Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i1.25.160
Year: 2026, Volume: 12, Issue: 1, Pages: 23-29
Original Article
Pradeep Kumar Reddy Mereddy1 , B M Soumya2 , C R Preethi3 , Varshini Sindhiya Chanda4
1Assistant Professor, Apollo Institute of Medical Sciences, Hyderabad, Telangana, India,
2Associate Professor, JJM Medical College, Davangere, Karnataka, India,
3Professor, JJM Medical College, Davangere, Karnataka, India,
4Consultant Pathologist, Dr Om Diagnostics, Karimnagar, Telangana, India
Address for correspondence: B M Soumya, Associate Professor, JJM Medical College, Davangere, Karnataka, India.
E-mail: [email protected]
Received Date:27 April 2025, Accepted Date:16 June 2025, Published Date:01 January 2026
Introduction: Dysfunctional uterine bleeding (DUB) is a common diagnosis in gynaecological clinics. It is important to diagnose the endometrial hyperplasias and carcinomas as these have a good prognosis when treated promptly. Progesterone Receptor (PR) is an independent prognostic and promising marker.
Objective/Aim: Aim of this study was to know the various endometrial patterns in DUB through histopathological evaluation in different age groups along with expression of PR in endometrial hyperplasias and carcinomas by immuno-histochemistry.
Methods: This prospective study included 169 patients clinically diagnosed as DUB. This study was conducted in the Department of Pathology, J.J.M.M.C, Davangere from June 2019 to May 2021. Histopathological examination was done along with PR staining on cases with endometrial hyperplasias and carcinomas. Allred scoring system was used to assess PR expression. Data was entered in Microsoft excel 2022 and was analyzed using IBM SPSS software version 23. Comparison between the categorical variables was done using Chi Square test.
Results: The study included 169 women between 18 and 73 years, most 80 (47.3%) of them belonging to perimenopausal age group of 41-50 years. Menorrhagia 114 (67.5%) was the most common bleeding pattern observed. Endometrial hyperplasia without atypia 57 (33.73%) was predominant followed by atypical hyperplasia 4(2.37%) and carcinoma 8 (4.73%). However, there was variation in PR expression in them.
Conclusion: DUB is a diagnosis of exclusion where no cause for abnormal uterine bleeding is found clinically. Histopathological examination from biopsy and curettage samples is a significant mode of determining the cause of DUB. PR has a good prognostic and diagnostic role.
Dysfunctional uterine bleeding (DUB) is defined as abnormal uterine bleeding in the absence of an organic disease. Menorrhagia is seen approximately in 30% of women is one of the most common causes of visit to the gynaecologists. 50% of patients presenting as menorrhagia have DUB.1 Microscopic examination of these tissue samples plays an important role in diagnosing various histopathological patterns in patients.2, 3 Of the various histopathological patterns of endometrium found in different studies, there are also pre-cancerous and cancerous lesions. 4 The diagnostic goal in these cases is to exclude cancer and identify the underlying pathology.5
Endometrial carcinoma is the sixth most common cancer in women and second most common gynaecologic malignancy in developed countries. With rise 6 Their incidence and mortality rates in developed and developing countries are 12.9 & 2.4 per 100,000 women and 5.9 & 1.7 per 100,000 women respectively.7 Socio-economic status was seen as being directly proportional to the incidence and prevalence of these cancers. Endometrial hyperplasias are included in the pre-cancerous lesions leading to this significant disease and so it’s important to diagnose and follow up these lesions for effective and best management of the disease burden.8, 9, 10
Various immuno-histochemical (IHC) markers are being studied for prognostic role of their expression in the management of lesions of the endometrium. 11 Of these, Progesterone Receptor (PR) seems to be one of the significant markers as observed by some authors.12, 13, 14
Hormonal therapy with progesterone is the common and conservative method of management of these lesions which are usually rich in progesterone receptors.15, 16, 17 Loss of PR indicates high proliferation and progression to metastases from primary stage. Some clinical trials are dependent on PR status like the CDK inhibitor studies which are being done to explore activity in PR negative tumours in systemic endometrial cancers.18
Objective of this study is to establish the various endometrial patterns in DUB through histopathological evaluation and study their distribution in different age groups. There is need to know the expression of PR in endometrial hyperplasias and carcinomas by immune histochemistry. Whereas novelty of the study was PR expression has been extensively studied in carcinoma, our study emphasised in endometrial hyperplasia.19
This is a prospective study done on the histopathology of endometrium in 169 patients diagnosed as DUB by clinicians undertaken in the Department of Pathology, J.J.M. Medical College, Davangere over a period of two years from June 2019 to May 2021. All procedures performed in the current study were approved by IRB and/or national research ethics committee (reference number and date) in accordance with the 1964 Helsinki declaration and its later amendments. IRB number - JJMMC/IEC- Sy-09-2019.
Study material used was endometrial sample sent using dilatation and curettage procedure or biopsy from patients presenting with abnormal uterine bleeding diagnosed as DUB. The samples were sent to the Department of Pathology, from patients attending OPD or admitted in Chigateri General Hospital, Bapuji Hospital, Women and Children Hospital and also from private hospitals in and around Davangere, Karnataka.
Inclusion criteria: Endometrial curettage and biopsy samples from patients diagnosed by clinicians as DUB.
Exclusion criteria: Endometrial curettage and biopsy samples from patients sent as DUB by clinicians but found with organic disease of female genital system.
Relevant clinical details and history was recorded from 169 patients. The endometrial samples received from them were fixed in 10% Formalin solution. Gross morphology of the samples received was recorded and tissue embedded totally. The samples were processed using an automated tissue processor, Leica ASP 6025 system. Paraffin tissue blocks were prepared and 3-5 micron thick sections from them were taken for staining with Hematoxylin and Eosin. Microscopic study of these were done and histopathological impression given.
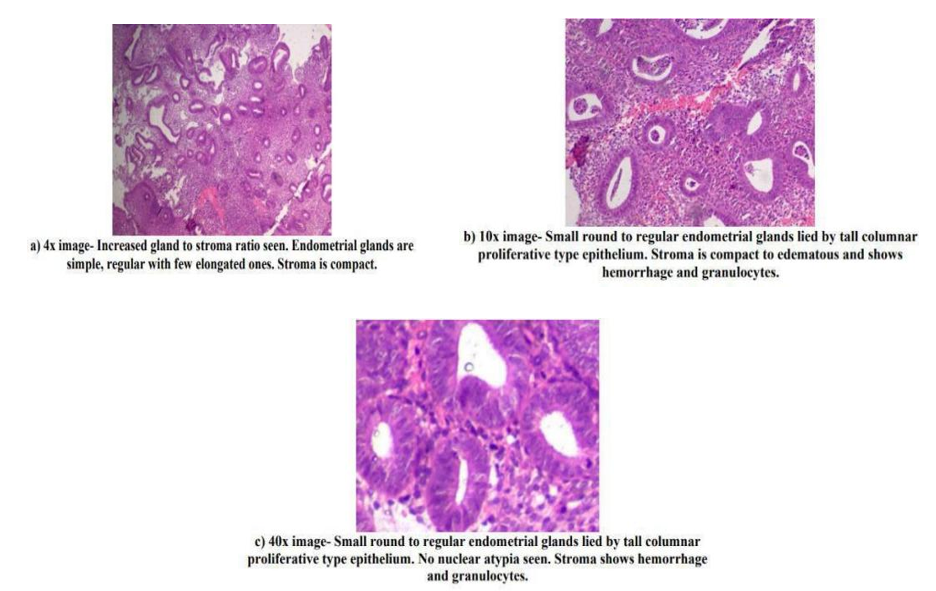
Histopathological parameters included gross and microscopy. Under microscopy, gland:stroma ratio, gland arrangement, dilated glands, shape of gland, gland epithelium and its stratification, stroma type (compact or oedematous), necrosis, hemorrhage, fibrin thrombi, atypia and mitosis. The paraffin tissue blocks of patients diagnosed as endometrial hyperplasias and carcinomas were taken for immuno-histochemical staining to detect PR expression in them. The expression of the marker in these tissues was assessed using Allred Score and studied. PR expression in various tissues like endometrium and breast can be calculated and interpreted by Allred score which is a semiquantitative method. The proportion of stained cells was divided into 6 categories (0: completely negative; 1: < 1% positive; 2: 1–10% positive; 3: 11–33% positive; 4: 34–66% positive; and 5: 67–100% positive).
The intensity of the most predominant area was recorded as 0–3 with higher scores indicating higher intensity. The proportion and intensity scores were added, yielding the Allred score (0–8). The cut-off level for each hormone receptor was ≥3, which is the cut-off level usually used in breast cancer.20
Informed consent was taken from all the subjects included in the study. Ethical committee clearance was taken from Institutional Ethical committee. Data was entered in Microsoft excel 2019 and was analyzed using IBM SPSS software version 23. Categorical data was represented in the form of frequency and percentage. Quantitative data was represented using mean, median, range and standard deviation. Since the data has been categorised into three groups, in place of nonparametric test, we preferred using a parametric test like Chi Square test with p< 0.05 as significant.
The study included 169 patients presenting with DUB between the ages 18 and 73 years with a mean age of 41.98 years. Most of them belonged to 41-50 years age group followed by 31-40 years group with 80 (47.3%) and 52 (30.8%) cases respectively.
Among 169, 5 were nulliparous, 19 were primiparous and 145 were multiparous with parity ranging from 2 to 7. Out of the multiparous patients, those with parity 2 and 3 were leading with 74 (43.8%) and 55(32.5%) cases respectively.
Menorrhagia was the most common presenting pattern which was seen in 114 (67.5%) cases. This was followed by 17 (10.1%) cases of metrorrhagia, 15 (8.9%) cases of dysmenorrhea and 12 (7.1%) cases of postmenopausal bleeding. Menometrorrhagia, polymenorrhea and polymenorrhagia were other patterns which were seen in less than 5% of cases each. USG was done in 128 out of 169 patients. Of these, 77 showed thickened endometrium and 51 of them had normal endometrium. There were no other lesions detected in any other organs of these patients.
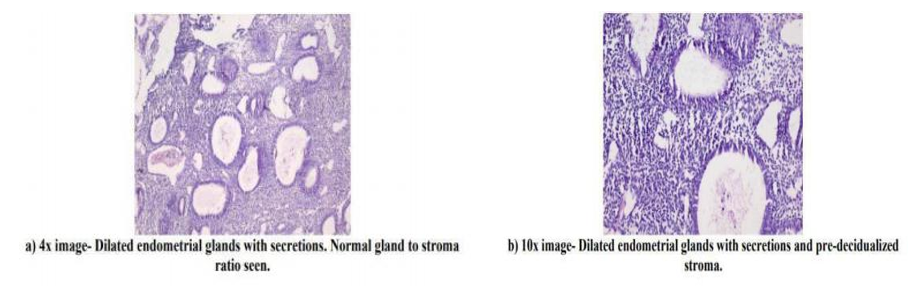
Of the 169 cases, endometrial hyperplasia without atypia was the most common diagnosis given with 57 (33.73%) cases. These were followed by secretory phase endometrium, disordered proliferative endometrium, proliferative phase endometrium and menstrual phase endometrium with 28 (16.57%), 27 (15.98%), 25 (14.79%) and 14 (8.28%) cases respectively. There were 5 (2.96%) cases of atrophic endometrium, and 1 (0.59%) case diagnosed as irregular shedding. 4 (2.37%) cases of Endometrial atypical hyperplasia and 8 (4.73%) cases of endometrial carcinoma were also seen in which 7 (87.5%) cases were diagnosed as endometrioid endometrial carcinoma and 1 (12.5%) case diagnosed as serous papillary carcinoma. Histological features of endometrial glands and stroma in DUB was varied in every condition.
Proportion of positivity of IHC marker PR along with scoring was done in both endometrial hyperplasia and endometrial carcinoma cases (Table 1, Table 2). Intensity of PR marker in endometrial hyperplasia and carcinoma was assessed (Suplementary Table S1, S2).
|
Proportion of PR positive cells |
Endometrial hyperplasia without atypia |
Endometrial atypical hyperplasia |
No. of cases |
|
SCORE 0 |
0 |
0 |
0 |
|
SCORE 1 |
1 |
0 |
1 |
|
SCORE 2 |
4 |
1 |
5 |
|
SCORE 3 |
9 |
0 |
9 |
|
SCORE 4 |
12 |
0 |
12 |
|
SCORE 5 |
31 |
3 |
34 |
|
Total |
57 |
4 |
61 |
|
Proportion of PR positive cells |
No. of cases |
Percentage |
|
SCORE 0 |
3 |
37.5 |
|
SCORE 1 |
0 |
0 |
|
SCORE 2 |
0 |
0 |
|
SCORE 3 |
2 |
25 |
|
SCORE 4 |
1 |
12.5 |
|
SCORE 5 |
2 |
25 |
|
Total |
8 |
100 |
Thus, Allred score was derived for both endometrial hyperplasia and carcinoma cases and scores were compared using Chi- square test and found to have p value of < 0.000001 which is highly significant (Supplementary S3, S4, S5). Allred scoring was independently performed by 2 pathologists and in cases of discordance final score was given by consensus.
Dysfunctional Uterine Bleeding (DUB) is a frequent diagnosis in routine gynaecological practice. It is also the underlying cause for performing hysterectomy in many of these patients.21, 22 DUB can occur at a variety of ages. It could be seen in women with anovulatory or ovulatory cycles, the former group usually dominating the show.
In the present study, most of the cases are in the age group of 41-50 years with 80 (47.3%). Many of the perimenopausal women belong to this group. These cases were followed by 52 (30.8%) cases in the 31-40 years age group. The two patterns were similar to DUB patients in many other studies. However, few other studies reported the opposite with highest number of cases as belonging to the 31-40 years age group followed by the women belonging to the 41-50 years group. In ages greater than 50 years which includes most postmenopausal women, 18 (10.7%) cases were reported in this study. This was similar to studies by Nepal et al, Fatima et al and Nayak et al. 23, 24, 25 There were few other studies which showed lesser percentage of cases in this category ranging between 2.7 to 4.6%.26, 27 Parity of the patient is an important parameter as it is known to influence treatment patterns. Hormonal therapy is one of the main treatments to control DUB and in women where uterus needs to be preserved for conception. Hysterectomy can be an important option and permanent solution to stop bleeding, especially in cases resistant to treatment, those with atypical lesions and multiparous women who do not wish to conceive. In the present study, DUB was found predominantly in multiparous women (parity ≥ 2) with 85.8% of the total cases. In the multiparous category, multipara 2 and 3 were leading with 43% and 32.5% of the total cases. Khan et al also described this trend in their study which was also observed in other studies. 28 19 (11.2%) women were primiparous and only 5(3%) of them were nulliparous. These results are comparable to many other studies. Pilli et al, Kaur et al and Mehta et al discuss similar findings in their studies with DUB patients being mostly multiparous. Most women (67.5%) in the current study presented with menorrhagia as the bleeding pattern which was similar to majority of the studies on DUB patients. 29, 30, 31
Metrorrhagia was the next most common pattern accounting for 10.1% of the total cases. Very few studies had metrorrhagia as the dominant bleeding pattern. 32 Other bleeding patterns seen here in lower percentages were dysmenorrhea, postmenopausal bleeding, menometrorrhagia, polymenorrhea and polymenorrhagia. The present study highlights endometrial hyperplasia as the most common histopathological diagnosis when compared singly with other diagnoses. 61 (36.10%) of the total 169 cases had hyperplastic endometria. Kariappa et al had proliferative endometrium as the leading diagnosis. 33
In the present study, a highly significant p value for Allred score comparison between the two entities of endometrial hyperplasias and carcinomas was obtained. This indicates that there was a good difference in PR expression of the two entities. Endometrial hyperplasias had the tendency to have rich PR expression commonly while carcinomas usually presented with negative or poor PR expression similar to other studies. Those other carcinomas with rich PR expression were lower grades of endometrioid endometrial carcinoma having better prognosis and response to hormonal therapy as described earlier by others.34, 35
Limitations: The study has only few cases of endometrial carcinoma and endometrial atypical hyperplasia. So, comparison of PR expression between endometrial hyperplasia without atypia and above mentioned two groups couldn’t be confidently concluded.
DUB is a common gynaecological problem occurring in majority of perimenopausal women, followed by women in reproductive age group. Histopathological examination from biopsy and curettage samples is a significant mode of determining the cause of DUB. PR is a significant IHC marker which can be used for diagnostic and prognostic purposes. Rich PR expression was seen in most precursor lesions of endometrial hyperplasias while endometrial carcinomas showed a predilection for poor and negative PR scores. PR has a good prognostic and diagnostic role.
Funding: None
Conflict of Interest: Nil
Subscribe now for latest articles and news.