Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.53
Year: 2026, Volume: 12, Issue: 2, Pages: 166-170
Original Article
Phalguni Srimani 1, Mithu Paul 2, Shukchand Hansda 3
1Associate Professor, Department of Anatomy, Calcutta National Medical College, 32, Gorachand Road, Kolkata – 700014, West Bengal, India.
2Assistant Professor, Department of Anatomy, Midnapore Medical College, Paschim Midnapore, West Bengal, India.
3Assistant Professor, Department of Anatomy, IPGME & R, Kolkata, West Bengal, India.
Address for correspondence: Phalguni Srimani, Associate Professor, Department of Anatomy, Calcutta National Medical College, 32, Gorachand Road, Kolkata – 700014, West Bengal, India.
E-mail: [email protected]
Received Date:10 February 2025, Accepted Date:13 March 2026, Published Date:18 May 2026
Background: Asterion is an important craniometric point in norma lateralis which often exhibit interpopulation variations. A precise understanding of morphology and exact location of such sutural pattern which might serve as superficial projection of different deep-seated structures of brain is pertinent to preoperative planning, operative procedure and post operative outcome during neurosurgical procedures into cranial fossae. Considering the recent interest, the present study was attempted to observe the details of asterion as sutural confluences along with its clinico-anatomical correlation in eastern Indian population.
Methods: 62 adult skulls of both sides were examined. Morphological variations of the sutural patterns were noted and morphometric details were recorded from adjacent anatomical bony landmarks.
Results: Two types of asterion were identified. In the present study, the commonest variant was Type II asterion as observed among 66.13% sides of total examined skulls. Based on different combinations of distribution of such sutural patterns, skulls were classified into symmetrical and asymmetrical categories. Bilateral symmetry was seen in all types of asterion with Type II variety being most prevalent among 41.93% cases. Asterion was situated 25.87±4.36 mm. posterior and 50.36±4.75 mm postero-superior to corresponding supra-mastoid crest and tip of mastoid process respectively. We observed no statistically significant difference while morphological and morphometric evaluation of both sides were made.
Conclusion: Therefore, evaluation of asterion as extremely variable bony landmark on skull can contribute significant consequences in the field of anthropology, forensic medicine and neurosurgery.
Recent development of neurosurgical interventions has increased the interest for a detailed anatomical knowledge of different important craniometric points like asterion which is an important anatomical bony landmark on postero-lateral aspect of skull at the meeting place of parietal, temporal and occipital bone. It is the sutural junction where lamdoid, occipito-mastoid and parieto-mastoid sutures meet. It is closely related to postero-lateral fontanelle in fetal skull also[1]. Based on the type of bony contact either directly or via a small sutural bone with new centers of ossification appearing to bind other bones, asterion is categorized into two types as Type I and Type II based on presence or absence of sutural bones respectively[2].
Shape and localization of sutural pattern are important as superficial projections of different deep-seated structures of brain which are highly variable and therefore pertinent to preoperative planning, operative procedure and post operative outcome during neurosurgical procedures into cranial fossae[3, 4]. Asterion is thus considered as reference point on skull which is important for invasive surgical approach to posterior cranial fossa since it is internally related to venous structures like transverse and sigmoid sinuses as well as other important neurovascular structures. Its surrounding zone as the mastoid triangle and inion-opisthocranium-asterion triangles are also considered as two important triangles with sexually dimorphic characteristics[5]. Knowledge of precise location of such surgical landmark with possible variations is therefore considered fundamental not only for forensic experts but during surgical approach to cranial cavity to avoid the risk of bleeding, thromboembolism and infections[6].
Considering the recent interest, the present study was attempted to observe the variations related to morphology and relative position of asterion as sutural confluences along with its clinico-anatomical correlations to add an anatomical reference data related to skulls in eastern Indian population.
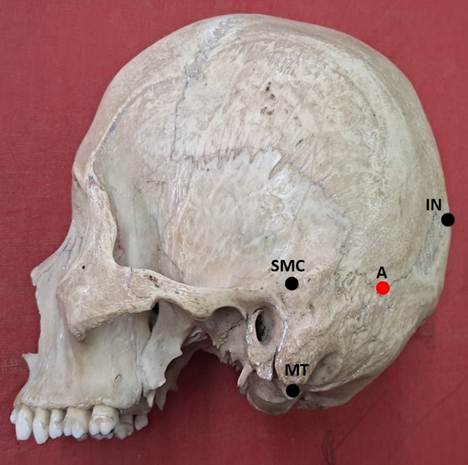
The study was conducted in the Department of Anatomy after taking approval from the institutional ethics committee of Midnapore Medical College, West Bengal (IEC/2024/13), dated 12.06.2024. A total number 62 adult dry skulls of unknown age and gender were studied on both sides and documented carefully with photographs for morphological and morphometric analysis of asterion. In the present study, skulls without any pathology or bony damage or decomposition on areas of interest on both sides were collected based on availability from the department. Depending on morphological characteristics, Type I and Type II asterion were defined in order to be coherent with previous studies[2]. Skulls were also categorized based on either symmetrical or asymmetrical distribution of such sutural pattern on either side. For metric analysis, we observed linear distances between the centre of the asterion and adjacent standard anatomical bony landmarks with digital vernier caliper with an accuracy of 0.01 mm. Three linear measurements were observed on either side to localize asterion [Fig. 1] as follows: i) the distance between centre of asterion (A) and tip of mastoid process (MT) as A-MT, ii) the distance between centre of asterion (A) and centre of supra-mastoid crest (SMC) as A-SMC and iii) the distance between centre of asterion (A) and inion (IN) as A-IN.
All the morphological and morphometric parameters were compared based on side of origin of skulls. Results were statistically analysed using the SPSS software with chi-square and Student’s t-test for categorical and numerical data respectively in which p < 0.05 was considered as statistically significant.
In the present study, 62 skulls were studied bilaterally and following observations were made:
Morphological analysis:
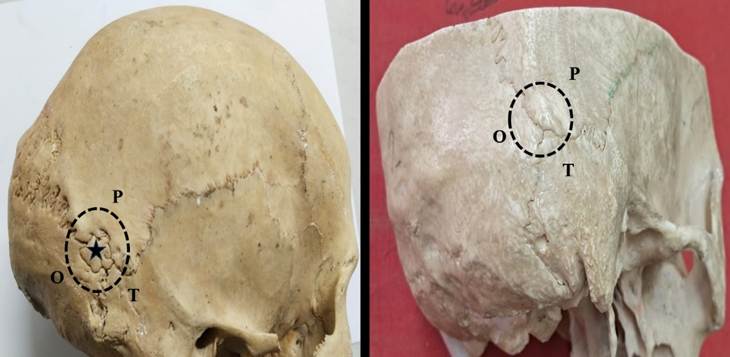
Two types of asterion were documented and depicted in [Fig. 2] as Type I and Type II [Table. 1] of which Type II was the commonest (66.13%) seen on right (32.26%) and left (33.87%) sides as compared to Type I (33.87%) on right -17.74% and left – 16.13% sides.
| Morphological variants | Right side N (%) | Left side N (%) | Total N (%) |
|---|---|---|---|
| Type I | 22 (17.74) | 20 (16.13) | 42 (33.87) |
| Type II | 40 (32.26) | 42 (33.87) | 82 (66.13) |
| Total sides | 62 | 62 | 124 |
No statistically significant difference was observed when such morphological variants were compared between sides (Chi-square value - 0.14, df -1, p = 0.70).
Symmetry of asterion were observed with both types and commonest being Type II as found in 26 skulls (41.93%) whereas Type I was present bilaterally only in 6 skulls (9.68%). Asymmetrical type of asterion was observed in 30 (48.39%) skulls [Table. 2].
| Types of Skulls | Types of asterion | Number of skulls (%) |
|---|---|---|
| Asymmetrical | Type I-Type II or Type II-Type I |
30 (48.39) |
| Symmetrical | Both Type I | 6 (9.68) |
| Both Type II | 26 (41.93) |
Morphometric analysis:
Morphometric evaluation of asterion as linear distances in relation to selected bony reference points on dry skulls like tip of mastoid process, supra mastoid crest and inion are presented in [Table. 3] with corresponding values of mean, standard deviation and range in mm. as derived from data.
|
Morphometric variables
|
Right Mean ±SD (Min-Max) |
Left Mean ±SD (Min-Max) |
Total Mean ±SD (Min-Max) |
p-value |
|---|---|---|---|---|
|
A-MT
|
50.91 ± 4.64 (41.22 – 62.12) |
49.81 ± 4.87 (35.54 – 58.36) |
50.36 ± 4.75 (35.54 – 62.12) |
0.19 |
|
A-SMC
|
25.79 ± 4.40 (17.28 – 34.85) |
25.94 ± 4.39 (16.63 – 34.5) |
25.87 ± 4.36 (16.63 – 34.85) |
0.79 |
|
A-IN
|
62.93 ± 6.17 (53.4 – 87.55) |
62.47 ± 5.26 (54.18 – 81.07) |
62.70 ± 5.69 (53.4 – 87.55) |
0.62 |
On statistical analysis, no significant difference was observed between right and left side in all measurements (p>0.05).
Variation is the rule of God’s creation. Bony surface landmarks on dry skulls are of no exception to this law since their morphology and relative locations are not constant. Accordingly, asterion is considered clinically relevant craniometric points often used as gold standard milestone for intracranial navigation approach to various structures of brain for which researchers have paid much interest to this sutural junction as reference that might enable neurosurgeons to avoid unnecessary risks during surgical maneuvers[7]. Morphogenetic studies have shown development of such sutural pattern in relation to adaptation of skull growth. Role of ethnicity, race, sex and environmental factors are also documented as other determinants for variability of type and location of these landmarks. Ethnic and racial difference could be further due to genetic as MSX2 gene is reported to be involved in the process of articulation of cranial bony segments towards formation of suture[8].
Variation of asterion as a relevant landmark is also important during surgical approach to tympanic cavity, mastoid antrum, membranous labyrinth during transmastoid cisternoscopy as well as approach to cerebellopontine angle[2]. Morphological type of asterion was confirmed in most of the previous studies in terms of Type II being commonest[2, 8-12] which was also consistent with our findings as we observed in 66.13% sides as compared to Type I among 33.87% sides among total examined skulls. Presence of sutural bones in Type I is usually quiescent in nature but may also vary in shape, size and number and prior anatomical knowledge regarding presence of sutural bone within bony confluence thus might avoid pitfalls in radiological diagnosis. These small accessory bones are also found more in number in skulls with hydrocephalus causing rapid cranial expansions[2].
Studies have also shown type of asterion being variable among genders[2]. Additionally, Type I variety was found more common on right side and Type II on left side[6]. In the present study, we observed no statistically significant differences between sides along with presence of both symmetrical as well as asymmetrical distribution of both types. Therefore, such observed variations in the incidences of asterion type might indicate role of epigenetic, embryological and environmental factors across different populations[5].
Knowledge about exact position of asterion is another challenging area for neurosurgeons and considered as safe landmark for retro-sigmoid craniotomy as well as for optimum implant during surgery[13]. It is located behind the auricle as an inappreciable depression at the intersection of lower two-third and upper one-third of auricle. Both traditional and radiological studies have shown variation in position of asterion as reliable external landmark which coincide with Transverse sigmoid sinus venous complex (TSSJ) for dural exposure of posterior cranial fossa with least complications[14, 15]. Also, meningioma occurring at sinus junction can be surgically removed without hazards in postero-lateral surgical approach[13].
Topographic location of asterion is of utmost important to avoid injuries of intracranial neurovascular structures. Studies have shown other bony reference points bearing consistent relationship to asterion and therefore considered to be reliable while attempting intracranial approach[16]. In the present study, we observed linear distance between asterion and corresponding inion was found as 62.70 ±5.69 mm. which differ with other reports as the same distance was noted as less in other study[6] whereas Leon et al.[17] observed it as more. However, the asterion was located 50.36± 4.75 mm. superior to corresponding tip of mastoid process which is comparable to previous study [2, 17, 18]. Author observed symmetrical pattern of location of asterion in both the sides[2] which is also similar to our findings. Further radiological studies also confirmed metric evaluation of asterion which was found in accordance with our observations[19]. However, we did not find any statistically significant differences in metric evaluation of asterion which suggests that surgical approach might be done from these landmarks irrespective of side.
Thus, considerable variation of shape and location of asterion observed across different population might indicate contribution of genetic and environmental factors affecting growth of different bony cranium.
Alteration of type and position of asterion with respect to different anatomical bony landmarks are not infrequent as previously believed. In this study, 2 types of asterion were observed as Type I and Type II among 33.87% and 66.13% sides of total examined skulls respectively. Bilateral symmetry was observed with both types of asterion. Regarding position, asterion was situated 25.87±4.36 mm. posterior and 50.36±4.75 mm postero-superior to corresponding supra-mastoid crest and tip of mastoid process respectively, whereas distance between inion and asterion was 62.70 ± 5.69 mm. Moreover, use of advanced radiological studies have evaluated different craniometric reference points with greater reliability and objectivity which often requires correlations with conventional ones. Accordingly, the present study can be considered as simple and complimentary method in absence of more expensive and sophisticated method employed in radiological analysis. Thus, morphological and morphometric assessment of asterion along with its clinical correlations in present study will definitely add a database to this field which can be evaluated pre-operatively for subsequent safer and more compatible surgical outcome.
Limitations:
As sample size in the present study depends on the availability of skulls in the department, proper sampling methods could not be employed during selection and the maximum number that were available during the study period was considered. The present study did not have any bias for age and gender related changes. Also, we did not get data related to internal morphometry of both craniometric reference points due to lack of availability of open skulls. So, further large scale multicentric studies can be done in future to get a population specific data on asterion.
Acknowledgement:
Authors sincerely thank those who donated the bones to the Department of Anatomy and gave consent to conduct studies for anatomical research purposes. We also acknowledge the great help received from the Department of Anatomy as well as the scholars whose articles are cited.
Funding source:
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest:
Authors declare no conflict of interest.
Authors Contribution:
Srimani P: Conceptualization, Methodology, Data collection, Manuscript writing. Paul M: Data management, Figure editing; Hansda S: Data collection, Manuscript editing; All authors: Approval of final manuscript.
1. Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, Ferguson MW. Gray’s Anatomy: The Anatomical Basis of Medicine and Surgery. 38th ed. London: Churchill Livingstone; 1995. p.583-606.
2. Analysis of the Asterion Morphology in Relation to Its Clinical Significance. International Journal of Morphology. 2023; 41 (6). Available from: https://doi.org/10.4067/s0717-95022023000601744
3. Hossein JM, Jaber G, Forouzan F, Masoud Z, Hosein S. The morphology of the pterion and asterion sutures in Iranian population. European Journal of Anatomy. 2021; 25 (1): 83-88
4. Anatomic Position of the Asterion and Implication for Neurosurgical Procedure. International Journal of Morphology. 2021; 39 (5). Available from: https://doi.org/10.4067/s0717-95022021000501429
5. The relationship between the mastoid triangle and localization of the Asterion. Anatomy. 2021; 15 (3). Available from: https://doi.org/10.2399/ana.21.1053714
6. Morphometric features of asterion in adult human skulls. International Journal of Research in Medical Sciences. 2015; 3 (6). Available from: https://doi.org/10.18203/2320-6012.ijrms20150140
7. Asterion as a surgical landmark for lateral cranial base approaches. Journal of Cranio-Maxillofacial Surgery. 2006; 34 (7). Available from: https://doi.org/10.1016/j.jcms.2006.05.003
8. Incidence of Sutural Bones at Asterion in Adults Indians Skulls. International Journal of Morphology. 2012; 30 (3). Available from: https://doi.org/10.4067/s0717-95022012000300066
9. Sudha R, Sridevi C, Ezhilarasi M. Anatomical variations in the formation of pterion and asterion in south Indian population. International Journal of Current Research and Review. 2013;5(9):92-100
10. Mwachaka PM, Hassanali J, Odula P. Sutural morphology of the pterion and asterion among adult Kenyans. Brazilian Journal of Morphological Sciences. 2009;26(1):4-7
11. Morphological Study on Types of Asterion. International Journal of Integrative Medical Sciences. 2015; 2 (10). Available from: https://doi.org/10.16965/ijims.2015.127
12. Leon SG, Hernandez-Rodri-Guez AN, Morales ÁR, Theriot-Giron MC, Elizondo-Omana RE, Guzman LS. Morphometric characteristics of the asterion and the posterolateral surface of the skull: relationship with dural venous sinuses and neurosurgical importance. Cirugía y Cirujanos. 2013; 81: 269-273.
13. Positioning a Novel Transcutaneous Bone Conduction Hearing Implant: a Systematic Anatomical and Radiological Study to Standardize the Retrosigmoid Approach, Correlating Navigation-guided, and Landmark-based Surgery. Otology & Neurotology. 2018; 39 (4). Available from: https://doi.org/10.1097/mao.0000000000001734
14. Is Asterion a Reliable Surgical Landmark for the Transverse and Sigmoid Sinus Junction in Indian Skulls?. Neurology India. 2023; 71 (4). Available from: https://doi.org/10.4103/0028-3886.383854
15. Anatomical relationship between cranial surface landmarks and venous sinus in posterior cranial fossa using CT angiography. Surgical and Radiologic Anatomy. 2012; 34 (8). Available from: https://doi.org/10.1007/s00276-011-0916-5
16. Evaluation of Asterion Morphometry in Terms of Clinical Anatomy. Eastern Journal Of Medicine. 2019; 24 (4). Available from: https://doi.org/10.5505/ejm.2019.50480
17. Leon SG, Rodriguez AN, Avalos RM, Theriot Giron M, Omana REE, Lopez SG. Morphometric characteristics of the asterion and the posterolateral surface of the skull: relationship with dural venous sinuses and neurosurgical importance. Cirugía y Cirujanos. 2013; 81:251-5.
18. Anatomic structural study of cerebellopontine angle via endoscope. Chinese Medical Journal. 2007; 120 (20). Available from: https://doi.org/10.1097/00029330-200710020-00021
19. Radiographic Evaluation of Mastoid Parameters for Sexual Differentiation in North Indian Population. Cureus. 2021; 14 Available from: https://doi.org/10.7759/cureus.16011
Subscribe now for latest articles and news.