Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.323
Year: 2026, Volume: 12, Issue: 2, Pages: 210-213
Case Report
Shweta Rajpal 1, Shahbaz Patel 2, Ruby Khatoon 2, Jamal Masood 2
1Assistant Professor, Department of Community Medicine and Public Health, King George’s Medical University, Lucknow, U.P, India.
2Department of Community Medicine, Era’s Lucknow Medical College, Era University, Lucknow, U.P, India.
Address for correspondence: Shweta Rajpal, Assistant Professor, Department of Community Medicine and Public Health, King George’s Medical University, Lucknow, U.P, India.
E-mail: [email protected]
Received Date:21 September 2025, Accepted Date:25 February 2026, Published Date:12 June 2026
Twin gestations inherently carry greater perinatal risk, including prematurity, low birth weight, and congenital anomalies. When combined with a diagnosis of congenital hydrocephalus, the clinical scenario becomes especially challenging—particularly in resource-constrained rural settings. This report describes a preterm twin neonate who survived delivery at 30 weeks’ gestation but subsequently developed severe hydrocephalus and profound malnutrition. This patient is currently undergoing multidisciplinary treatment in a tertiary centre. This case highlights the cumulative risks of prematurity, congenital anomalies, malnutrition, and immunisation gaps—each exacerbating child morbidity and mortality in resource-constrained environments and the need for integrated clinical, nutritional, and public health interventions to mitigate adverse trajectories.
Multiple pregnancies are associated with markedly high risks during pregnancy and the neonatal period compared to singleton gestations. These include an increased chance of preterm birth, low birth weight, and birth defects like congenital hydrocephalus [1-3]. Hydrocephalus, which is characterized by excess cerebrospinal fluid within the brain's ventricles, is recognized as a devastating complication—one that further amplifies the risk profile for preterm twins. The inherently shortened gestation of twin pregnancies exposes neonates to the dual threats of organ immaturity and the sequelae of any underlying congenital anomalies [4, 5].
Infants who are born at the edge of survival, particularly twins, are vulnerable not just to immediate perinatal complications but also to chronic health challenges that extend into infancy and beyond [2]. Within these, the coexistence of severe hydrocephalus and malnutrition
represents especially an unfavourable clinical trajectory, as each condition feeds into the other in a cycle of growth failure and neurodevelopmental delay [6]. Rural healthcare disparities, with their attendant barriers to care and nutrition, can further compound these risks.
This report presents a premature twin delivery where the surviving infant in a twin pregnancy developed congenital hydrocephalus and severe acute malnutrition soon after birth. Through this case, the interplay of biological vulnerability and social determinants in shaping outcomes among high-risk neonates is being reported.
A female child was born after a lower-segment caesarean section (LSCS) at 30 weeks' gestation, as part of a twin pregnancy, in a rural health care setting. Weighing 1.08 kg at birth (25th percentile for gestational age), she cried shortly after delivery and registered healthy APGAR scores of 7 and above at both 1 and 5 minutes. Tragically, her co-twin died within the first hours of life, reflecting the acute perinatal hazards associated with prematurity in multiple gestations [1, 2].
The early postnatal period was marked by an absence of breastfeeding within the first hour—an opportunity often missed in low-resource settings. Surviving initial respiratory and metabolic adaptation, the baby required a prolonged two-month stay in a tertiary Neonatal
Intensive Care Unit (NICU) to support stabilisation and further maturation.
At six months, her caregivers noted progressive cranial enlargement [Fig. 1]. Medical evaluation and imaging revealed congenital hydrocephalus, attributed to aqueductal stenosis [Fig. 2]. The child underwent a ventriculoperitoneal shunt surgery [Fig. 1] to relieve raised intracranial pressure. However, over the subsequent months, despite successful shunt placement, she continued to exhibit severe undernutrition.

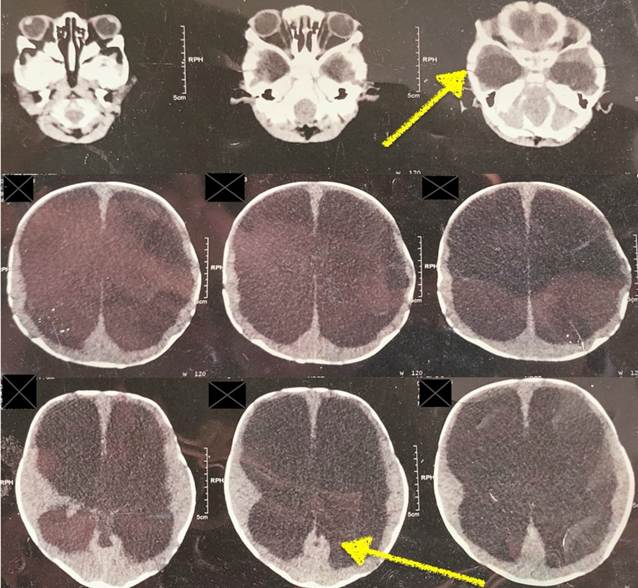
At one year of age, the infant's anthropometric measures showed an evident picture: a weight of 5.8 kg (well below the median of 8.4 kg for age), stunted length at 62 cm (against a median of 72 cm), and a MUAC of only 9 cm—all indicative of severe acute malnutrition per WHO criteria [Table. 1]. Head circumference gradually reduced post-operatively from 51 cm to 47 cm, yet remained above normal, reflecting residual hydrocephalus. Developmental milestones were significantly delayed—likely the cumulative result of prematurity, neurological dysfunction, and nutritional deprivation.
|
Parameter |
Measurement |
WHO Reference |
Interpretation |
|---|---|---|---|
|
Weight |
5.8 kg |
8.4 kg (median) |
Severely Underweight |
|
Length |
62 cm |
72 cm (median) |
Stunting |
|
MUAC |
9 cm |
>12.5 cm |
Severe Malnutrition |
|
Head Circumference (Pre-op) |
51 cm |
~ 47 cm |
Enlarged |
|
Head Circumference (Post-op) |
49 cm |
~ 47 cm |
Improving |
Dietary history revealed exclusive dependence on milk powder beyond the age of six months, with no introduction of appropriate complementary foods, contrary to recommended infant feeding guidelines. Immunisation documentation showed early doses administered [Table. 2], but subsequent critical vaccines—including Rotavirus, PCV, MR and Vitamin A—had been missed, increasing vulnerability to infectious morbidity.
| Vaccine | Status | Comments |
|---|---|---|
| BCG, OPV, Hep B | Given | At Birth (Except Hep B) |
| Pentavalent 1,2,3 | Given | At 6, 10, 14 weeks |
| OPV (Booster) | Not Given | Missed |
| Rotavirus, IPV, PCV | Not Given | Recommended up to 1 year |
| MR-1, JE-1, Vit A | Not Given | Advised for immediate catch-up |
Socioeconomic evaluation placed the family in Class IV under the Modified BG Prasad scale: the father earned a daily wage of approximately Rs. 400, supporting five dependents, with limited access to both healthcare and social safety nets. Though the family successfully registered for the Ayushman Bharat scheme, utilisation of these benefits was minimal.
This case exemplifies the grave compounding of vulnerabilities—prematurity, congenital hydrocephalus, severe malnutrition, and insufficient immunisation—in the context of rural poverty. Each factor, independently a driver of child morbidity and mortality, interacts synergistically in this setting, amplifying the risk to survival and healthy development.
Preterm delivery, especially in twin pregnancies, brings inherent perinatal hazards. Twins often have shorter gestations and more frequent complications due to organ immaturity compared to singletons, resulting in less favourable outcomes, especially when congenital anomalies like hydrocephalus are present [1, 2, 3]. Congenital hydrocephalus, particularly from aqueductal stenosis, poses critical risks: unchecked, it causes progressive intracranial hypertension, developmental delay, and, frequently, early death unless neurosurgical intervention—such as ventriculoperitoneal (VP) shunting—is performed in time. In this case, although shunt surgery was completed, the persistent neurological and nutritional challenges underscored gaps in continuity of care and systemic resource limitations [7].
Severe acute malnutrition (SAM), as reflected by the child's clearly low anthropometric scores (weight, length, and MUAC) which originates from inadequate feeding but also perpetuates a cycle of delayed recovery, repeated infections, and impaired neurodevelopment. Malnutrition directly diminishes immune function, further heightening susceptibility to common and vaccine-preventable illnesses [8]. In infants contending with a neurological disorder, these risks are magnified; up to a third of children with hydrocephalus in similar sub-Saharan settings are malnourished, leading to heightened morbidity and slower recovery [6].
Socioeconomic constraints, such as poverty, low paternal earnings, and large family size, are central to understanding the adverse trajectory in this case. The family's position in BG Prasad Class IV is suggestive of broader social and economic determinants that recur in reports of preventable child deaths in low-resource contexts [9]. Lack of parental awareness, health literacy, limited engagement with social safety nets, and geographic isolation from advanced care facilities make timely intervention difficult.
Immunization gap of PCV, Rotavirus, and MR, vitamin A (all crucial for infection prevention), reflect not only individual oversight but also structural deficits in primary healthcare reach and parental education. Immunization is globally recognized as among the most cost-effective public health tools, yet incomplete coverage remains a persistent problem in rural settings and contributes directly to excess mortality and severe illness in children like the one described here [10].
From a health systems vantage, this case demonstrates the urgent need to reinforce the continuum of antenatal and postnatal care—especially in regions where congenital anomalies, prematurity, and malnutrition converge but diagnostic and referral infrastructure are weak.
In order to address the needs of such patients, a coordinated strategy is essential which include systematic antenatal screening for anomalies, robust community nutrition, feeding programs, and widespread immunization. The role of community health workers and public health teams in early identification and consistent follow-up of at-risk infants cannot be overstated. Only with integrated efforts—melding clinical excellence with social and public health interventions—can similar tragic outcomes be prevented moving forward.
Premature birth in a twin pregnancy, complicated by congenital hydrocephalus and severe malnutrition, presents an extreme challenge in rural and low-resource settings. This case re-emphasises the need for early detection, aggressive nutritional and neurological management, completion of immunisation, and the strengthening of rural public health systems. Moreover, taking care of socioeconomic and educational barriers alongside medical care is crucial to preventing similar tragedies and promoting holistic child health.
Authorship declaration: All authors are in agreement with the content of the manuscript. SR and RK designed the study. SR and SP has primarily collected data for this study. SR wrote the majority of the manuscript. SR, SP, JM, RK contributed to the analysis. SR, SP, JM and RK provided critical feedback and revision on the manuscript. All authors have read and approved the final version of the manuscript.
Declarations of Ethics and Consent to Participate: All the ethical and consent process guidelines have been followed during the publication of this manuscript.
Funding: The authors received no financial support for the research, authorship, and/or publication of this manuscript.
Conflict of Interest: The authors declare that they have no conflict of interest.
1. Pregnancy Complications with Multiple Births. 2024 [cited 2025 Aug 5]. Available from: https://www.babymed.com/medical-issues/what-are-pregnancy-complications-twins
2. Twins vs singletons—Long‐term health outcomes. Acta Obstetricia et Gynecologica Scandinavica. 2023; 102 (8). Available from: https://doi.org/10.1111/aogs.14579
3. Genetics and developmental pathology of twinning. Seminars in Fetal and Neonatal Medicine. 2010; 15 (6). Available from: https://doi.org/10.1016/j.siny.2010.06.002
4. Developmental Outcome Following Posthemorrhagic Hydrocephalus in Preterm Infants. American Journal of Diseases of Children. 1987; 141 (11). Available from: https://doi.org/10.1001/archpedi.1987.04460110040018
5. Hydrocephalus in prematurity: does valve choice make a difference?. Child's Nervous System. 2024; 40 (4). Available from: https://doi.org/10.1007/s00381-023-06204-8
6. High burden of wasting among children under-five with hydrocephalus receiving care at CURE children’s hospital in Uganda: a cross-sectional study. BMC Nutrition. 2024; 10 (1). Available from: https://doi.org/10.1186/s40795-024-00819-z
7. Congenital Hydrocephalus with Aqueductal Stenosis: A Rare Condition Case Report. International Journal of Pharmaceutical Investigation. 2022; 12 (3). Available from: https://doi.org/10.5530/ijpi.2022.3.67
8. Effects of Malnutrition on the Immune System and Infection and the Role of Nutritional Strategies Regarding Improvements in Children’s Health Status: A Literature Review. Nutrients. 2023; 16 (1). Available from: https://doi.org/10.3390/nu16010001
9. Updated BG Prasad’s Socioeconomic Status Classification for the Year 2023. Indian Journal of Community Medicine. 2023; 48 (6). Available from: https://doi.org/10.4103/ijcm.ijcm_401_23
10. Understanding the full-immunization gap in districts of India: a geospatial approach. Clinical Epidemiology and Global Health. 2020; 8 (1). Available from: https://doi.org/10.1016/j.cegh.2019.09.002
Subscribe now for latest articles and news.