Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.010
Year: 2021, Volume: 7, Issue: 3, Pages: 45-50
Original Article
Gopalakrishna Ravichandra1 , Kibballi Madhukeshwar Adarsh2 , Kumar Harsha3 , Sudhir Shyam4 , Acharya Devadas5
1Professor and Head, Department of Radiodiagnosis, Yenepoya Medical College, Mangaluru, Karnataka,
2Associate Professor, Department of Radiodiagnosis, Yenepoya Medical College, Mangaluru, Karnataka,
3Senior resident, Department of Radiodiagnosis, Yenepoya Medical College, Mangaluru, Karnataka,
4Professor and Head, Department of Pediatrics, Yenepoya Medical College, Mangaluru, Karnataka,
5Professor, Department of Radiodiagnosis, Yenepoya Medical College, Mangaluru, Karnataka
Address for correspondence:
Kibballi Madhukeshwar Adarsh, Associate Professor, Department of Radiodiagnosis, Yenepoya Medical College, Mangaluru, Karnataka. E-mail: [email protected]
Background: Corpus callosum (CC) abnormalities are usually associated with abnormalities of cerebral cortex as they facilitate the communication between hemispheres. Developmental delays are associated with white matter abnormalities. The association between the developmental delays and CC thickness is less studied. Aims: To assess the difference in the sizes of various regions of corpus callosum in cases of children with developmental delay and children with normal milestones and to determine the association between different types of developmental delays with thinning of corpus callosum. Methods: This was a cross-sectional study conducted among children with developmental delay as cases and children without developmental delay as comparison group. Imaging of CC was performed with 3T MRI. Thicknesses of CC at its various regions were measured and mean thickness was compared among cases and comparison group. Results: The total number of children included were 102 (51 cases and 51 comparisons). Mean age of the children was 2.9 (±1.24) years and majority were male children (55%). The difference in the mean thicknesses of cases and comparison groups in various regions of CC were found to be statistically significant (p-value <0.001). The association between the thickness of anterior midbody and splenium of CC with motor milestone delay and language milestone delay respectively was also found to be statistically significant (p-value 0.003 and <0.001 respectively). Conclusion: Decrease in the thickness of CC is directly associated with developmental delays. Hence, developmental delays need to be evaluated in children with corpus callosum abnormalities and vice versa.
Keywords: Developmental delays, corpus callosum, 3T MRI
Growth and development are unique phenomena among the pediatric population. Increase in the physical size of the body is growth and increase in skills and function is development. Growth and development are always considered as whole because the child grows and develops together. [1] While the sequence of events is similar across populations, the rates vary from child to child and age to age.
This pattern of development is averaged across child population to obtain a set of milestones or markers which signal appropriate growth and development. [2]
The child is usually assessed across the major domains of gross motor, fine motor, social and language skills so as to ascertain whether the development was satisfactory. [3] When the child fails to attain skills or faculties within the reference range for the age, a delay is suspected and then the cause is sought out. The effects of delay maybe static following the restricted event in the history or it may be progressive with residual and recurring alternations in the development of the child. [4] The term developmental delay (DD) covers a heterogeneous group of conditions that start early in life and present with delay in development or an abnormal pattern of developmental progression. [5]
The largest white matter structure in the human brain is corpus callosum (CC) and it connects the right and left hemispheres. It has an important role of integration of the two hemispheres and facilitates the normal communication between them. [6] Abnormalities in development of the cerebral cortex may be reflected by abnormalities in the corpus callosum and vice-versa. [7]
The prevalence of the corpus callosal abnormalities is found to be 2-3% in individuals with developmental challenges and 0.3 to 0.7% among general population who undergo neuro-imaging. [8,9] There can be multiple conditions resulting in thinning of CC. They can be divided into primary and secondary causes. The primary cause can be due to abnormal or failed myelination resulting in hypomyelinating conditions like leukoencephalopathies, metabolic disorders or microcephaly. Secondary causes can be diffuse injuries like hypoxic-ischemic encephalopathy, hydrocephalus etc.[10]
The presence of hypoplastic CC is highly associated with cerebral dysgenesis as a cause of cerebral palsy. Corpus callosal alterations are noted in various psychiatric and neurodevelopmental disorders like autism[11] , mental retardation, developmental dyslexia, attention deficit hyperactivity disorder[12] , developmental language disorder, schizophrenia and Downs syndrome. The abnormalities found in CC in developmental dyslexia and developmental language disorder has been proven. [13] Prevalence of DD among children has been reported as 5–10%. Based on the previous studies, around 60% cases have abnormal Magnetic Resonance Imaging (MRI) findings. [14] Brain MRI is an important modality for assessment of these patients and neuroimaging helps to reveal previous injuries or any other specific abnormalities. CC and its parts can be discretely identified and has shown to produce sharp images on MRI.
Thus, this study was conducted to assess the difference in the sizes of various regions of corpus callosum in cases of children with developmental delay and children with normal milestones. The other objective of the study was to determine the association between different types of developmental delays with thinning of corpus callosum.
This cross-sectional study was conducted among patients referred to the department of radio diagnosis of a medical college hospital of coastal Karnataka. The data was collected from January 2018 to December 2018.
The patients who were diagnosed with DD and aged between 2 years to 5 years were included as study subjects/cases. Children who underwent MRI for other conditions (seizures/ acute trauma etc.) with DD being ruled out from their diagnosis were included in the comparison group. The cases and comparisons were age and gender matched. Patients who had undergone neurosurgery, lesions disturbing the anatomy of the CC, presence of complete/partial agenesis of CC, cerebral abnormalities, neuropsychological disorders, children with premature birth, pre and perinatal trauma/ hypoxic injury were excluded. Also children with motion artifacts and children whose parents did not give written informed consent were excluded from the study.
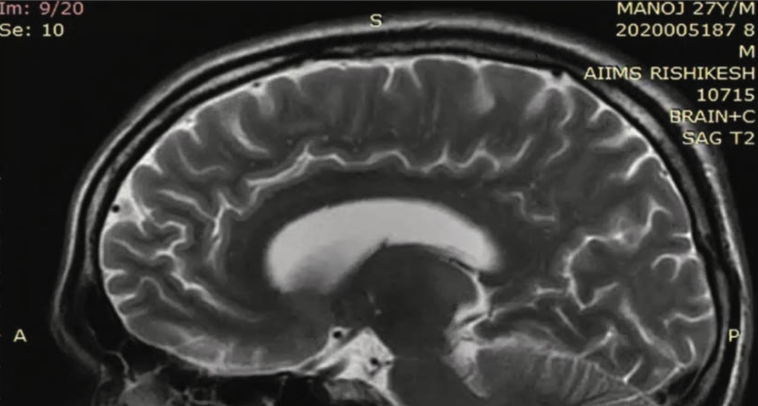
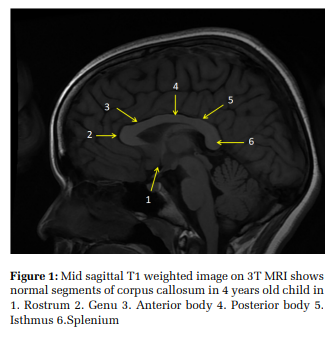
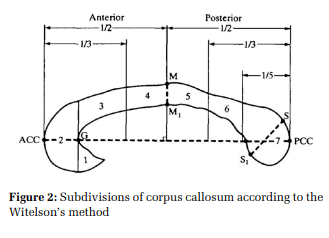
The development was evaluated by a pediatrician on four domains, gross motor, fine motor, social and language milestones. A detailed developmental history was taken in a pre-designed proforma. Children who were unable to gain the age appropriate developmental milestones were considered as having a DD which was performed using Denver Developmental Screening Test II (DDSTII). The cases and comparison groups were imaged using 3 Tesla MRI (GE Signa Pioneer). Routine sequencing (T1, T2, Flair axial, T1 sagittal, diffusion weighted imaging and SWI axial) were used for imaging. Figure 1 depicts mid sagittal T1 weighted image, which were used to measure the thickness of CC (in millimeters) in its various segments according to Witelson’s method as depicted in Figure 2. [15]
The anterior corpus collosum (ACC) and posterior corpus callosum (PCC) (Figure 2) indicate the anterior most and posterior most parts of the corpus callosum. M and M1 are the superior and inferior points of the mid-point of corpus callosum. S and S1 are the superior and inferior points on the splenium and G is the anterior most point on the inner convexity of CC. The dotted lines and solid lines divide the CC in to seven parts: rostrum, genu, rostral body, anterior midbody, posterior midbody, isthmus and splenium
IBM Statistical Package for Social Sciences (SPSS) (22 IBM, New York, USA) was used for analysis of data. The measurements were expressed as mean and standard deviation. The association between the mean sizes of the different regions of CC among the cases and comparison groups was assessed using student t-test. Also the associations between the different types of delays with thinning of CC were assessed using student t-test.
Institutional ethics committee approval was obtained for the study. Informed consent from the parents was obtained as the participants enrolled for the study were aged less than 5 years. Parents of children presenting with developmental delays were approached for enrollment into cases group. Parents of children who underwent MRI for other conditions were approached for enrollment in comparison group.
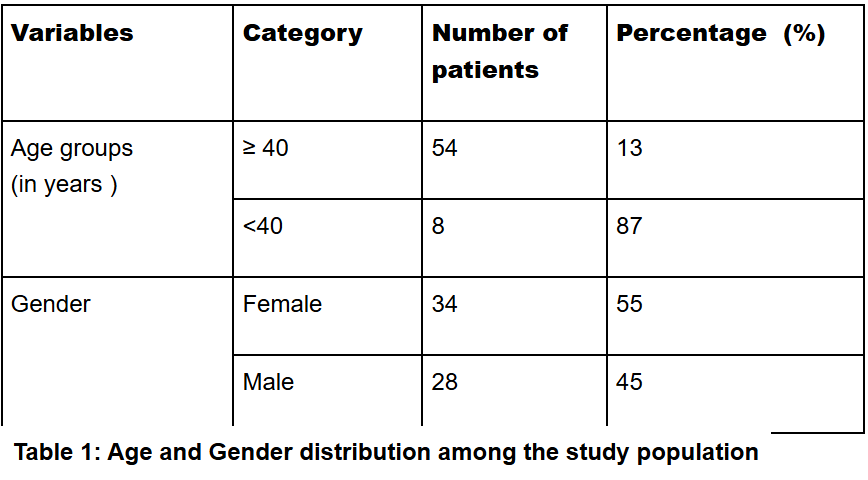
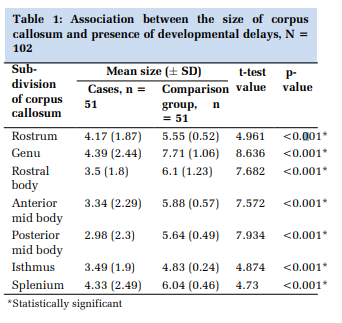
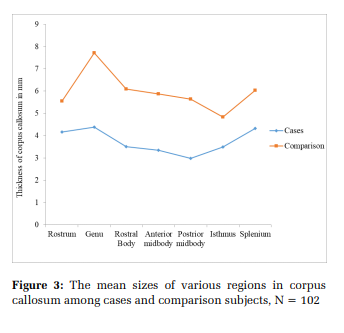
A total of 102 children were included in the study, 51 each in case and control groups. Mean age of the children was 2.9 (±1.24) years. Among the study participants, 56 (55%) were male children. Figure 3 depicts the mean sizes of various areas of CC among cases and comparison subjects. The association between the mean values of sizes of CC among cases and comparison subjects were analyzed and it was found that the difference in the sizes of various subdivisions of CC was statistically significant (p<0.001). (Table 1)
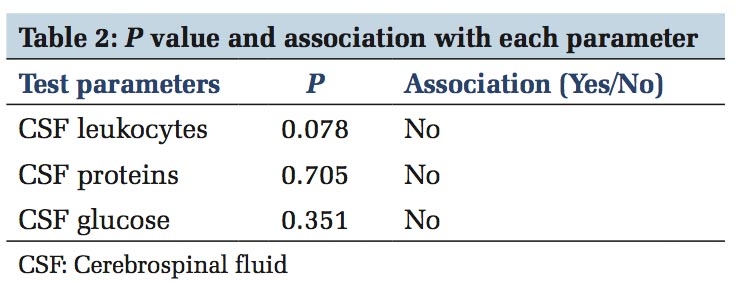
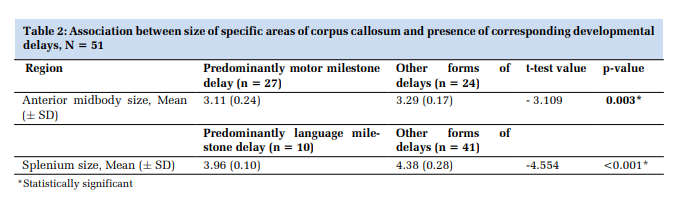
The thickness of specific regions of CC was analyzed for the association with specific delays. The associations between the size of anterior midbody and splenium with motor milestone delay and language milestone delay were found to be statistically significant (p<0.05). (Table 2)
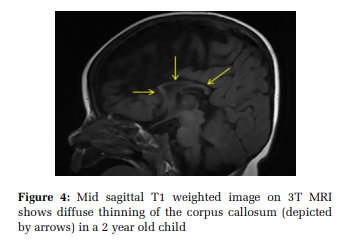
In this study, we analyzed the difference in the sizes of various regions of corpus callosum among children with developmental delays and without delays. The sizes of various regions of CC were found to be lower among the cases than among the comparison and these differences was found to be statistically significant. Figure 4 represents the diffuse thinning of corpus callosum.
It is known fact that the thickness of the CC correlates with the cerebral white matter volume and hence, estimation of CC can help the radiologists to estimate the extent of volume loss in cases of children with peri-ventricular white matter injuries. And also, reduced volume of white matter in the brain is associated with DDs.[16] A study conducted by Ng WHA et al among Chinese school-going children to correlate between the size of the CC with academic performance concluded that mathematical skills and language may be related to general morphometry of CC.[17]
Different set of fibres pass through various regions of CC. The motor neurons predominantly pass through the anterior midbody. [15] Similarly, the speech and language related neurons are related to the splenium of CC. [18] Reduced thickness of CC in anterior midbody was associated with motor developmental delay in our study. Similar findings were observed in a Chinese study conducted by Chang CL et al, where the thickness of CC was positively associated with the ‘rolling over’ milestone of the babies. [6] Another study by Rademaker KJ et al to determine the association between CC and motor performance among prematurely born children in a population cohort found that the mean cross-sectional area of CC was significantly smaller among children born preterm compared to the term babies. The study concluded that among the children who were prematurely born and followed up for 7-8 years of age, larger CC, posterior region in particular was strongly associated with better motor functions. [19]
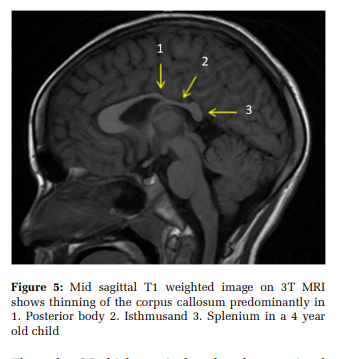
The difference in the means of splenium was compared among cases who had language milestone delay and others was found to be statistically significant indicating that the size of splenium could be associated with the language development. In a study conducted by Northon GB et al, the inter-hemispheric connectivity was correlated with language impairment among adolescents who were born preterm. It was found that there was significant reduction in the volume of the white matter in the region of splenium among individuals with language impairments. [18] Similarly a systematic review conducted by Stipdonk et al found that oral language skills and verbal fluency were strongly related to volume of CC. [20] (Figure 5)
Thus, the CC thickness is found to be associated with the various delays in the attainment of developmental milestones. However, the routine workups for developmental delays do not consider screening of CC. Also, the incidental findings of thin CC necessitate evaluation of the child for presence of developmental delays.
The strengths of our study are that it was a novel idea to correlate the size of CC with developmental delay and cases and comparison groups were used for the same. Two regions of CC were analyzed with the specific type of delay based on the neurons that passed through them. Limitations of the study can be that the metabolic conditions like phenylketonuria/ maple syrup urine disease etc. that can be associated with developmental delays are not considered in this study. Also, a bigger sample size/ a multi-centric study would have provided more comprehensive results and hence, the study findings are not generalisable.
In our study, we have found that the decrease in the size of CC was associated with the developmental delays among children. The decrease in the size of anterior midbody and splenium regions were associated with motor milestone delay and language milestone delay respectively. The children with thin CC need evaluation for developmental delays.
Technological advancement in the field of medical sciences has reformed educational quality, promoting adaptive and collaborative learning by the students and the teachers. We are of the opinion that e-learning plays a powerful role in education, but it cannot be a replace the traditional face-to-face offline/classroom learning. A complete shift to digital learning is a bit tricky. However, we cannot ignore the benefits derived from e-learning. There is a need to understand the hardship that come in the way of online teaching & learning and take appropriate measures to overcome those in view of delivering a good quality education to students.
We thank all the teachers who have participated in this study.
Subscribe now for latest articles and news.