Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i3.25.92
Year: 2025, Volume: 11, Issue: 3, Pages: 263-267
Original Article
Teena Jasmin D’Souza1 , Kavitha Prabhu2 , Prasanna N Bhat3 , Ganesh Nayak S4
1BSc MLT Intern, FMAHS, Mangaluru, Karnataka, India,
2Assistant Professor, Department of Microbiology, Father Muller Medical College, Mangaluru, Karnataka, India,
3Associate Professor, Department of Microbiology, Father Muller Medical College, Mangaluru, Karnataka, India,
4Associate Professor, Department of General Medicine, Father Muller Medical College, Mangaluru, Karnataka, India
Address for correspondence: Kavitha Prabhu, Assistant Professor, Department of Microbiology, Father Muller Medical College, Mangaluru, Karnataka, India.
E-mail: [email protected]
Received Date:26 February 2025, Accepted Date:07 June 2025, Published Date:20 October 2025
Background: Dengue (DEN) is the most significant emerging tropical illness in the world. Dengue infection presentation varies from as a mild self-limiting disease to more fatal hemorrhagic complications. This study was undertaken to estimate the prevalence percentage of dengue infection in patients admitted with dengue like illness in a tertiary care hospital in south India and to see their clinical, demographic and microbiological characteristics.
Methods: Blood samples received in the microbiology laboratory from May2024 to November2024 for Dengue specific ELISA and Dengue rapid testing were included in the study. Detection of NS1/ IgM/IgG were taken as confirmed cases. Demographic, clinical, laboratory and microbiological parameters were retrieved from medical records and recorded in an Excel sheet and analyzed using SPSS V 23.
Results: Overall, 723 inpatient samples came positive for dengue either by rapid test or ELISA or both (723/3739,19.33%). Fever < 5 days was the most frequent symptom. Thrombocytopenia was seen in 54.91% of patients. The mean age of dengue patients was 39.34 years with male preponderance (55.3%). Raised AST level was seen in 66.1% of cases with median =89(IQR12-10084) and raised ALT in 54.5%, with median = 56.5(IQR 10-6737). Out of total dengue positive cases, 67.7 % had high ferritin level with median = 889.0(IQR 00-9790)).
Conclusions: High suspicion with prompt investigations needed due to varied presentation of dengue. Recognizing and monitoring the warning signs and laboratory changes in a dengue positive patient can help in effective management and thus reducing mortality rate.
Keywords
Dengue, RDT, Dengue specific ELISA, Thrombocytopenia, Ferritin level
Dengue fever is caused by four distinct but antigenically related serotypes of dengue viruses. Dengue viruses belong to flaviviridae which is seen in tropics and sub tropics, transmitted by mosquito bite principally Aedes aegypti and Aedes albopictus. 1 According to World Health Organization estimates about 50- 80 million cases of dengue fever occur worldwide every year. 2
Primary dengue infection is characterized by mild to high grade fever lasting for 3 to 7 days, severe headache with pain behind the eyes, muscle and joint pain, rash and vomiting which is a self-limiting disease. 2 Secondary infections are the more frequent form of the disease in many parts of Southeast Asia and South America. Secondary dengue infection is due to infection with another serotype which is different from the first serotype. 3 This form of the disease is more serious, most often caused by dengue serotype 2 or 3 and can result in severe dengue infection with complications due to severe plasma leakage, severe bleeding and severe organ involvement. 3 Usually, there will be warning signs before the manifestations of shock and appear towards the end of the febrile phase, between days 3–7 of illness. Abdominal pain and persistent vomiting with rapid decrease in platelet count are the early indication of plasma leakage. 2 These symptoms persist and may become worse and along with hepatomegaly and hemorrhagic manifestations, patient can progress into the state of shock. 2, 3
Laboratory diagnosis of dengue infection is by polymerase chain reaction techniques Real-time reverse transcriptase-polymerase chain reaction (RT-PCR) or antigen detection (Enzyme linked immuno sorbent assay, ELISA or Rapid diagnostic test, RDT) if the infection is less than 5 days’ duration. There will be a rise in dengue-specific IgM antibody within 4–5 days of fever onset, followed by rise of IgG antibody with 7–10 days. Secondary infection is characterized by an early rise in the IgG antibody titer and a lower titer of IgM rise. Dengue specific IgM or IgG are detected by ELISA, or RDTs. Again, early phases of secondary dengue also show PCR and NS1 positivity. 4 With this background, this study was undertaken to estimate the percentage prevalence of dengue infection in patients admitted in tertiary care hospital in South India and to see their clinical, demographic and microbiological features.
An ambispective observational study was conducted for a period of 7 months from May2024 to November2024 in our tertiary care hospital after obtaining approval from the ethics committee (711/2024, 13/08/2024).
Inclusion criteria: Samples received from all clinically suspected dengue patients admitted in the hospital.
Exclusion criteria: Samples which have come positive for anti-lepto antibodies, WIDAL and Weil-Felix and clinically correlating with other disease conditions.
Sample size calculation: The sample size was calculated based on the study conducted by Teena Damodar et al.,5 in which the prevalence of dengue was 29 % (P). Considering a 95% confidence interval and 5% allowable error (e), the sample size was estimated using the formula n = (Z2α/2pq)/d2 = (1.96*1.96) *29*71/5*5 = 316.
Method: Blood (serum) samples received in the microbiology laboratory for Dengue specific ELISA was done by using Panbio™ Dengue IgM Capture ELISA, Panbio™ Dengue IgG Capture ELISA kit and blood samples received for Dengue rapid test was done by using Dengue Day 1 Test (J. mitra & co. PVT. LTD) for the detection of dengue NS1 antigen, IgM and IgG antibodies in human serum. Both the tests were performed and interpreted according to manufacturer’s instructions. All seropositive cases for dengue with NS1/IgM/IgG were listed and further details like demographic, clinical, laboratory and microbiological parameters were retrieved from medical records and recorded in an Excel sheet.
Statistical analysis: IBM SPSS Statistics V.23 was used for statistical analysis. The variables like demographic, and microbiological variables were analyzed and expressed in terms of frequencies and percentages. Continuous variables were expressed in terms of the median. The test of normality was done by the kolmogorov smirnov test.
During the study period, 3739 samples received from clinically suspected dengue inpatients in the hospital. Among them 3365 samples from were received only for dengue rapid diagnostic test and 96 samples for only dengue specific IgM/ IgG ELISA. For 278 samples, both RDT and ELISA were requested. Overall, 723 inpatient samples came positive for dengue by either by RDT/ELISA or both (723/3739,19.33%). On rapid diagnostic kit, majority were NS1 + positive (59.4%) followed by NS1+IgM (20.12%). In ELISA method, IgM alone was detected in 49/84 positive cases (58.3%) and in 35 samples (41.6%) both IgM and IgG were detected (Table 1).
|
Test method |
Serological marker |
Number / percentage |
Total / percentage |
|
Rapid diagnostic method |
NS1 positive |
393(59.4) |
661(18.14%) |
|
NS1+IgM |
133(20.12) |
||
|
IgM |
121(18.30) |
||
|
IgM + IgG |
11(1.66) |
||
|
NS1+ IgM+ IgG |
03(0.45) |
||
|
NS1+IgG |
NIL (0) |
||
|
ELISA method |
IgM |
49(58.3) |
84(22.45%) |
|
IgM + IgG |
35(40.22) |
About 25 samples were positive by both RDT and ELISA method. Sixteen samples were positive only for IgG, so they were considered as past infection and excluded from the study. Eight samples were borderline, and they were excluded from the study as doubtful cases.
The common age group affected by dengue was 20-30 years followed by 40-50years (Figure 1).
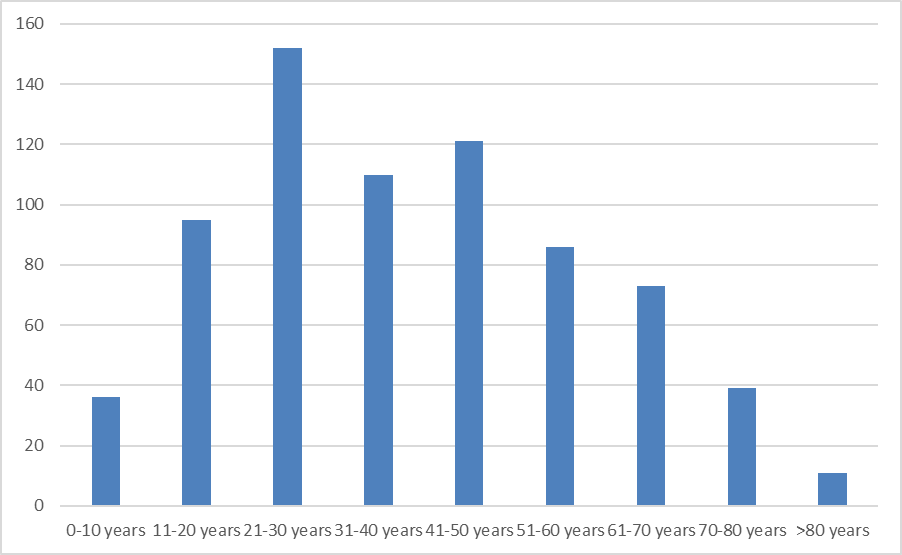
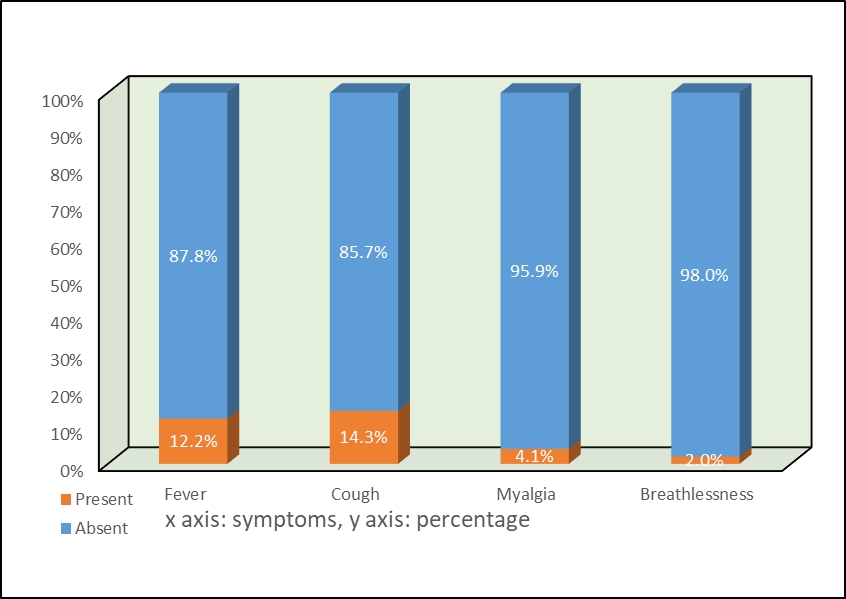
Mean age of dengue affected cases was 39.34 years. Males were commonly affected than females (55.5% verses 44.5%). Major symptom of dengue positive patients was fever < 5 days (52.6%). Other common clinical symptoms were myalgia (37.2%), headache (34.4%) and vomiting (33.3%). Skin rash was seen only in 2.8% cases (Table 2). Thrombocytopenia (platelet count<1 lakh/mm3) was seen in 397 patients (54.91%) with median=90,000 (IQR 6000-135000) (Table 2, Table 3).
|
Clinical presentation |
Frequency (%) in total dengue cases (n=723) |
|
Fever (3-5 days) |
380 (52.6) |
|
Fever (5-7 days) |
255 (35.3) |
|
Myalgia |
269 (37.2) |
|
Arthralgia |
23 (3.2) |
|
Headache |
249 (34.4) |
|
Chills |
184 (25.4) |
|
Nausea |
108 (14.9) |
|
Vomiting |
241(33.3) |
|
Skin rash |
20 (2.8) |
|
Abdominal pain |
120 (16.6) |
|
Hepatomegaly |
54 (7.5) |
|
Encephalitis |
11(1.5) |
|
Restlessness |
6 (0.8) |
|
Laboratory (Haematological and liver) parameters |
|
|
Platelet count (10000-100000)/mm3 |
390(54.5) |
|
Platelet count<10000/ mm3 |
7(1.0) |
|
Serum AST>59 IU/L |
434(66.1%) |
|
Serum ALT>50 IU/L |
374(54.5) |
|
Serum Ferritin>464 IU/L |
317(67.7) |
Raised AST level was seen in 66.1% of cases with median = 89(IQR12-10084) and raised ALT in 54.5%, with median = 56.5(IQR 10-6737). Out of total dengue positive cases, 67.7 % had high ferritin level with median = 889.0(IQR 00-9790)). Median value of packed cell volume observed among dengue positive cases was 39.30% (Table 3).
|
Laboratory data |
Mean ± SD |
Median (IQR) |
Significance (P) |
|
Platelet count |
115935.4749 ± 105152.28822 |
90,000 (6000 - 135000) |
0.000 |
|
PCV |
39.1965 ± 9.70994 |
39.30 (13 - 224) |
0.000 |
|
Serum AST level |
192.7443 ± 564.54701 |
89.0 (12 - 10084) |
0.000 |
|
Serum ALT level |
132.3367 ± 405.60131 |
56.5 (10 - 6737) |
0.000 |
|
Serum Ferritin level |
1605.2305 ± 1930.4835 |
889.0 (00-9790) |
0.000 |
The test of normality was done by Shapiro-Wilk method.
Dengue is an emerging vector born disease. We are seeing an increase in number of cases year by year in our country as well as in our city. In our study, we found sero-positivity of 19.33% in clinically suspected dengue cases which is less compared to a previous study conducted in the same center 8 years back, in which they found 29% sero-positivity. 5 This could be due to increased awareness among people and taking more precautionary measures for controlling of mosquitoes and avoiding mosquito bites. The common age group affected by dengue in our study was between 20 and 50 years with male predominance (55.4%) (Figure 1) which is similar to the previous studies conducted in south India. 5, 6 Male predominance could be due to the risk of exposure to the mosquitoes while working outdoors. Our study found that fever (87.8%) was most commonly presenting symptom followed by headache (34.4%) and myalgia (37.2%) (Table 2) similar to other studies. 6, 7, 8 Abdominal pain and vomiting were observed in 16.6% and 33.4% of cases (Table 2), respectively, which is concordant to the study of Manjunath et al. 7 Additionally, we observed that 1.5% of cases had encephalitis and 7.5% hepatomegaly (Table 2). In 2.8% of our cases, skin rashes were seen contrary to 0.5% (Table 2) in Mohan et al. 6
Most of our cases detected by RDT (59.4%) (Table 1) were identified only by presence of viral NS1 antigen in patient sera compared to IgM antibodies (18.30%). These observations were similar to a study conducted previously by Tina Damodar et al in which they found that (40%) were detected exclusively by the presence of viral NS1 antigen compared to IgM (7%) antibodies in patient’s sera. 5 Contrary to our study, in a study conducted by Islam et al. 8, NS1 was detected in 95.9% of cases, perhaps due to the early presentation of patients to the hospital. If we take an account of ELISA, out of 87/374 (Table 1) patients tested positive for dengue. Out of them 49 were positive for only IgM and rest 35 were positive for both IgM & IgG. We observed that in our hospital, the first test requested on suspicion of dengue was rapid dengue test and if it comes negative in a highly suspected case, then only ELISA was done. This could be due to the high cost of ELISA compared to RDT. Laboratory diagnosis and case confirmation of early of DEN cases are reportedly enhanced by the using the NS1 assay. 9 As our study also showed, NS1 antigen testing is much more sensitive and especially helpful during for the detection of early phase of dengue.
Varying degree of abnormal hematological/liver parameters (Table 3) were observed in dengue positive cases. Thrombocytopenia (<100000/mm3) was observed in 54.5% of dengue cases with < 10,000/mm3 in 1% of cases. We noticed that elevation of liver enzymes with AST being significantly higher than ALT, raised AST is seen in 66%and raised ALT in 54.5% of infection. This abnormality could be taken as an early indicator of complication in the diagnosis of dengue infection. As per the previous study by Swamy am et al, the broad spectrum of hepatic dysfunction in dengue varies from asymptomatic elevation of the transaminases to fatal fulminant hepatic failure. 10 In their study 74.2% of patients had elevated transaminases. AST was elevated in 73.3% of the patients and ALT in 50.8% of the patients, which was comparable to our findings. The highest AST value found in their study population was 4942 IU/L which was more than 100 times the normal limit, while the highest ALT value in our study was 1306 IU/L which was nearly 30 times the upper limit.
The serum ferritin levels significantly increased (Table 3) in positive dengue cases with complications. Out of 723 dengue cases 13 patients’ serum ferritin value was >10000 ng/ml with a mean of 1605.23 ng/ml. Common clinical presentations of these patients with high ferritin were altered sensorium and seizure. Petchiappan et al noted higher ferritin levels on day 4 onward during the febrile phase of illness in severe dengue patients than non-severe dengue cases. 11 Study by Suresh et al analyzed serum ferritin levels both during febrile and defervescence, or convalescent phase, which is critical as the disease progression to severe dengue occurs after the febrile phase and demonstrated that an increase in ferritin levels as the severity grade increases. 12
Out of 723 positive cases 78 patients had been admitted to ICU for further management. Among them 15 patients (2.07%) expired. Patients admitted in ICU presented with severe thrombocytopenia, diffuse cerebral edema, seizures, bilateral mild pleural effusion, hepatic encephalopathy in patients with underlying chronic liver disease. In a study conducted by Suresh et al, the major causes for the ICU admissions were life-threatening bleeding manifestations, severe thrombocytopenia with or without bleeding manifestation, systemic inflammatory response syndrome, DSS, acute respiratory distress syndrome, CNS impairment, and shock with pre-renal failure. 12
There were few limitations of the study. The study was observational and dengue serotypes and type of infection, whether primary or secondary were not looked for. Also, other health conditions, nutritional status and co-infections were not considered into account which can affect the laboratory parameters as well.
Our study showed the importance of early detection of dengue infection by performing NS1 RDT and IgM/IgG ELISA. Thrombocytopenia, raised ALT, AST and serum ferritin level were observed in dengue positive cases presented with complications. High suspicion with prompt investigations needed due to varied presentation of dengue. Recognizing and monitoring the warning signs and laboratory changes in a dengue positive patient can help in effective management and thus reducing mortality rate.
Funding: None
Conflict of Interest: None
Subscribe now for latest articles and news.