Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i1.24.349
Year: 2025, Volume: 11, Issue: 1, Pages: 91-97
Original Article
G M Krithika1 , A S Sanjana2
1Final year post graduate, Department of Dermatology, Venereology and Leprosy, BGS GIMS, Bangalore, Karnataka, India,
2Professor and HOD, Department of Dermatology, Venereology and Leprosy, BGS GIMS, Bangalore, Karnataka, India
Address for correspondence:
G M Krithika, Final year post graduate, Department of Dermatology, Venereology and Leprosy, BGS GIMS, Bangalore, Karnataka, India.
E-mail: [email protected]
Received Date:06 November 2024, Accepted Date:08 February 2025, Published Date:08 February 2025
Introduction: Acne vulgaris is a common dermatological condition which often leads to scars. The treatment of acne scars typically involves a multi-faceted approach, with microneedling and PRP therapy emerging as effective options for atrophic scars. While several studies have compared the effects of microneedling alone versus microneedling combined with PRP, there is a lack of direct comparison between the individual efficacy of microneedling and PRP. This study aimed to address that gap. Objectives: To compare the efficacy of dermaroller versus PRP therapy in the same patient with acne scars. Materials and methods: A total of 25 patients were included in the study. Goodman and Baron quantitative acne scar grading system was employed for classification. Patients were treated with dermaroller on right side of face and intradermal PRP injections on left side of face. Response was assessed at 1, 2, 3, and 4 months using a visual analog score (VAS). Results: The mean (SD) age of the study participants was 29.8 (5.2) years. Out of 25 patients, 52% (n=13) were males and 48% (n=12) were females. At the end of 4 sessions of microneedling on right cheek, 92% (n=23) had fair response and 8% (n=2) had poor response, whereas on left cheek, 80% (n=20) had good response and 20% (n=5) had excellent response post PRP and this difference was significantly different (p <0.001). Conclusion: Platelet-rich plasma (PRP) yields superior outcomes compared to microneedling in improving atrophic acne scars.Top of Form
Keywords: Acne scars, Platelet rich plasma, Microneedling
Acne vulgaris is a common dermatological condition which often leads to scars 1, 2, 3. Facial scars affect both sexes equally and are seen in 90% of patients with acne 4. Different types of acne scars include ice pick scars, rolling scars, boxcar scars, papular scars, atrophic scars, hypertrophic or keloidal scars. Severe post acne scarring can cause considerable psychological distress, mainly among adolescents 5, 6, 7.
The treatment of acne scars typically involves a multi-faceted approach, with microneedling and PRP therapy emerging as effective options for atrophic scars.
Microneedling, which is done using dermaroller, is an efficacious procedure which causes collagen induction and creates minute inlets for effective absorption of topical agents 8.
PRP serves as rich source of autologous growth factors like epidermal growth factor, transforming growth factor beta, platelet-derived growth factor, and vascular endothelial growth factor and enhances the wound-healing response 9, 10.
While several studies have compared the effects of microneedling alone versus microneedling combined with PRP, there is a lack of direct comparison between the individual efficacy of microneedling and
The present study was to compare the efficacy of dermaroller versus PRP in patients with acne scars.
To compare the efficacy of dermaroller versus PRP therapy in the same patient with acne scars.
Evaluate the effectiveness of dermaroller and PRP therapy in treating acne scars in the same group of patients.
Assess the improvement in acne scars using a standardized scar assessment scale (e.g., the Global Acne Scar Grading System) before and after treatment.
Conduct the comparison within a defined patient group who meet the inclusion criteria (e.g., age, severity of acne scars).
Provide valuable insight into which treatment modality (dermaroller or PRP) is more effective for acne scar improvement.
Complete the comparison within a 6-month period, with measurements taken before treatment, after each session, and at follow-up.
After obtaining clearance from institutional ethical committee (ethical committee clearance number: BGSGIMS/IEC/App/Mar/2023/02 - 30th March 2023), a total of 25 patients were included in the study. Proper counselling was done, and detailed clinical findings were recorded. CBC, serology and coagulation profile were done. Clinical photographs were taken.
The inclusion criteria included cases with atrophic acne scars belonging to the age group of 18–40 years.
The exclusion criteria included active acne, history of keloid, bleeding disorders, patients with unrealistic expectations.
We employed the Goodman and Baron quantitative acne scar grading system for classification.11 This system evaluates scars based on lesion count and severity. Lesion counting assigns 1 point for fewer than 10 lesions, 2 points for 11 to 20 lesions, and 3 points for more than 20 lesions. Severity is graded with 1 point for mild atrophic scarring, 2 points for moderate scarring, 3 points for severe scarring, and 4 points for hyperplastic scarring. The lesion count score is then multiplied by the severity score. The final score is calculated by summing the points from each category, resulting in a total that ranges from 0 to 84, indicating the severity of the condition.
Patients were treated with dermaroller on right side of face and intradermal PRP injections on left side of face [Figure 1, Figure 2].
After a gentle cleansing, both cheeks will be anesthetized with a thick layer of topical anesthetic cream (2.5% lidocaine and 2.5% prilocaine) applied under occlusion for approximately 30 to 45 minutes. For PRP preparation, 5 ml of whole blood will be collected and divided into two sterile conical test tubes of 2.5 ml each, containing acid-citrate dextrose. These will undergo the first centrifugation (hard spin) at 3000 rpm for 15 minutes, resulting in three layers: plasma, buffy coat, and red cell sediment. The red cell sediment will be discarded, and the remaining solution will be subjected to a second centrifugation (soft spin) at 1500 rpm for 10 minutes, creating a dense layer of platelets at the bottom and a clear fluid layer on top. Both the clear fluid (platelet-poor plasma) and PRP will be injected.
Skin needling will be performed using a dermaroller equipped with 192 microneedles, each 1.5 mm in length, arranged in eight rows. After cleansing the face with antiseptic (Betadine solution), 2 to 4 ml of prepared PRP will be injected intradermally into the left cheek using an insulin syringe. The dermaroller will be applied to the right cheek in horizontal, vertical, and diagonal patterns until pinpoint bleeding occurs. The face will then be cleaned with normal saline, and ice compresses will be applied. Patients were advised strict photoprotection (daily application of sunscreen with SPF 30) and to use a topical antibiotic twice daily for three days. A total of four sessions will be conducted at monthly intervals, with the final response assessed after four months.
Response was assessed at 1, 2, 3, and 4 months using a visual analog score (VAS). Patients filled out a questionnaire to evaluate their improvement on a scale from 0 to 10. A score of 0 represented "no response," scores of 1-3 were deemed "poor response," 4-5 indicated a "fair response," 6-7 signified a "good response," and scores of 8-10 were considered "excellent response." 12
Study Design : A comparative single group pre-post assessment.
Duration of study: April 2023 – July 2023.
Sample Size : 50.
Sample size was calculated based on survey of previous literature for an outcome variable on Goodman and Baron’s quantitative scores at baseline and after treatment, with minimum difference of 4 points change in Goodman and Baron’s quantitative scores, with standard deviation of 6.08 11, type 1 error of at least 5%, type 2 error at 10% and keeping statistical power above 90%
n = 50 [25 in each arm: Microneedling (with Dermaroller) and PRP]
Since this was a split face study, only 25 patients were recruited, microneedling with dermaroller was done on right cheek and PRP was done on left cheek in the same patient.
Sampling technique: Systematic random sampling.
Statistical methods: Chi-Square test, Fisher exact test, student t test or any other suitable method at the time of data analysis.
Software used: SPSS 22.0, R Environment, MedCalc, MS Excel and Word.
Data were entered into MS Excel 2010. Data cleaning was carried out and statistical analysis was carried out using SPSS software version 25.0. Continuous variables such as age was presented as mean (standard deviation) based on normality. Categorical variables such as gender, grades and types of scars were presented as frequency and percentage. Data were also tabulated and graphically represented.
Observed difference of VAS scores at different time points was tested for statistical significance using Repeated ANOVA test. A p value <0.05 was considered statistically significant.
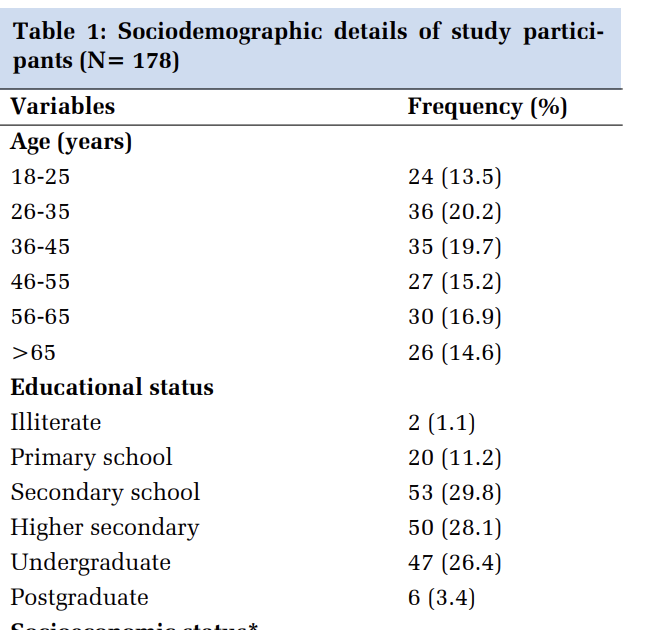
The mean (SD) age of the study participants was 29.8 (5.2) years. [Table 1] Out of 25 patients, 52% (n=13) were males and 48% (n=12) were females. [Table 1] On right side of the cheek, 28% (n=7) had acne scars of grade 3 and grade 4. On left side of the cheek, 32% (n=8) had grade 4 acne scars. [Table 2] Among all the participants, 36% (n=9) had ice pick and rolling scars and 28% (n=7) had ice pick, box car and rolling scars. [Table 3] The VAS score at the end of 1st, 2nd, 3rd and 4th sitting was significantly different (p <0.001) between right (dermaroller) and left cheek (PRP) [Table 4]. Comparatively, following each sitting, VAS scores were higher for left cheek post PRP as compared to right cheek post microneedling [Table 4]. At the end of 1st session of microneedling with dermaroller on right cheek, 44% (n=11) had no response and 56% (n=14) had poor response [Table 5], whereas on left cheek, 100% (n=25) had poor response [Table 6] and this difference was significantly different (p <0.001). At the end of 4 sessions of microneedling on right cheek, 92% (n=23) had fair response [Figure 3, Figure 5, Figure 7] and 8% (n=2) had poor response [Table 5], whereas on left cheek, 80% (n=20) had good response and 20% (n=5) had excellent response [Figure 4, Figure 6, Figure 8] post PRP [Table 6] and this difference was significantly different (p <0.001) [Table 4].
|
Variables |
Frequency |
Percentage (%) |
|
Mean (SD) Age |
29.8 (5.2) years |
|
|
Age (years) |
|
|
|
20-30 |
15 |
60.0 |
|
31-41 |
10 |
40.0 |
|
Gender |
|
|
|
Male |
13 |
48.0 |
|
Female |
12 |
52.0 |
|
Total |
25 |
100 |
|
Variables |
Frequency |
Percentage (%) |
|
Grade on right side |
|
|
|
2 |
6 |
24.0 |
|
3 |
7 |
28.0 |
|
4 |
7 |
28.0 |
|
6 |
4 |
16.0 |
|
9 |
1 |
4.0 |
|
Grade on left side |
|
|
|
2 |
6 |
24.0 |
|
3 |
6 |
24.0 |
|
4 |
8 |
32.0 |
|
6 |
4 |
16.0 |
|
9 |
1 |
4.0 |
|
Total |
25 |
100 |
|
Type of Scars |
Frequency |
Percentage (%) |
|
Rolling |
4 |
16.0 |
|
Ice pick and Box car |
5 |
20.0 |
|
Ice pick and rolling |
9 |
36.0 |
|
Ice pick and Box car and Rolling |
7 |
28.0 |
|
Total |
25 |
100 |
|
|
Mean (SD) |
|
|
|
VAS |
Right |
Left |
P value* |
|
1 month |
0.72 (0.73) |
1.8 (0.71) |
<0.001 |
|
2 month |
1.48 (0.59) |
3.96 (0.84) |
<0.001 |
|
3 month |
2.56 (0.58) |
6.2 (0.71) |
<0.001 |
|
4 month |
4.36 (0.64) |
6.96 (0.67) |
<0.001 |
*Independent t test
|
VAS |
Right Mean (SD) |
P value* |
|
1 month |
0.72 (0.73) |
<0.001 |
|
2 months |
1.48 (0.59) |
|
|
3 months |
2.56 (0.58) |
|
|
4 months |
4.36 (0.64) |
*Repeated ANOVA
|
VAS |
Left Mean (SD) |
P value* |
|
1 month |
1.8 (0.71) |
<0.001 |
|
2 months |
3.96 (0.84) |
|
|
3 months |
6.2 (0.71) |
|
|
4 months |
6.96 (0.67) |
*Repeated ANOVA
|
VAS Grades at 1 st month |
n (%) |
P value* |
|
|
Right |
Left |
||
|
No response (0) |
11 (44.0) |
0 (0.0) |
<0.001 |
|
Poor response (1-3) |
14 (56.0) |
25 (100) |
|
|
Fair response (4-5) |
0 (0.0) |
0 (0.0) |
|
|
Good response (6-7) |
0 (0.0) |
0 (0.0) |
|
|
Excellent response (8-10) |
0 (0.0) |
0 (0.0) |
|
*Chi squared test
|
VAS Grades at 4 th month |
n (%) |
P value* |
|
|
Right |
Left |
||
|
No response (0) |
0 (0.0) |
0 (0.0) |
<0.001 |
|
Poor response (1-3) |
2 (8.0) |
0 (0.0) |
|
|
Fair response (4-5) |
23 (92.0) |
0 (0.0) |
|
|
Good response (6-7) |
0 (0.0) |
20 (80.0) |
|
|
Excellent response (8-10) |
0 (0.0) |
5 (20.0) |
|
*Chi squared test








Acne scars are a common skin concern and addressing them often requires a combination of treatments. Among the promising options for treating atrophic acne scars are microneedling and platelet-rich plasma (PRP) therapy.
Microneedling involves the use of fine needles to create micro-punctures in the skin, which stimulates the body’s natural healing process. This promotes collagen and elastin production, improving the texture of the skin and reducing the appearance of scars. Additionally, microneedling enhances the absorption of topical treatments applied during or after the procedure.8 PRP, on the other hand, is derived from the patient’s own blood and contains growth factors that promote tissue repair and regeneration. PRP is believed to enhance collagen production and skin rejuvenation, making it a beneficial complement to microneedling in the treatment of acne scars. 9, 10
Despite the growing popularity of microneedling and PRP for scar treatment, there is a lack of studies directly comparing the efficacy of these treatments when used independently. To address this gap, our study aimed to evaluate the outcomes of microneedling and PRP as standalone therapies for acne scars. The study involved participants with an average age of 29.8 years, with the majority (60%) aged between 20 and 30 [Table 1]. This is consistent with previous studies, such as Majid’s research, which found a similar age range with a mean age of 22.4 years.13 Our study also observed a slight male predominance (52:48) [Table 1], which aligns with findings from Goulden et al., who noted that males tend to have higher rates of scarring. 14
The types of acne scars presented in the study were primarily a combination of ice pick and rolling scars (36%), followed by a mix of ice pick, rolling, and boxcar scars (28%) [Table 3]. These results are in line with Jacob et al.’s findings, which showed that ice pick scars constitute 60% to 70% of acne scars, with boxcar scars accounting for 20% to 30%, and rolling scars making up 15% to 25%. 15
Previous studies have shown that combining microneedling with PRP yields superior results. For instance, Fabbrocini et al. conducted a split-face analysis that revealed significant improvement on the side treated with both microneedling and PRP compared to microneedling alone.9 Similarly, Nofal et al. reported that patients who received a combination of both treatments experienced statistically significant improvements in scar severity.16 In our study, after four sessions of microneedling on the right cheek, 92% of patients showed a fair response [Figure 3, Figure 5, Figure 7], while 8% had a poor response [Table 5]. In contrast, when PRP was applied to the left cheek, 80% of patients showed a good response, and 20% exhibited an excellent response [Figure 4, Figure 6, Figure 8] [Table 6]. This difference was statistically significant (p < 0.001) [Table 4], suggesting that PRP may offer enhanced benefits when compared to microneedling.
Platelet-rich plasma (PRP) yields superior outcomes compared to microneedling in improving atrophic acne scars. Further research, including larger-scale studies and long-term follow-ups, will help further establish the individual efficacies of microneedling and PRP, and guide clinical practice.
Small sample size, shorter duration of study, patients were not followed up after 4 weeks.
Subscribe now for latest articles and news.