Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.274
Year: 2026, Volume: 12, Issue: 2, Pages: 171-177
Original Article
Mayuri Gogoi 1, Lahari Saikia 2, Vaishali Sarma 3, Supriya Sona 4
1Associate Professor, Department of Microbiology, Jorhat Medical College and Hospital, Barbheta, Jorhat, Assam785001, India.
2Professor and Head of Department, Department of Microbiology, Nagaon Medical College and Hospital, Dipholu, Nagaon, Assam-782003, India.
3Assistant Professor, Department of Microbiology, Gauhati Medical College and Hospital, Bhangagarh, Guwahati, Kamrup (M), Assam-781032, India.
4Assistant Professor, Department of Microbiology, State Cancer Institute (Annexe of Gauhati Medical College and Hospital), Bhangagarh, Guwahati, Assam-781032, India.
Address for correspondence: Mayuri Gogoi, Associate Professor, Department of Microbiology, Jorhat Medical College and Hospital, Barbheta, Jorhat, Assam-785001, India.
E-mail: [email protected]
Received Date:09 September 2025, Accepted Date:22 May 2026, Published Date:12 June 2026
Leptospirosis is an emerging zoonoses which can present with varied clinical manifestations ranging from mild self-limiting illness to severe disease with multi-organ involvement. Objective: The present study was undertaken to determine the seroprevalence of leptospirosis among patients presenting with febrile illness and to determine the involvement of hepato-renal system in the sero-positive cases with respect to the age groups. Methods: A retrospective study was carried out in patients with febrile illness attending Gauhati Medical College and Hospital over a period of three years from Jan 2019 to Dec 2022. The laboratory data relating to the testing for leptospira IgM ELISA were collected. From all the leptospira IgM ELISA positive cases, the information on demographic, clinical and laboratory parameters were recorded. Results: Sero-prevalence of leptospirosis was found to be 27.9% (151/541). The seropositivity was higher in males as compared to females which was statistically significant. Majority of the patients i.e., 58.9% (89/151) were in the age group of 15-40 years followed by 40-60 years age group (48/151, 31.7%). Fever was the most common presentation seen in 65/71 (91.5%) cases followed by jaundice in 51 /71 (71.8%). Hepato-renal dysfunction was seen in 64.2% (97/151) of the sero-positive patients, majority being in the 15-40 years age group (32.4%) followed by 40-60 years group (24.5%). Conclusion: Leptospirosis along with hepato-renal dysfunction is more common in the working age group with a predominance toward male. Hence the laboratory parameters need to be monitored, and timely intervention should be taken to reduce the mortality and morbidity.
Leptospirosis is emerging as an important public health problem in India[1, 2]. It is a direct zoonotic disease caused by different pathogenic species of the genus Leptospira. Different animals may act as carriers or vectors. Human infection occurs due to accidental contact with carrier animals or environment contaminated with leptospires. The primary source of leptospires is the excreta of animals whose renal tubules excrete the leptopspires into the environment with the urine[3]. Humans are infected by contact with rat urine, especially during paddy cultivation. Increasing numbers
of cases are however being reported in the recent times from urban and semi-urban areas as well due to overcrowding, flooding, and poor sanitation issues which provide an environment favorable for the transmission of leptospirosis[4].
Leptospirosis presents with a wide spectrum of clinical presentations. While most patients present only with mild fever and recover without complications, a small proportion of them may develop various complications due to involvement of multiple organ systems[5].
Incidence of leptospirosis ranges between 10- 100/1,00,000 cases per year in developing countries. As per the estimates, India should report 0.1-1.0 million cases per year. However, cases reported is considerably less, which are around 10,000 cases per year[6]. Leptospirosis is a diagnostic challenge because of its protean manifestations and elusive features. It is a disease easily treatable by antibiotic therapy but if left untreated, may prove to be fatal[7].
Hepatic involvement in leptospirosis is not an uncommon feature and can vary from asymptomatic rise in transaminases to severe icteric hepatitis. However, detailed studies on the frequency, degree and type of hepatic involvement in leptospirosis are limited[8].
Though anicteric leptospirosis is the most common form of the disease affecting nearly 90 percent of the patients, severe form of leptospirosis involving kidney and liver known as Weil’s disease is also seen in some patients which has a very high mortality[9].
In India, where an eco-system with inter dependence of humans and animals sharing the same source of food, water and shelter exists, there is abundant opportunity for cross-infection from animals to humans[10]. Some important predisposing factors for this infection include heavy rainfall, animal rearing practices, unplanned urbanization and agrarian way of life[5]. This study was therefore undertaken to determine the sero-prevalence of leptospirosis and the hepato-renal involvement among the seropositive leptospirosis cases with respect to the age groups.
The present study was a retrospective observational study period of three years between January 2019, and December 2021 carried out in the department of Microbiology, GMCH. The registries of the leptospirosis patients were reviewed and the information on demographic, clinical profile and laboratory parameters of the leptospirosis patients was recorded in a well- structured proforma.
Approval to conduct this study was obtained from the Institutional Ethics Committee bearing No MC/190/2007/Pt-II/Oct-2022/3 dated 27/01/2023. Informed written consent was taken from all the study subjects (format enclosed).
During this period, the microbiology laboratory received serum samples from suspected cases with febrile illness for leptospira serology. Serum samples were tested for qualitative determination of specific anti-leptospira IgM antibody using the PanBio IgM ELISA (Panbio diagnostics, Brisbane, Australia) and J.Mitra IgM ELISA. Initially PanBio IgM kits were used but later due to unavailability of this kit, J.Mitra IgM Kits were used. Both the kits use Indirect ELISA technique. The test procedure was performed according to manufacturer’s instructions. With the Panbio IgM kit results were interpreted as Panbio Units. If Panbio units >11 it was considered positive. Sensitivity and Specificity of Panbio IgM kit is 96.5% and 98.5% respectively. Similarly for the J. Mitra IgM kits, Lepto IgM units are calculated and if it is >11 it is considered positive. Sensitivity and Specificity of J.Mitra IgM kit is 99.62% and 99.92% respectively. Negative controls, positive controls and calibrators were kept with each test run.
Statistical analysis:
Data generated from the present study have been presented in the form of tables and all descriptive analyses have been shown in percentages. P value has been calculated to analyze statistical significance.
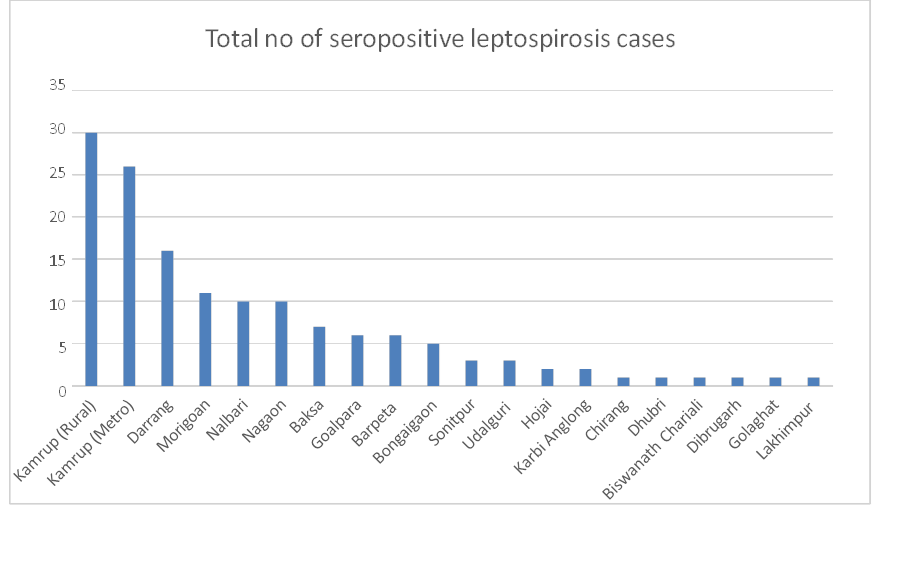
A total of 541 patients were included in the present study. Of these 541 patients, 27.9% (151/541) were seropositive for anti-leptospira specific immunoglobulin (IgM) antibodies. Among these 151 patients, 76.8% (116/151) were males and 23.1% (35/151) were females and the male to female ratio was 3.3:1 [Table. 2]. The age ranged from 4 to 80 years with a mean age of 37.4 years and median value of 35 years. Of the total 151, 143 (95.3%) were adults and 7 (4.6%) were children ≤15 years of age. Only 6 (3.9%) cases were seen in children less than 15 years old [Table. 1]. The district wise distribution showed that majority of the cases were from Kamrup (Rural) 30/151 followed by Kamrup (Metro) 26/151 [Fig. 1].
| Age | Total number of samples tested for Leptospira IgM ELISA | Total number of leptospira sero-positive cases | Leptospira sero- positive cases with hepato-renal dysfunction | Leptospira sero-positive cases without hepato-renal dysfunction |
|---|---|---|---|---|
| <15 years | 26 | 6 | 3 | 1 |
| 15-40 years | 296 | 89 | 49 | 3 |
| 40-60 years | 163 | 48 | 37 | 0 |
| >60 years | 56 | 8 | 8 | 0 |
| TOTAL | 541 | 151 | 97 | 4 |
| Sex of the patient | Total number of samples tested for Leptospira IgM ELISA | Total number of leptospira sero- positive cases | Total number of leptospira sero- positive cases with hepato-renal dysfunction |
|---|---|---|---|
| Male | 354 | 116 | 82 |
| Female | 187 | 35 | 15 |
| TOTAL | 541 | 151 | 97 |
| Clinical feature | Total number of patients showing the symptom |
|---|---|
| Fever | 65 |
| Jaundice | 51 |
| Oliguria, difficulty in passing urine | 28 |
| Headache | 2 |
| Abdominal pain | 2 |
| Abdominal swelling | 3 |
| Generalised weakness | 2 |
| Cough | 4 |
| Haematemesis | 2 |
| Seizures | 2 |
| Loss of consciousness | 1 |
History of exposure to risk factors like exposure to pets and people living in flood affected areas were taken via telephonic conversation with the patients. History could be elicited from 65 patients. In 43/65 (66.1%) cases history of exposure to risk factors was present and in 22/65 (33.8%) no such history was found.
Occupation history was available from 62 patients. Out of the 62 patients, 19 (30.6%) were farmers followed by house-wife (10/62) and students (9/62).
Data on clinical presentation were available from 71 patients. Fever was the most common presentation seen in 65/71 (91.5%) cases followed by jaundice in 51/71 (71.8%) and features of renal involvement 28/71(39.4%). Other less common features were headache, myalgia, cough, abdominal pain and abdominal swelling. The duration of fever was less than 7 days in 47/65 cases and more than 7 days in 18/65 cases [Table. 3]. However, scoring on the basis of the Modified Faine’s criteria was not done in this study.
Laboratory parameters of the leptospira sero-positive cases were also studied. Hyperbilirubinema was noted in 103 sero-positive patients, out of which 80 patients had Grade IV hyperbilirubinemia. Direct bilirubin (>0.2mg/dl) was elevated in 90 sero-positive cases. The mean values of liver enzymes AST and ALT were found to be 197.25U/L and 159.85U/L respectively. Liver enzymes (AST, ALT) were elevated in 108 patients. The mean Blood urea and creatinine levels were 183mg/dl and 4.4mg/dl respectively. Blood urea was elevated (>40mg/dl) in 98 sero-positive patients. The creatinine levels were elevated (>1.3mg/dl) in 104 patients, out of which 45 patients had creatinine levels more than 5mg/dl. The mean leucocyte count was 1.5X 103 cells/mm3, leucocytosis was seen in 85 patients. Hepato-renal dysfunction was seen in 64.2% (97/151) of the leptospira sero-positive cases. Mean haemoglobin and platelet count were 10.41g/dl and 125 X 1000/mm3 respectively. Anaemia and thrombocytopenia were seen in 118 and 97 sero-positive patients respectively. The C-Reactive Protein was elevated in 57/59 cases. Pancreatic involvement in the form of elevated amylase in 6 patients and elevated lipase in 9 patients was also seen [Table. 4].
On enquiring about the patient outcome, information could be obtained from 57 patients. 15/57 patients expired; 35 patients recovered. However, 7 patients had developed renal impairment following leptospirosis and had to undergo dialysis.
Leptospirosis is a frequently under-diagnosed infection because of its varied manifestations and difficulty in distinguishing it from other febrile illnesses. Failure to provide timely diagnosis of leptospirosis cases may lead to unnoticed cases developing acute fatal illness[11]. Our study describes the seroprevalence along the detailed analysis of the abnormalities in the hepatic, renal function parameters in patients with leptospirosis.
The seroprevalence of leptospirosis was found to be 27.9%. In a study done by Kalita et al from Northeast India in the year 2008, the prevalence was found to be 22.57%[12]. From these findings it is evident that there has been an increase in the seroprevalence of leptospirosis in our part of the country which may be due to the better availability of diagnostic tests and also because of episodes of floods in the monsoon season along with urban waterlogging. In a 10- year study done by Chaudhuryet al. from northern India, the seroprevalence of leptospirosis was reported to be 26.90 %[13]. The sero-positivity rate of leptospirosis as per studies conducted from other parts of the country ranges from 17.8–40.5%[14].
| Liver Function test parameter | Abnormality | Total number of leptospira sero-positive cases | Total number of sero-positive cases with records available |
|---|---|---|---|
|
Total bilirubin |
Hyperbilirubinaemia |
|
n=115 |
|
Grade I |
6 |
||
|
Grade II |
5 |
||
|
Grade III |
12 |
||
|
Grade IV |
80 |
||
|
Normal range |
12 |
||
|
Direct Bilirubin |
Elevated (>0.2mg/dl) |
90 |
n=109 |
|
Normal range |
19 |
||
| Aspartate aminotransferase |
Elevated (>40U/L) |
|
n=108 |
|
Mild |
54 |
||
|
Moderate |
40 |
||
|
Severe |
5 |
||
| Alanine aminotransferase |
Elevated (>40U/L) |
|
n=108 |
|
Mild |
48 |
||
|
Moderate |
8 |
||
|
Severe |
4 |
||
| Alkaline Phosphatase |
Elevated (>130U/L) |
39 |
n=66 |
|
Normal range |
27 |
||
|
Renal Function test |
|
|
|
|
Blood urea |
Elevated (>40mg/dl) |
98 |
n=117 |
|
Normal range |
19 |
||
|
Creatinine |
Elevated (>1.3mg/dl) |
104 |
n=124 |
|
>1.3 to 5mg/dl |
59 |
||
|
5 to 9 mg/dl |
36 |
||
|
>10mg/dl |
9 |
||
|
White Blood Cell count |
Leucocytosis (>11000/mm3) |
85 |
n=131 |
|
Leucopenia (<3500/mm3) |
6 |
||
|
Normal range |
40 |
||
|
Haemoglobin |
|
|
n=35 |
|
Female |
Anaemia (<12g/dl) |
32 |
|
|
|
Normal range |
3 |
|
|
Male |
Anaemia (<13g/dl) |
86 |
n=116 |
|
Normal range |
30 |
||
|
Platelet count |
Thrombocytopenia |
97 |
n=130 |
|
(<1,50,000) |
|||
|
Thrombocytosis (>4,50,000) |
3 |
||
|
Normal range |
30 |
||
|
Serum Amylase |
Elevated (>140U/L) |
6 |
n=10 |
|
Normal range |
4 |
||
|
Serum Lipase |
Elevated (>160U/L) |
9 |
n=10 |
|
Normal range |
1 |
In the present study, hepato-renal dysfunction was seen in 64.2% (97/151) of the leptospira sero-positive cases, majority of which belonged to the 15-40 years age group (32.4%) i.e. in the young population followed by 40-60 years group (24.5%). A significant correlation was found between age of the patients and hepatorenal dysfunction (p value is 0.028). The higher number of hepato-renal dysfunction in the 15-40 years age group could be due to the fact that majority of leptospira sero-positive cases were detected in this age group in this study i.e., 58.9% (89/151) were in the age group of 15-40 years. Such clustering of the cases in the age group of 20-40 years has been observed by many other studies[5, 12, 15-19]. The reason for the higher seropositivity in this age group can be explained by the fact that they contribute the majority of the outdoor working population. And since this disease affects the productive age group, this has lot of economic burden both on the family and society[20].
In a study done by Goyal et al, hepatic dysfunction was present in 72.5% patients[8]. Various other studies are shown varying degrees of hepatic and renal involvement in leptospirosis patients[5, 21-23]. The mean serum bilirubin in the present study was 14.6 mg/dl, which is similar to that reported in previous studies[5, 8, 24]. The mean serum transaminases values in our study were similar to that reported by Sethi et al. but higher than those reported by Clerke et al. [40-50 U/L][5, 24]. The creatinine levels were elevated in 104 patients, out of which 45 patients had creatinine levels more than 5mg/dl. Seven patients developed renal failure and had to undergo dialysis. Pancreatic involvement was seen in nine patients with elevated amylase/lipase levels.
The male to female ratio was found to be 3.3:1. Males were found to be at higher risk of being seroreactive than females (P value = .00053). This finding is consistent with various other studies where the prevalence was found to be higher in males[12, 13, 15, 16, 25]. This may be generally attributed to men being more involved in agricultural and animal husbandry related activities, as animals are the major sources of infection for humans.
Majority of the leptospirosis patients were farmers (30.6%) and history of exposure to risk factors like animal exposure, living in flood affected areas could be elicited from 66.1% patients. Also, the sero-prevalence of leptospirosis was found to be more the rural districts. Similar findings were reported by some studies where the prevalence of leptospirosis was found to be more in rural areas[5, 8, 25]. However, the prevalence of leptospirosis was found to be more in urban areas as reported by Shukla et al.[26]
Fever was the most common presentation seen in 65/71 (91.5%) cases followed by jaundice in 51/71 (71.8%). These findings are similar to studies done by Kanan et al., Agarwal et al. and Mandal et al.[14, 27, 28]
On analyzing the haematological parameters, leucocytosis was seen in 64.8% (85/131) of the patients. Leptospirosis being a bacterial infection, leukocytosis with neutrophilia is seen[29]. Anaemia and thrombocytopenia were seen 78.1% (118/151) and 74.6% (97/130) of the sero-positive patients respectively. The thrombocytopenia was significant in patients with leptospirosis in this study, which is observed in various Indian studies as well[23, 30].
Leptospirosis is an emerging zoonosis. It affects mainly the working-age group with a predominance toward male thus having a major economic impact on the family and the country. Hepato-renal dysfunction in leptospirosis is common and especially more so in the younger age groups leading to long term complications. The increased awareness among physicians of protean clinical manifestations of leptospirosis, effective monitoring of the laboratory parameters along with timely intervention can reduce the mortality and morbidity associated with the disease.
Limitations of the study: Paired sera were not used for Leptospira IgM ELISA testing which could have given better results. Also scoring as per the Modified Faine’s Criteria was not done as the detailed clinical history was not available from all sero-positive cases.
Funding: No funding sources
Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee.
1. Leptospirosis on the horizon. <I>National Medical Journal of India</I>. 2000; 13 Available from: https://nmji.in/nmji/archives/Volume-13/issue-5/editorials-2.pdf
2. Leptospirosis, India: report of the investigation of a post-cyclone outbreak in Orissa, November 1999. Weekly Epidemiological Record. 2000; 75 (27). Available from: https://iris.who.int/handle/10665/231209
3. Leptospirosis: an emerging global public health problem. Journal of Biosciences. 2008; 33 (4). Available from: https://doi.org/10.1007/s12038-008-0074-z
4. Seroprevalence of leptospirosis in an endemic mixed urban and semi-urban setting—A community-based study in the district of Colombo, Sri Lanka. PLOS Neglected Tropical Diseases. 2020; 14 (5). Available from: https://doi.org/10.1371/journal.pntd.0008309
5. Increasing Trends of Leptospirosis in Northern India: A Clinico-Epidemiological Study. PLoS Neglected Tropical Diseases. 2010; 4 (1). Available from: https://doi.org/10.1371/journal.pntd.0000579
6. Leptospirosis - current scenario in India. API Medicine Update. 2008; 18 Available from: https://doi.org/10.13140/2.1.4905.6968
7. World Health Organization. <I>Report of the brainstorming meeting on leptospirosis prevention and control</I>. Mumbai: WHO; 2006.
8. Hepatic dysfunction and predictors of mortality in Leptospirosis. Tropical Gastroenterology. 2016; 37 (4). Available from: https://doi.org/10.7869/tg.369
9. Kormanova E. On clinical and therapeutic aspects of icterohemorrhagic leptospirosis (Vasil'ev-Weil disease). <I>Zh Mikrobiol Epidemiol Immunobiol</I>. 1962;33:58-62.
10. Reservoir hosts of leptospira inadai in India. Revue Scientifique et Technique de l'OIE. 2000; 19 (3). Available from: https://doi.org/10.20506/rst.19.3.1251
11. Leptospirosis: The "mysterious" mimic. Journal of Emergencies, Trauma, and Shock. 2008; 1 (1). Available from: https://doi.org/10.4103/0974-2700.40573
12. Leptospirosis among patients with pyrexia of unknown origin in a hospital in Guwahati, Assam. Indian Journal of Public Health. 2008; 52 (2). Available from: https://pubmed.ncbi.nlm.nih.gov/19125541/
13. Serological and molecular approaches for diagnosis of leptospirosis in a tertiary care hospital in north India: a 10-year study. Indian Journal of Medical Research. 2013; 137 (4). Available from: https://pubmed.ncbi.nlm.nih.gov/23703348/
14. Leptospirosis in northern India: a clinical and serological study. Southeast Asian Journal of Tropical Medicine and Public Health. 2003; 34 Available from: https://pubmed.ncbi.nlm.nih.gov/15115094/
15. Seroepidemiological Study of Leptospirosis among Clinically Suspected Cases. International Journal of Current Microbiology and Applied Sciences. 2017; 6 (3). Available from: https://doi.org/10.20546/ijcmas.2017.603.015
16. Aravind GN, Prashanth VN. Clinical profile of leptospirosis. <I>International Journal of Clinical Cases and Investigation</I>. 2015;6:3-24.
17. Seroprevalence of leptospirosis among febrile patients: a hospital-based study. Journal of Academia and Industrial Research. 2015; 3 (10). Available from: https://jairjp.com/MARCH%202015/05%20SAHIRA.pdf
18. An outbreak of leptospirosis in Orissa, India: the importance of surveillance. Tropical Medicine & International Health. 2004; 9 (9). Available from: https://doi.org/10.1111/j.1365-3156.2004.01293.x
19. Clinicolaboratory profile of leptospirosis: Observations from a tertiary care hospital. Journal of Applied Hematology. 2020; 11 (3). Available from: https://doi.org/10.4103/joah.joah_11_20
20. Anos potenciais de vida perdidos e custos hospitalares da leptospirose no Brasil. Revista de Saúde Pública. 2011; 45 (6). Available from: https://doi.org/10.1590/s0034-89102011005000070
21. An outbreak of leptospirosis in Mumbai. Indian Journal of Medical Microbiology. 2002; 20 (3). Available from: https://doi.org/10.1016/s0255-0857(21)03249-7
22. Leptospirosis in Madras: a clinical and serological study. Journal of the Association of Physicians of India. 1995; 43 (7). Available from: https://pubmed.ncbi.nlm.nih.gov/8713215/
23. Leptospirosis: an institutional experience. <I>Journal of the Indian Medical Association</I>. 2011; 109 Available from: https://pubmed.ncbi.nlm.nih.gov/22482321/
24. Clinical profile of leptospirosis from Gujarat. Journal of Postgraduate Medicine. 2002; 48 Available from: https://pubmed.ncbi.nlm.nih.gov/12215693/
25. Decreasing trend of seroprevalence of leptospirosis at All India Institute of Medical Sciences New Delhi: 2014–2018. Journal of Family Medicine and Primary Care. 2018; 7 (6). Available from: https://doi.org/10.4103/jfmpc.jfmpc_198_18
26. Leptospirosis in central and eastern Uttar Pradesh, an underreported disease: a prospective cross-sectional study. Indian Journal of Medical Research. 2022; 155 (1). Available from: https://doi.org/10.4103/ijmr.ijmr_1811_19
27. Clinical profile and prognostic factors of leptospirosis: a study of 50 cases from North Kerala, India. International Journal of Research in Medical Sciences. 2017; 5 (11). Available from: https://doi.org/10.18203/2320-6012.ijrms20174921
28. Serologic evidence of human leptospirosis in and around Kolkata, India: A clinico–epidemiological study. Asian Pacific Journal of Tropical Medicine. 2011; 4 (12). Available from: https://doi.org/10.1016/s1995-7645(11)60234-4
29. Changes in full blood count parameters in leptospirosis: a prospective study. International Archives of Medicine. 2014; 7 (1). Available from: https://doi.org/10.1186/1755-7682-7-31
30. Clinical, biochemical and haematological changes in leptospirosis. International Journal of Research in Medical Sciences. 2018; 7 (1). Available from: https://doi.org/10.18203/2320-6012.ijrms20185381
Subscribe now for latest articles and news.