Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.336
Year: 2026, Volume: 12, Issue: 2, Pages: 203-205
Case Report
Archana Shetty 1, V Vidhya 2, B N Divyashree 3
1Professor, Department of Pathology, Dr. Chandramma Dayananda Sagar Institute of Medical Education & Research, Dayananda Sagar University, Ramanagara, Karnataka, India.
2Senior Resident, Department of Pathology, Dr. Chandramma Dayananda Sagar Institute of Medical Education & Research, Dayananda Sagar University, Ramanagara, Karnataka, India.
3Associate Professor, Department of Pathology, Dr. Chandramma Dayananda Sagar Institute of Medical Education & Research, Dayananda Sagar University, Ramanagara, Karnataka, India.
Address for correspondence: B N Divyashree, Associate Professor, Department of Pathology, Dr. Chandramma Dayananda Sagar Institute of Medical Education & Research, Dayananda Sagar University, Ramanagara, Karnataka, India.
E-mail: [email protected]
Received Date:06 October 2025, Accepted Date:27 January 2026, Published Date:12 June 2026
Pseudoxanthomatous salpingitis (PXS) is a rare, non-specific inflammatory condition of the fallopian tube, characterized by the presence of hemosiderin-laden macrophages within dilated tubal plicae. We report the case of a 40-year-old woman presenting with lower abdominal pain with imaging features suggestive of bilateral hemorrhagic ovarian cysts and salpingitis. Intraoperative findings revealed extensive pelvic adhesions consistent with stage IV endometriosis. Histopathological examination of the salpinges demonstrated characteristic features of PXS, including hyperplastic plicae, inflammatory infiltrate, and iron-positive pigment-laden macrophages. This unexpected finding prompted additional sampling of ovarian cysts, which revealed foci of endometrial glands and stroma, confirming and supporting the clinical diagnosis of ovarian endometriosis. This case highlights the importance of recognizing PXS as a potential histological clue to underlying endometriosis, particularly when classical features are inconspicuous. Awareness of this rare entity can aid in prompting further tissue evaluation, thereby contributing to accurate diagnosis and appropriate clinical management.
Non neoplastic lesions of the fallopian tube though uncommon can have significant clinical implications including chronic pelvic pain, infertility or mimickers of malignancy. Accurate recognition and diagnosis are essential to guide appropriate management and avoid overtreatment. Pseudoxanthomatous salpingitis (PXS) is one such rare pathological entity characterized by presence of hemosiderin-laden macrophages within the lamina propria of the fallopian tube, with or without associated inflammation. PXS is most commonly associated with ovarian endometriosis, followed by pelvic inflammatory disease, prior radiation therapy, and the use of intrauterine contraceptive devices[1-3].
Grossly, the adnexa may present as a tubo-ovarian mass, with the tubal lumen exhibiting nodular projections. Histopathological examination typically reveals dilated plicae and abundant hemosiderin-laden macrophages within the lamina propria. A closely related condition is xanthomatous salpingitis in which lamina propria is filled with foamy, lipid-laden macrophages along with inflammatory cells. Herein, we report an incidental finding of Pseudoxanthomatous salpingitis which prompted a retrospective, detailed gross and microscopic examination of the submitted ovarian tissue ultimately confirming the presence of coexisting ovarian endometriosis.
A forty year old female presented to the gynecology OPD with complaint of lower abdominal pain since a week. The pain was dull, not localized and had no specific pattern. Ultrasound showed features of bilateral ovarian hemorrhagic cysts and salpingitis with hematosalpinx in both the fallopian tubes. Routine laboratory tests and CA-125 were within normal limits. Intraoperatively, uterus was retroverted and sigmoid colon was adherent to posterior wall of uterus with anterior wall being adherent to anterior abdominal wall. Right tube and
ovary were adherent to each other forming a tubo ovarian mass. Left fallopian tube was adherent to left lateral pelvic wall and omentum and left ovary was adherent to posterior wall of uterus. Uterosacral ligaments were thickened with features suggestive of grade IV endometriosis, under general anesthesia adhesions were released, Methylene blue test was done to rule out any ruptures which showed no staining on gloves, adhesions released followed by hysterectomy and bilateral salpingoophorectomy.
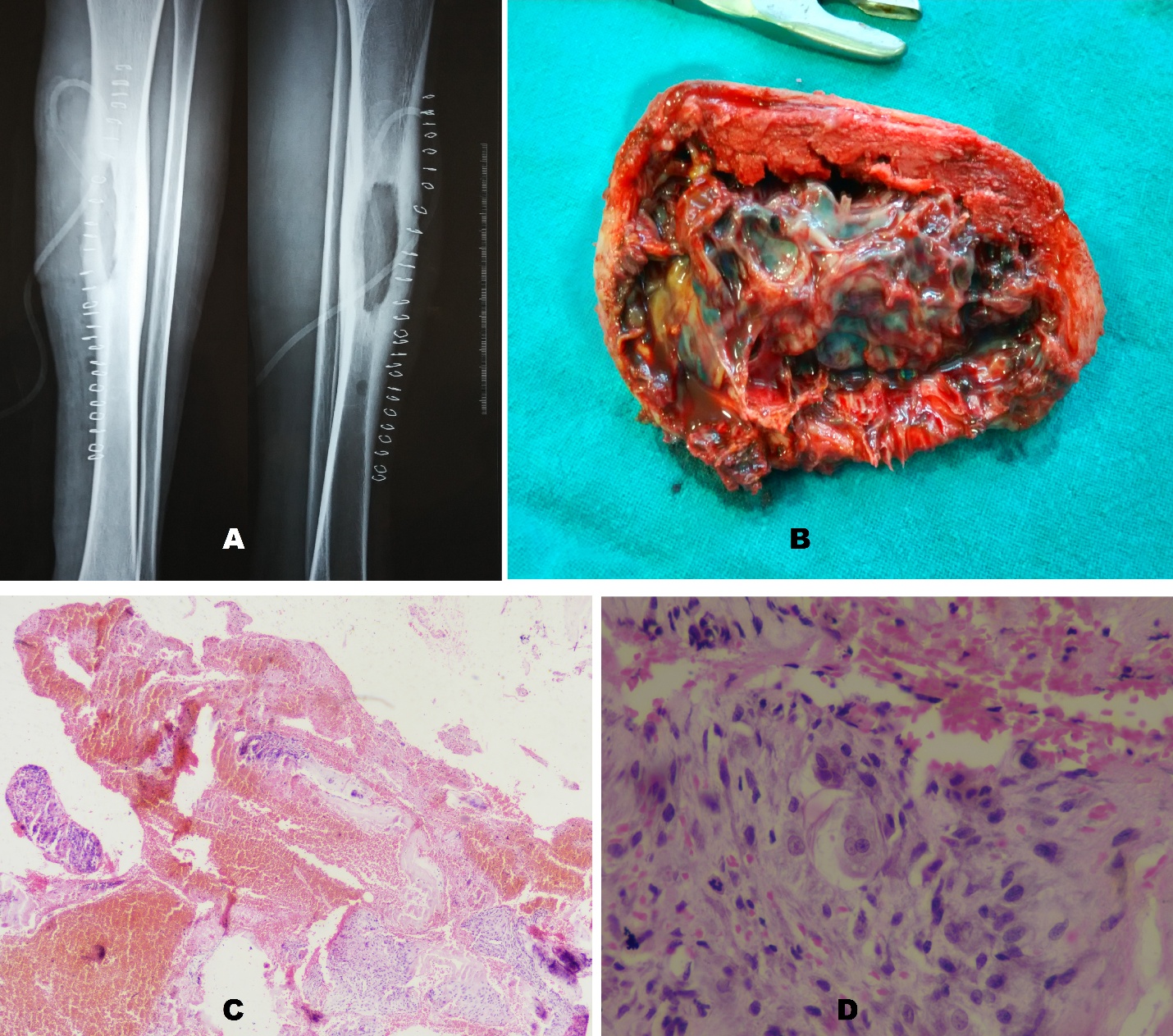
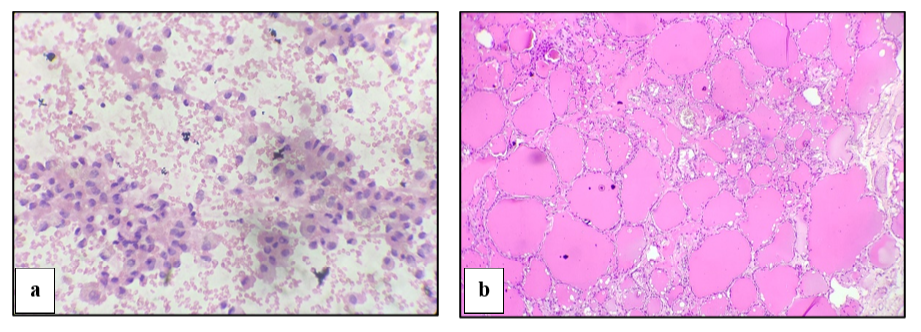
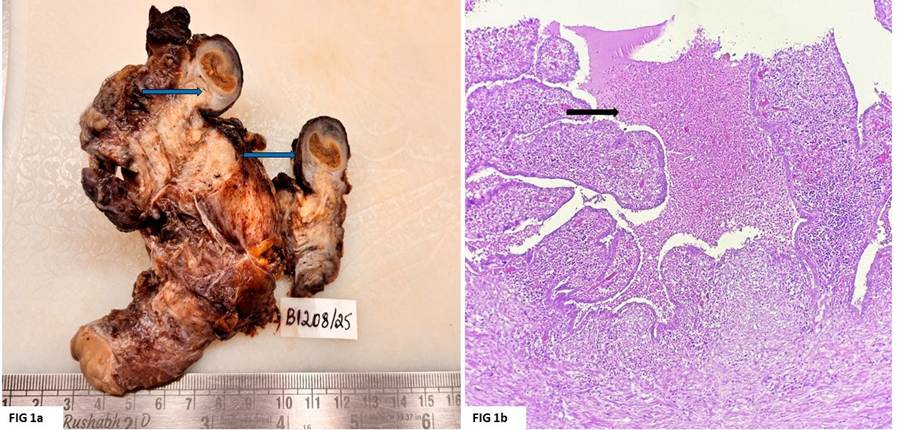
Grossly the specimen of uterus with cervix measured 8 x 4 x 3 cms. Bilateral tubo ovarian masses measured 4 x 3 x 2 cms with tube and ovary being adherent to each other. Cut section of the masses revealed hemorrhagic cysts. Cut sections of both fallopian tubes showed hyperplastic plicae with yellowish discoloration and yellowish brownish material occluding the lumen ([Fig. 1]a).
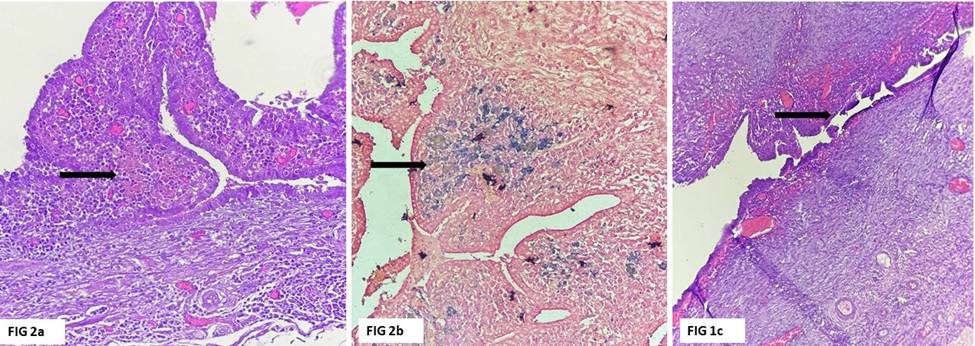
Microscopy of the ovary showed few areas of hemosiderin laden macrophages with hemorrhage and doubtful endometrial stroma. There was diffuse mixed inflammatory infiltrate in the ovarian stroma. Sections from both the fallopian tubes showed dilated plicae with retained architecture and luminal exudate ([Fig. 1]b). Lamina propria showed dense mixed inflammatory infiltrate comprising of lymphocytes, neutrophils and plasma cells. Also seen were good number of brown pigment laden macrophages which stained positive for Perl’s Prussian blue stain : findings suggestive of pseudoxanthomatous salpingitis ([Fig. 2]a & [Fig. 2]b).
This finding led to giving additional bits from the ovarian cysts which revealed foci of broken endometrial glands surrounded by stroma with congested thin walled vessels and hemosiderin laden macrophages ([Fig. 2]c). A final impression of bilateral acute on chronic salpingo ophoritis with ovarian endometriosis and pseudoxanthomaous salpingitis was confirmed. Post-operative course of the patient having been treated for the PID was uneventful and currently is on follow up.
Pseudoxanthomatous salpingitis (PXS) also called as pigmentosis tubae, or melanosis tubae is a rare and histologically distinctive condition of the fallopian tube characterized by presence of pigment laden macrophages filling the lamina propria with or without inflammation. This condition was first described by Herrera et al with only limited number of cases being documented in literature[1]. Etiologies of PXS include ovarian endometriosis, pelvic inflammatory disease (PID), intrauterine contraceptive devices (IUCD) and prior radiation exposure. Among these, the most commonly associated cause is ovarian endometriosis with reflux of hemorrhagic endometriotic material from the ovary into fallopian tubes being the most widely accepted pathophysiological mechanism for the presence of hemosiderin laden macrophages. In endometriosis sloughed off endometrial cells and debris travel retrograde into the fallopian tube. and could possibly be a trigger for initiation of PXS.
Clinical findings in PXS being nonspecific, this entity can mimic adnexal neoplasms radiologically, particularly when associated with adnexal cysts, similar to our case. In our case, ultrasound showed features of bilateral ovarian hemorrhagic cysts and bilateral salpingitis with hematosalpinx. Histopatholoically the hemorrhagic cysts were of the endometriotic type but hematosalpinx proved to be pseudoxanthomatous salpingitis. Radiological findings in PXS are hence non specific[5, 6]. Given its non specific clinical and imaging features, histopathological examination may play a critical role in categorization of tubal lesions. In PXS, grossly the tubal mucosa shows bulbous yellowish luminal projections or only as dilated lumen, as observed by Limaiem and Vaitheesh, et al.[1, 3]. At this stage the other close differential to consider is Xanthogranulomatous salpingitis, (XGS). Microscopically, XGS shows bridging and architectural distortion whereas PXS shows expansion of plicae[2]. Lamina propria in PXS shows pigmented macrophages with or without other inflammatory cells. Accumulated pigment may be hemosiderin, lipofuscin or ceroid deposits. When associated with endometriosis, final degradation product of blood getting accumulated in the cytoplasm of macrophages as hemosiderin is the most accepted pathogenesis[1]. Prussian blue staining can be used to highlight hemosiderin pigment, which helps differentiate endometriosis-associated PXS from XGS or PXS cases unrelated to endometriosis, where this pigment may be absent. In contrast, XGS is characterized histologically by presence of foamy vacuolated histiocytes admixed with inflammatory cells and is most commonly associated with Pelvic Inflammatory Disease (PID)[3].
Studies have demonstrated strong association between presence of PXS and ovarian endometriosis underscoring the importance of documenting this finding in fallopian tube. Seidman and Woodburn in 2015 characterised the pathological findings in cases with PXS and established its close relation with endometriosis with the presence of iron in histiocytes[7, 8]. Recognition of PXS should alert the surgical pathologist to do additional sampling and evaluate for endometriosis, especially in tubo ovarian masses[2]. Our case showed pigment laden macrophages with Perl’s stain positivity confirming the diagnosis of PXS. Additionally, there was an admixture of dense mixed inflammatory infiltrate suggesting the possibility of a coexisting PID. Few authors have proposed that pseudoxanthomatous salpingiosis develops after an episode of acute salpingitis during which actively bleeding ovarian endometriosis leaks blood into the lumen of the fallopian tube, which can be correlated in our case as there was luminal exudate[4].
This case illustrates how identifying pseudoxantho- matous salpingitis through its hallmark hemosiderin-laden macrophages can serve as a histological clue prompting further investigation for underlying pathologies such as endometriosis which may not be evident on gross or initial sampling. Furthermore, these findings also indicate that pelvic inflammatory disease in addition to endometriosis may play a role in the development of psuedoxanthomatous salpingitis.
1. Pseudoxanthomatous salpingitis: An uncommon lesion of the fallopian tube. Clinical Case Reports. 2022; 10 (9). Available from: https://doi.org/10.1002/ccr3.6319
2. Pseudoxanthomatous Salpingitis: A Rare Granulomatous Pathology of the Fallopian Tube. Journal of Human Reproductive Sciences. 2024; 17 (1). Available from: https://doi.org/10.4103/jhrs.jhrs_174_23
3. An unusual case of pseudoxanthomatous salpingitis. International Journal of Research in Medical Sciences. 2024; 12 (9). Available from: https://doi.org/10.18203/2320-6012.ijrms20242633
4. Snyder AN, Crane JS. Histology, Lipofuscin. [Updated 2023 May 1]. In: Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537358.
5. Kostopoulou E, Daponte A, Kallitsaris A, Papamichali R, Kalodimos G, Messinis IE, et al. Xanthogranulomatous salpingitis: report of three cases and comparison with a case of pseudoxanthomatous salpingitis. Clinical and Experimental Obstetrics & Gynecology. 2008;35(4):291-4.
6. Pseudoxanthomatous and Xanthogranulomatous Salpingitis of the Fallopian Tube: A Report of Four Cases and a Literature Review. International Journal of Gynecological Pathology. 2002; 21 (1). Available from: https://doi.org/10.1097/00004347-200201000-00010
7. Endometriosis: A Review of Clinical Diagnosis, Treatment, and Pathogenesis. Cureus. 2022; 14 (9). Available from: https://doi.org/10.7759/cureus.28864
8. Pseudoxanthomatous salpingitis as an ex vivo model of fallopian tube serous carcinogenesis: A clinicopathologic study of 49 cases. International Journal of Gynecological Pathology. 2015; 34 (3). Available from: https://doi.org/10.1097/pgp.0000000000000154
Subscribe now for latest articles and news.