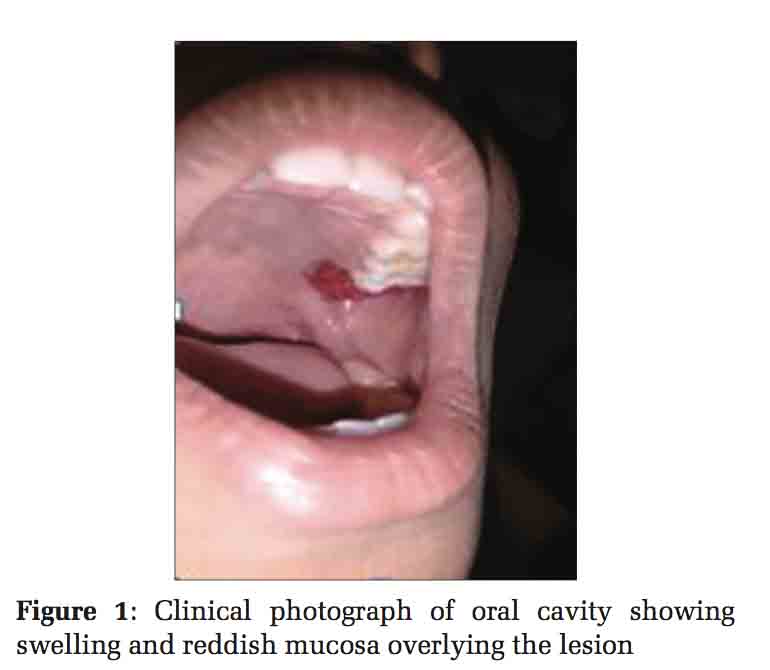
On oral examination, a solitary diffuse 2 cm × 2 cm intraoral swelling was seen in the left upper buccal region in the oral cavity, not bleeding on touch. The swelling was roughly oval in shape. The swelling was tender on palpation and fluctuant inconsistency. The overlying mucosa was reddish in color [Figure 1], and the superficial blood vessels were prominent.
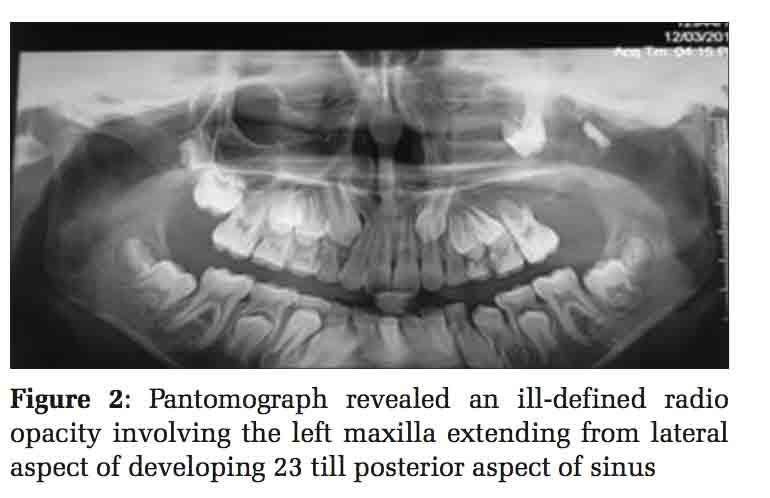
A panoramic radiograph [Figure2] was advised. The pantomograph revealed an ill-defined radio- opacity involving the left maxilla extending from lateral aspect of developing 23 till posterior aspect of sinus. Superoinferiorly, it is extending from alveolar crest till infraorbital rim. Superior displacement of developing 27 and 28 is noted.
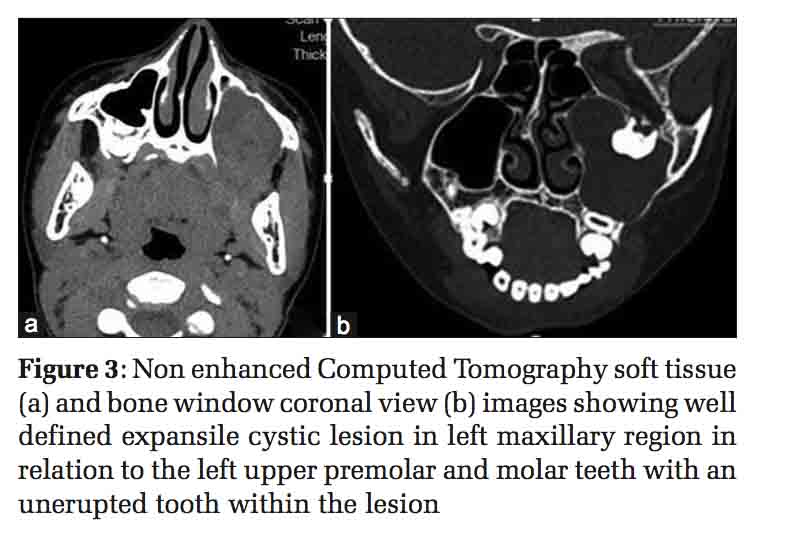
Further, contrast-enhanced computed tomography (CECT) was advised to know the extent of lesion and for further characterization which was performed on a multi-detector row computed tomography (CT) scanner (Brilliance ICT 256, Philips Medical Systems, Best, The Netherlands) with multiplanar reconstruction. The axial [Figure 3a] and coronal [Figure 3b] images revealed that the cyst was larger than was apparent on the digital pantomograph. CECT Figure 4 shows well- defined expansile unilocular cystic lesion in the left maxilla of approximate size 2.8 cm × 4.9 cm × 4.0 cm in transverse, anteroposterior, and craniocaudal axis, respectively, noted in relation to upper premolar and molar tooth on the left side.
There is unerupted molar tooth noted within the cystic lesion and non-enhancing hypodense collection within of average attenuation 16HU.
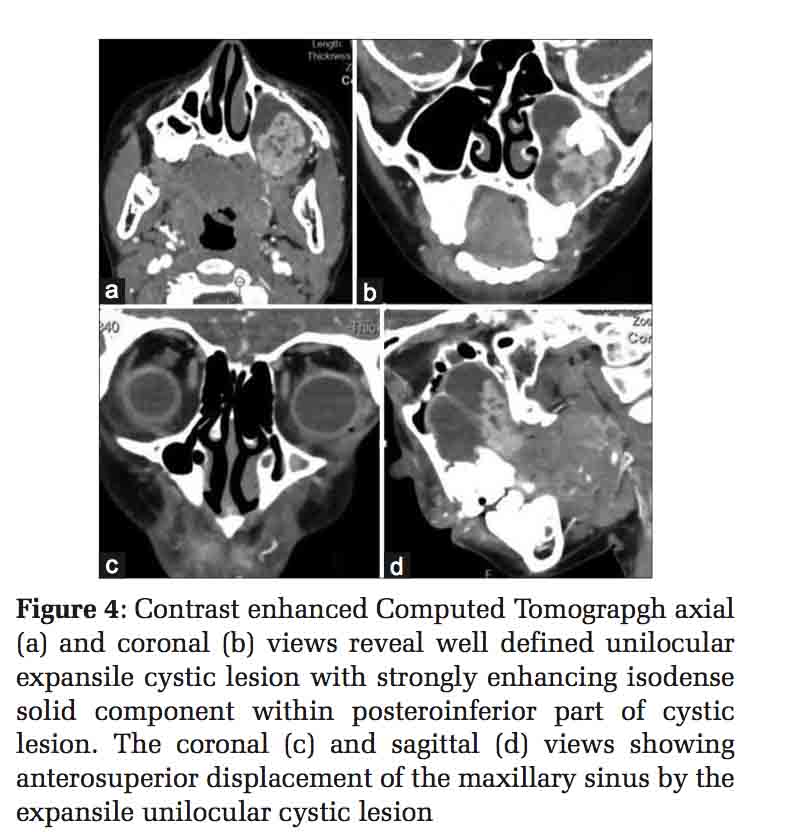
There is strongly enhancing isodense solid component within posteroinferior part of cystic lesion with extension of solid component into the gingivobuccal sulcus and abutting the left medial pterygoid muscle through cortical breech in inferior part of cystic lesion [Figure 4a and d].
The left maxillary sinus was displaced and compressed anterosuperiorly [Figure 4c and d].
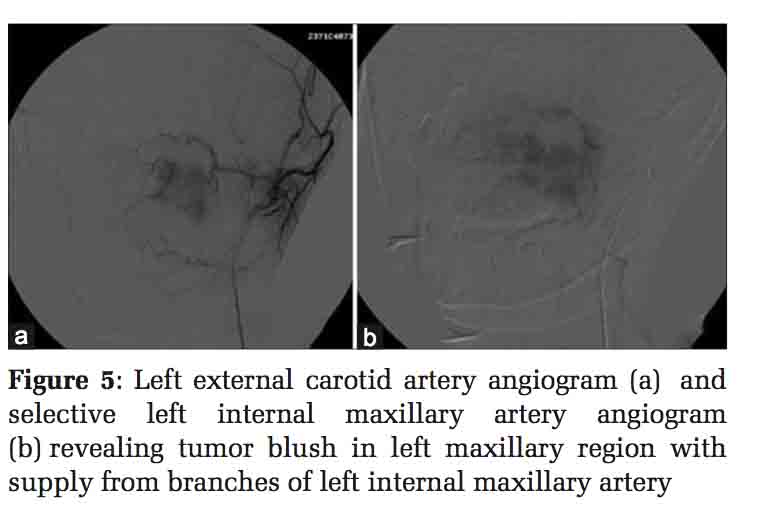
In view of the vascular component, the patient was referred to interventional radiology for pre-operative embolization by the department of oral and maxillofacial surgery. Digital subtraction angiography was performed through the right femoral approach using Terumo guide wire, 4F H1 catheter, and Progreat microcatheter. The left carotid artery angiogram was done. Vascular solid component was supplied by the left maxillary artery revealed as an abnormal vascular blush from terminal internal maxillary arterial (IMA) branches on the left external carotid angiogram [Figure 5a].
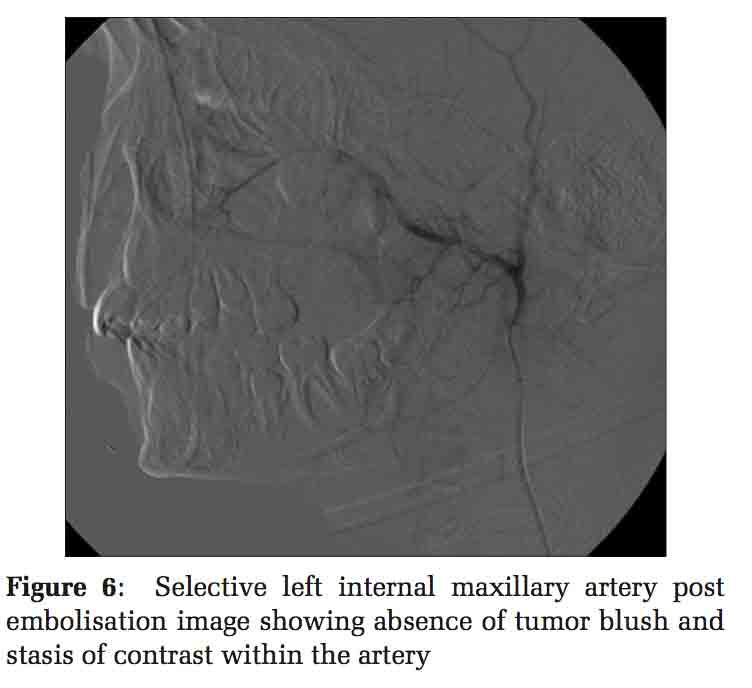
Selective left IMA angiogram [Figure 5b] revealed tumor blush. Superselective embolization of the left IMA arterial branches supplying the tumor mass done using 8–10 ml of 100–200 microns and 300–500 PVA particles. Post-embolization external carotid artery angiogram Figure 6 showing complete absence of tumor blush with contrast stasis in IMA.
Patient then underwent resection (enucleation) and curettage [Figure 7].
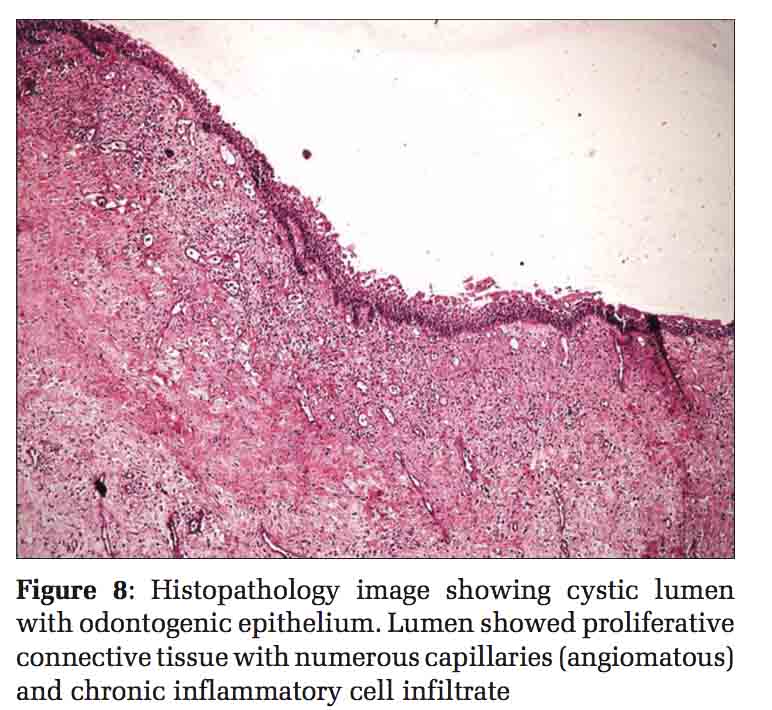
On histopathology, the lesion demonstrated cystic lumen with odontogenic epithelium. Lumen showed proliferative connective tissue with numerous capillaries (angiomatous) and chronic inflammatory cell infiltrate which is s/o organization of proliferative cystic epithelium. Final histopathological diagnosis was dentigerous cyst with angiomatous change [Figure8]. Such changes can finally undergo malignant ameloblastomatous transformation, so the patient was kept on follow up. Ethical clearance was obtained from the Ethical Committee.
The patients with dentigerous cyst can be asymptomatic, or when symptomatic the most common clinical presentation is the cheek pain or swelling.[5] On clinical examination, the finding of unerupted tooth may be the only presentation of dentigerous cyst. It has to be investigated through different imaging modalities. Early diagnosis and ability to differentiate developmental cyst from inflammatory cyst is crucial in pediatric patients for subsequent treatment planning to reduce potential morbidity. Dentigerous cyst with angiomatous changes is quite rare.
In our case, the imaging features on radiography
were suggestive of a well-defined cystic lesion in relation to an impacted tooth. Hence, the differential diagnosis included odontogenic tumors such as odontogenic keratocyst and dentigerous cyst. However, the imaging features like vascular solid component and extension into the adjacent soft tissue on computed tomography made us think about the aggressive tumor-like unilocular ameloblastoma with mural nodule.
Odontogenic keratocyst is usually located within the jaw that is they are intraosseous benign tumors originating from the dental lamina containing cheesy material.[6] They are periapical in location. They can cause root resorption and show peripheral daughter cyst on imaging.
Dentigerous cyst is avascular, unilocular cyst noted in relation to the crown of an impacted tooth. On attaining large size, they displace the normal tooth. Large dentigerous cyst can rarely undergo malignant transformation into the unilocular mural ameloblastoma.[7,8]
Ameloblastomas are slow growing, locally aggressive, and infiltrative benign tumors. They most commonly present in age group between 20 and 40 years. They may be unicystic, desmoplastic, and mixed solid cystic types.[9]
Thus, the patient had mixed imaging features of dentigerous cyst and ameloblastoma. On histopathology, our case is consistent with dentigerous cysts with angiomatous change. There can be coexistence of these changes as there can be ameloblastic transformation of dentigerous cyst. Angiomatous changes can be a process toward malignant transformation which is rarely observed. 15–20% of all unicystic ameloblastomas are known to form in the wall of dentigerous cysts.[10,11]
In summary, though the radiological features help us to narrow the differential diagnosis of an odontogenic lesion, the diagnosis mostly depends on the histopathologic evaluation. In our case, CT imaging findings proved to be of utmost importance than conventional radiographic evaluation to the maxillofacial surgeons which nicely depicted the vascular component. Hence, all the odontogenic cysts should undergo a CECT study before surgery and embolization in case of vascular component to reduce blood loss intraoperatively.
At follow-up examinations, the patient had no complications. Finally, all dentigerous cysts should be followed up as all dentigerous cysts have the potential risk of developing ameloblastoma.

Radiology plays an important role in diagnosis of dentigerous cyst. Radiologically, they are simple cystic lesion, but whenever one encounters cystic lesion with enhancing mural nodule with impacted tooth a possibility of ameloblastic transformation needs consideration and confirmation on histopathology.
Subscribe now for latest articles and news.