Introduction
The irregular shaped scapulae bone is located posterior to the thoracic wall. One of the divisions from upper trunk of brachial plexus is suprascapular nerve (C5, C6) which first crosses the supraclavicular fossa to reach the notch located in superior border of scapula. The supraspinatus and the infraspinatus muscles located in the respective fossa, seen in the dorsal surface of scapula was supplied by suprascapular nerve 1. The ossification of the transverse ligament bridging the notch compresses the suprascapular nerve 2. But the suprascapular vein and suprascapular artery escapes from such compression as they go directly above the fibro-osseous tunnel formed by a superior transverse scapular ligament. It’s not only the SSN size but its shape also plays crucial role in nerve compression syndrome. The suprascapular notch was categorized based on their shape as Type I to Type VI. A higher chance of nerve compression can occur in a shallow J shape - Type IV SSN leading to atrophy of muscles supplied by it, resulting in the hollowed appearance of superior scapular fossa 3. The Type VI notch is more vulnerable to cause nerve compression syndrome as the ligament bridging the notch was completely ossified resulting in a narrow foramen 4. So, the suprascapular notch of the scapula is considered an important landmark to locate the suprascapular nerve during operative procedures 5. Visualising a suprascapular neurovascular bundle is vital in case of chronic shoulder pain of unknown etiology to get rid of the pain by giving nerve blocks 6. Suprascapular neuropathy in Type VI and Type IV notch is an uncommon cause of shoulder pathology with vague pain. So the patient is unaware of the complications and if the condition is left untreated for months can lead to muscle wasting 7, 8. The wasting involves both supraspinatus and infraspinatus muscle as a result of narrow Type IV notch and ossified ligament seen in Type V, Type VI notch resulting in limited external rotation and abduction of shoulder movements 9. This study helps the orthopaedician’s for locating SSN and suprascapular nerve while performing arthroscopic shoulder operations. It also helps to classify and categorise the more risk type of SSN (Type VI) causing neuropathy using a plain radiograph.
Aims and Objectives
-
To estimate the proportion of the six types of SSN (based on the classification by Rengachary et al) among dry human scapulae of South Indian origin.
-
To estimate the notch dimensions (superior transverse length, notch depth, middle transverse length and inferior transverse length) in these scapulae.
Materials and Methods
After getting Institutional Ethical Committee clearance (AMC/IEC/Proc.No.3/2020), the study proceeded further. Fifty (50) dry human scapulae bone, which includes both right (24) and left side (26) scapulae. These samples were collected from the Anatomy Department with the concern of respective authorities.
Study type
Descriptive study
Study population
Scapulae bone of South Indian origin
Sample size
50 (Scapulae bone — 24 Right side and 26 Left side)
Study duration
6 months
Inclusion criteria
Scapulae with complete fusion of ossification centres and without gross deformities or damage to the superior border
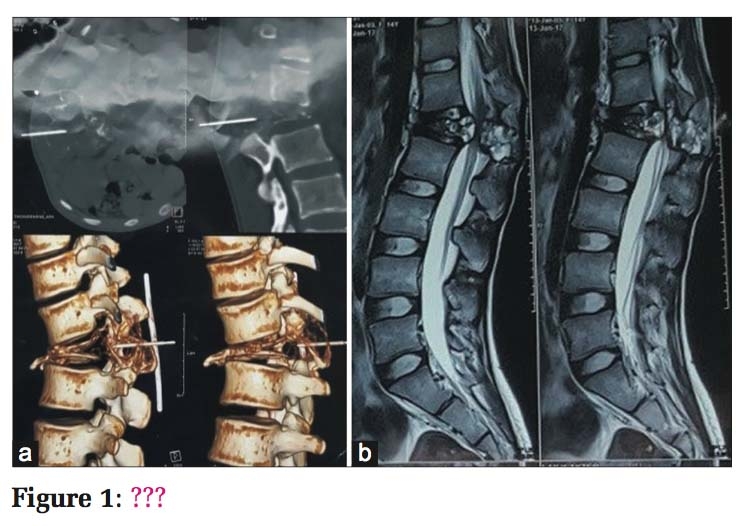
According to Rengachary et al SSN was categorised as six varieties as described below10
Type I. — Slight indentation or Absent
Type II. — Narrow V shape
Type III. — Broad U shape
Type IV. — Shallow J shape
Type V. — STSL with partial ossification
Type VI. — STSL with Complete ossification
All 50 scapulae bone were scrutinised to assess SSN shape and was categorised into six types. Each type of SSN was labelled with a specific number to arrange them in order. One scapula from each type was arranged in ascending order and to illustrate the categorisation of the notch, as shown in Figure 1.

The following parameters of six types of notches were recorded as given below 11, 12.
-
Superior Transverse Length (STL) – Distance measured in the superior aspect of notch from its right to left end.
-
Notch Depth (ND) – Distance from median transverse superior length to deepest point of Suprascapular notch.
-
Middle Transverse Length (MTL) – Distance measured at the level of the midpoint of maximum depth.
-
Inferior Transverse length (ITL) - Distance measured between curved arch near the base of SSN as shown in Figure 2.

The above parameters of the suprascapular notch were measured using the Digital vernier caliper as shown inFigure 3 with a measuring accuracy of 0.01mm. All the parameters were taken thrice to avoid observer’s error, and the average value of each parameter was noted.

The occurrence and percentage of notch type prevalent were noted to compare it with other studies. The scapula with completely ossified transverse ligament falls under notch type-VI, and its prevalence was compared with other types of notches. Even the side of the scapulae (Right or Left) with a maximum number of the type-VI notch was noted to compare the incidence between the two sides. The statistical analysis was done using SPSS software version 25. The continuous variable was denoted by mean, median and sample standard deviation. The nominal variable was represented by number (Digit) and percentage.
Observations and Results
In the present study, 50 scapulae (24 right sides, 26 left sides) were categorised into 6 with their percentage distribution as shown in Table 1.
|
Sl. No |
Types of Suprascapular notch |
Right side (%) n =24 |
Left side (%) n =26 |
TOTAL (%) n =50 |
|
1 |
Type I |
6 (25%) |
6 (23.07%) |
12 (24%) |
|
2 |
Type II |
6 (25%) |
2 (7.69%) |
8 (16%) |
|
3 |
Type III |
7 (29.16%) |
5 (19.23%) |
12 (24%) |
|
4 |
Type IV |
3 (12.5%) |
7 (26.92%) |
10 (20%) |
|
5 |
Type V |
2 (8.33%) |
4 (15.38%) |
6 (12%) |
|
6 |
Type VI |
0 |
2 (7.69%) |
2 (4%) |
The Type III, Type I notches were noticed in 12 scapulae (24%). Type IV was observed in 10 scapulae (20%), Type II in 8 scapulae (16%), Type V in 6 scapulae (12%) and Type VI in 2 left-sided scapulae (4%) where suprascapular notch was converted into a foramen. Type VI with completely ossified STSL was noticed only in the left side scapulae as shown in Table 1.

In Type II, IV, V the ITL was 4.38±1.04mm, 4.13±0.66mm and 4.54±1.84mm respectively but in Type III it was 5.53±1.02mm greater than other types. MD in type II, IV was 7.27±0.70mm, 6.32±1.19mm which is less than Type III, V with 9.66±2.08mm, 9.14±1.90mm respectively, as shown in Figure 4. In Type V notch, STL was less than other types as the STSL was partially ossified. In Type III notch ITL was higher than other types as the shape of SSN was U showing a broader base. As the Type IV notch shows a reduction in MD when compared to Type II, III and V notch due to narrow SSN, which may cause nerve compression.
|
Sl. No |
Notch Types |
Transverse diameter of scapulae (mm) |
|||||||
|
Superior |
Middle |
Inferior |
Notch depth |
||||||
|
Right Scapulae (Mean±SD) |
Left Scapulae (Mean±SD) |
Right Scapulae (Mean±SD) |
Left Scapulae (Mean±SD) |
Right Scapulae (Mean±SD) |
Left Scapulae (Mean±SD) |
Right Scapulae (Mean±SD) |
Left Scapulae (Mean±SD) |
||
|
1 |
I |
Notch is absent |
|||||||
|
2 |
II |
14.34±2.97 |
12.50±0.36 |
10.14±2.30 |
8.58±1.09 |
4.45±1.10 |
4.39±0.40 |
7.62±0.55 |
6.57±0.39 |
|
3 |
III |
10.01±3.30 |
11.37±3.06 |
7.63±2.39 |
8.26±1.78 |
5.19±1.02 |
5.45±0.87 |
8.93±1.86 |
9.68±2.09 |
|
4 |
IV |
9.54±2.45 |
8.80±1.18 |
7.42±1.11 |
5.98±1.17 |
4.59±0.53 |
3.94±0.56 |
7.26±0.76 |
5.93±1.02 |
|
5 |
V |
3.59±2.23 |
6.96±3.06 |
8.27±1.03 |
8.03±1.94 |
5.76±0.18 |
3.94±1.77 |
9.44±0.18 |
9.00±2.11 |
|
6 |
VI |
Notch converted into a foramen |
|||||||
In Type I, the notch was not discrete whereas in Type VI, the notch converted into foramen due to STSL ossification, so their dimensions were not recorded. In type II notch, STL in both right and left scapulae was 14.34mm, 12.50mm higher than MD with 7.62mm and 6.57mm respectively, representing V shape notch. In type III notch, STL in both right and left scapulae was 10.01mm, 11.37mm whereas MD was 8.93mm, 9.68 mm respectively, showing a slight difference in mean measurements. In U shaped notch (Type III), inferior transverse length in the right and left scapulae was higher than Type II and IV notches. In Type IV notch, maximum depth in both right and left side was 7.26mm, 5.93mm which was comparatively less than other types since J shape notch depth was less than other types. In type V notch, STL measurements vary with the ligament ossification, so on right side, it was 3.59mm which is less than the left side as it is 6.96mm.
Discussion
The existing study shows the following frequency distribution of notches V ˂ VI ˂ II ˂ IV ˂ III& I and was compared with other studies as shown inTable 3.
|
Authors |
State |
Types of Notches |
|||||
|
I. |
II. |
III. |
IV. |
V. |
VI. |
||
|
Vibhash Kumar Vaidya (2018) 12 |
Uttar Pradesh |
20% |
15% |
26.42% |
28.57% |
7.14% |
7.14% |
|
Albino et al., (2013)13 |
Rome |
12.4% |
19.8% |
22.8% |
31.1% |
10.2% |
3.6% |
|
Muralidhar Reddy Sangam (2013) 14 |
Andra Pradesh |
21.15% |
8.65% |
59.61% |
2.88% |
5.76% |
1.92% |
|
Vasudha TK et al., (2013) 15 |
Karnataka |
6.08% |
0% |
34.78% |
19.13% |
1.73% |
4.34% |
|
Girish V. Patil et al., (2014) 16 |
Kerala |
20.54 % |
14.29 % |
25 % |
35.71 % |
1.79 % |
2.68 % |
|
Kannan et al., (2014) 17 |
Pondicherry |
20% |
10% |
52% |
4% |
4% |
10% |
|
Agrawal D et al., (2015) 18 |
North India |
3.43% |
26.37% |
52.60% |
3.84% |
0.82% |
12.91% |
|
Manoj Kumar Reddy.G (2017) 19 |
Andhra Pradesh |
6.6% |
41.2% |
44.3% |
0% |
4.7% |
2.8% |
|
Saikia R et al., (2017)20 |
Assam |
27.51% |
7.75% |
40.31% |
21.31% |
0% |
3.1% |
|
Vedha. S (2017) 21 |
South India |
21.2% |
0% |
53.2% |
5.2% |
5.2% |
9.2% |
|
Shalom Elsy Philip (2017) 22 |
South India |
9% |
36% |
38% |
8% |
6% |
3% |
|
Sachin Patil et al., (2019) 23 |
New Delhi |
22.42% |
12.98 % |
53.98 % |
0% |
7.08 % |
3.54% |
|
Chaitra et al., (2019) 24 |
South India |
22% |
33% |
18% |
13% |
4% |
10% |
|
Daripelli S et al., (2020) 25 |
Telangana (India) |
27.5% |
22.5% |
30% |
5.5% |
4.5% |
10% |
|
Adewale AO et al., (2020) 26 |
Uganda |
16.3% |
12.2% |
51% |
12.2% |
4.1% |
8.2% |
|
Tsikouris G et al., (2021) 27 |
Greece |
54.85% (Unossified suprascapular ligament) ( Polguj’s method of classification) |
25.8% |
19.35% |
|||
|
Kaledzera et al., (2022) 28 |
Malawi |
36.8% |
16.8% |
29.6% |
4% |
7.2% |
0.8% |
|
Nasr AY (2023) 29 |
Saudi Arabia |
Rt-43.3% Lt-36.7% |
Rt- 26.7% Lt-30% |
Rt- 13.3% Lt-13.3% |
Rt-10% Lt-10% |
Rt- 6.7% Lt-10% |
(According to Polguj’s classification) No such type |
|
Present study (2023) |
Tamil Nadu |
24% |
16% |
24% |
20% |
12% |
4% |
Vibhash Kumar Vaidya et al. found the most dominant type being Type IV, second most common Type III and least Type VI which correlates with the present study as collected samples belongs to a specific (Indian) population 12.
Paolo Albino et al. observed the percentage distribution of SSN showing prevalent Type IV notch in 31.1% scapulae which differs from our study as Type III, and I was found to be most common. So, such highlighted differences in SSN may due to racial or regional differences owing to such a result 13.
Sangam et al. described the incidence of various notches in which Type III was prevalent and least was Type VI. SSN dimensions revealed that MTD dimensions of Type IV notch was less with 1.75 ± 0.63mm. MD in Type V notch shows the higher value of 9.09 ± 2.69mm and it was least in Type IV with 6.32±1.19mm. STD in Type V notch was less with 5.65 ± 0.9mm since the medial part of STSL was partially ossified. The findings were similar to our present study both in parameters and incidence of notch type, which depicts the existence of regional and genetic factors, may influence the notch type 14.
According to Vasudha TK, et al. Type III was most common, Girish V. Patil et al. found Type IV was the prevalent type, but both the author found the least variety was Type V with an incidence of 1.73%, 1.79%, respectively, which is comparatively less than Type VI with 4.34%, 2.68% respectively. So, the possibility of nerve compression was higher when compared to the present study as the least type was Type VI. The coracoid process of scapula’s ossification and other bony landmarks may also influence the notch type producing such difference 15, 16.
Usha Kannan et al. studied 400 dry scapulae of the South Indian population and observed Type III SSN was prevalent and Type IV, V being less common which is similar to our study (50 scapulae) with incidence of Type IV was 20%. Although both the studies were done in the same South Indian population, results may be dissimilar due to the major difference in the sample size 17.
Agrawal D et al. found the incidence of distribution of suprascapular notch in 728 dry scapulae in North Indian population. The most common type of notch was Type III – U shape in 52.60% (383 scapulae), next Type II– V shape in 26.37% (192 scapulae) and the least was Type V in 0.82% (6 scapulae). The suprascapular nerve entrapment syndrome occurs in Type VI with completely ossified ligament in 12.91% (94 scapulae). This result correlates with the present study with prevalent Type III in 24% (12 scapulae) and the least Type VI in 4% (2 scapulae). The percentage distribution of Type VI was higher when compared with the present study which may be due to the large sample size and nature of work which involves frequent shoulder movements 18.
Manoj Kumar Reddy G studied the frequency of distribution of suprascapular notch and found the majority of scapulae fall under Type III (44.3%), Type IV (0%), Type VI (2.8%). In Type VI out of 3 scapulae, one belongs to right and 2 belong to left side. In present study, the Type VI notch was observed on the left side scapula that does not correlate with handedness as right-hand dominance was observed in the majority population. This means that not only handedness, but also genetic factor serves as an etiological factor for the ossification of STSL 19.
Saikia R et al. reported Type III notch was predominant succeeded by Type I, IV as noted in the present study except Type V where the author found none of the scapulae showed partial ossification of STSL, but in the current study Type V notch observed in 12% scapulae, such disparity may be due to varied method which was followed by the author to evaluate the notch type based on Nagaraj et al.classification20.
Vedha S reported Type III notch was prevalent with 53.2%, Type I with 21.2% next is Type VI with 9.2%, but the present study shows only 4% of Type VI notch. Such a higher incidence of ossification of STSL alters the action of omohyoid muscle resulting in the bone renovation. Occupation of an individual may play a key role as vigorous overhead abduction movement changes the incidence of Type VI notch among a similar population 21.
Shalom Elsy Philip observed that Type III and II notch was prevalent with 38% and 36%, respectively and least Type VI (3%). The mean STD, MTD, MD for Type II, III, IV, V notch correlates with the present study because the samples collected were from South India and the SSN was classified by using Rengachary classification 22.
Sachin Patil et al. described the percentage distribution of various notches. They found Type III with 53.98 %, Type I with 22.42%, Type VI with 3.54%, the least Type IV 0%, which relates with the present study. However, the only difference is Type IV showing 20%, which is the second most common type noticed in our study. The type of notch may be determined by a specific population showing regional variation as the sample belongs to the North-central part of India 23.
Chaitra et al. study showed Type II notch with 33% (Prevalent type), Type I 22%, Type VI 10%, least Type V 4% showing partially ossified STSL. The findings vary slightly from our study as the ossified coracoid process creates an impact on the frequency of SSN type distribution. The STL and MTL in Type II and III were higher than Type IVand V notches. The mean maximum depth in Type V notch (6.64±1.96 mm) was less than other notch types (8.27±1.58 mm, 10.64±2.13 mm, 8.8±0.78 mm) which correlates with the present study as dimensions in SSN decides the type of SSN. Suprascapular nerve entrapment depends upon the availability of surface area provided by the notch type. Slight variation in incidence may be due to various factors as the type of notch was influenced by the population from which the sample was collected, the method of evaluation and the method used to classify the notch type 24.
Dariselli S et al. found the predominant type of notch was Type III 30% (60 scapulae), Type I 27.5% (55 scapulae), Type II 22.5% (45 Scapulae) and least was Type IV 5.5% (11 scapulae), Type V 4.5% (9 scapulae). The STD, MD in Type III, II, IV was 9.69±2.53mm, 8.04±2.56mm, 9.22±2.58mm, 6.35±2.12mm and 6.31±1.27mm, 5.92±8.1mm which correlates with the present study, since the study was done in same South Indian population with similar predominant type of notch noticed in Type I, III 24% (12 scapulae) and the least Type VI 4% (2 scapulae). The MD was minimum in Type IV with 6.32±1.19mm as it is J shape and MD was maximum in Type III with 9.66±2.08 mm as it is U shape 25.
Adewale AO et al. studied 50 scapulae bones of Uganda population and classified the suprascapular notch into 6 types based on Rengachary’s classification. The percentage distribution of completely ossified STSL (Type VI) was 8.2% and the prevalent type of notch was Type III with 51%, followed by Type I with 16.351%. The results were in accordance with the present study, as the prevalent Type was Type III with 24% but Type VI being 4% which is comparatively less as there is a racial difference exhibit among the study samples 26.
Tsikouris G et al. studied in 31 frozen specimens, in which STSL in 8 scapulae (25.8%) was partially ossified, in 6 scapulae (19.35%) completely ossified and in remaining 17 scapulae (54.85%) it was not ossified. The classification of suprascapular notch was done by Polguj et al classification based on the arrangement of neurovascular structures in suprascapular notch. The notch was classified into four types with predominant Type I in 70.97% (22 scapulae), followed by Type II in 22.58% (7scapulae), Type III in 6.45% (2 scapulae) and Type IV 0% with maximum MTD was observed in Type III with 14.05±1.02mm and least Type I with 8.64±3.34mm. The ossified ligament was observed in 14 out of 31 scapulae (partial – 8 and complete – 6) such result was not associated with the present study as 8 out of 50 scapulae (partial – 6 and complete – 2). This difference is mainly because the classification of scapulae was done by the author by using Polguj’s method and the types were classified based on suprascapular vessels and nerve in relation to the suprascapular notch 27.
According to Kaledzera et al. the most common type of notch was Type II in 36.8% (46 scapulae), secondly Type III in 29.6% (37 scapulae) and the least was Type VI in 0.8% (1 scapula). The STL, MTL, MD in Type II was 1.3.13cm, 1.013cm and 0.375cm whereas for Type IV it was 0.650cm, 0.400cm and 0.350cm respectively which indicates the shallow notch was observed in Type IV (J shape) which correlates with the present study as STL,MTL, MD was 9.02±1.79mm, 6.41±1.40mm and 6.32±1.19mm respectively. The result indicates Type IV (J shape) notch has minimum depth when compared to other type of notches. But the prevalence type was Type II, not in accordance with the present study as Type I & III being the most common type. Such variation in dominant notch type may be due to regional variation and environmental factors might play a major role for such difference in notch dimensions 28.
Nasr AY studied 120 dry scapulae of Saudi Arabian population to classify the notch type based on Polguj’s classification and found the predominant type was Type I (J shaped) notch, 43.3% in right side and 36.7% in left side. The least type was Type V (Absent) notch with 6.7% in right side and 10% in left side scapulae. The morphometric measurements observed in J shaped notch VD (12.9±2.8 mm) > STD (10.9±2.2 mm), U shaped notch VD (11.0±2.65 mm) = STD (10.9±2.53mm), V shaped notch VD (9.9±1.1 mm) < STD (12.9±2.6mm) which is in accordance with the present study showing the similar mean J shaped notch VD (12.9±2.8 mm) > STD (9.54±2.45mm), U shaped notch VD (8.93±1.86mm) = STD (10.01±3.30mm), V shaped notch VD (7.62±0.55 mm) < STD (14.34±2.97 mm). But the predominant type was J shape which is not in accordance with the present study due to following reason, as the classification was done based on Polguj’s classification and the samples belong to Saudi Arabian population 29.
Conclusion
The prevalence of completely ossified STSL (Type VI) was even though less in South Indian population but Type IV with J shape notch was the 2nd most common type which is dangerous as the depth of the notch was shallow resulting in suprascapular nerve compression. The pain due to suprascapular neuropathy by an ossified superior transverse suprascapular ligament and a shallow notch will be similar to the rotator cuff tear. Hence, anatomical knowledge about the SSN and its types are necessary to separate it from other related pathology. The present study helps clinicians identify suprascapular neuropathy in high-risk groups like sports persons because of their routine training activities. So, early diagnosis of suprascapular nerve entrapment in SSN is vital to prevent the atrophy of supraspinatus and infraspinatus muscle resulting in restricted movements in shoulder joint.
Authors contributions
SS – Manuscript preparation, Data collection, Data analysis, Interpretation of result, Article submission, BS – Drafting manuscript, Data collection, Data analysis, Result interpretation AK - Manuscript preparation, Data collection, Data analysis, Photographs, RS – Drafting manuscript, Data collection, Result interpretation
Conflicts of Interest
Nil