Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.316
Year: 2026, Volume: 12, Issue: 2, Pages: 199-202
Case Report
Thirunavukarasu Thivya 1, V Sriram 2, Govindasamy Revathi 3, Erli Amel Ivan 4
1Post Graduate, Department of Pathology, Sri Manakula Vinayagar Medical college and Hospital, Puducherry, India.
2Professor, Department of Pathology, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India.
3Assistant Professor, Department of Pathology, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India.
4Professor and Head, Department of Pathology, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India.
Address for correspondence: Govindasamy Revathi, Assistant Professor, Department of Pathology, Sri Manakula Vinayagar Medical College and Hospital, Puducherry, India.
E-mail: [email protected]
Received Date:13 September 2025, Accepted Date:27 January 2026, Published Date:12 June 2026
Xanthogranulomatous inflammation is a rare, chronic inflammatory condition that has been reported in various organs, most commonly the kidney and gallbladder. Its occurrence in the female genital tract is uncommon and poses a diagnostic challenge. We report the case of a 37-year-old nulliparous woman who presented with abdominal pain, an elevated CA-125 level, and imaging that revealed a complex right adnexal cyst. Histopathological examination confirmed the diagnosis of xanthogranulomatous salpingo-oophoritis. The presence of coexisting features of salpingitis isthmica nodosa and osseous metaplasia of the ovary makes this case unique.
Xanthogranulomatous inflammation is a rare chronic inflammatory process characterized by the accumulation of lipid-laden macrophages, lymphocytes, plasma cells, and neutrophils, causing tissue destruction and replacement with granulomatous tissue[1]. This condition is commonly reported in various organs such as the kidney, gallbladder, rarely in stomach, bone, urinary bladder, testis and epididymis. Xanthogranulomatous inflammation of the female genital tract is rare and is usually limited to the endometrium. Only a few cases involving both fallopian tube and ovary have been reported in the literature[2]. Due to its local destructive nature and mass-forming capacity due to adhesions, it mimics malignancy both clinically and radiologically, often leading to misdiagnosis and unnecessary extensive
surgical interventions[3]. Hence, awareness of this entity is important to ensure the proper management of the patients. The presence of additional pathological features such as salpingitis isthmica nodosa (SIN) and ovarian osseous metaplasia adds uniqueness to this case.
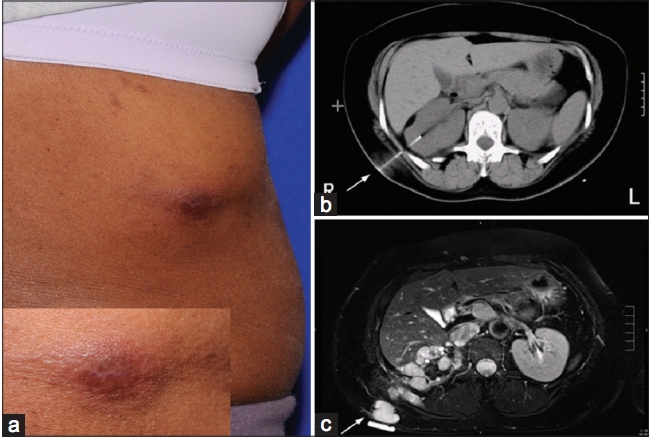
A 37 year old nulliparous women presented to gynaecology outpatient department with complaints of right lower abdominal pain for 2 weeks. Patient also had history of fever for 2 weeks, on and off associated with chills. She had a regular menstrual history. There was no history of any chronic illness like tuberculosis in the past. Per abdominal examination revealed tenderness in the right iliac and hypogastric region. Her per speculum examination showed white discharge with healthy vagina and cervix while per vaginal examination revealed uterus of 14 weeks size. Patient was further investigated and contrast-enhanced MRI of pelvis showed a right complex adnexal cystic lesion of size 9.5 x 6.4 x 11.1 cm with peripheral restriction and thick peripheral, septal post contrast enhancement and right moderate hydroureteronephrosis. Tumor marker CA 125 levels were elevated measuring 94.71 U/ml. With a provisional diagnosis of right complex adnexal cyst, patient underwent laparotomy with bilateral salphingo-oophorectomy and omentectomy.
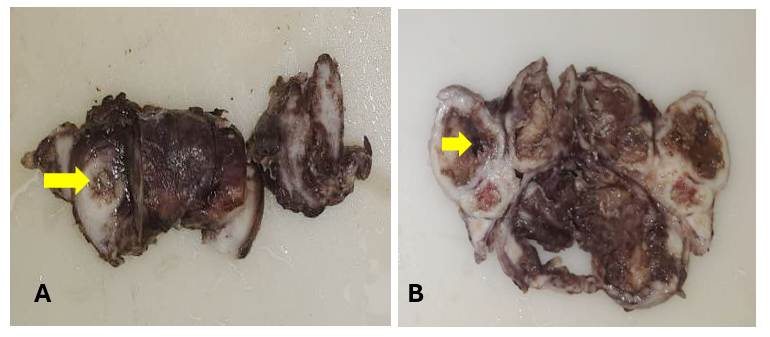
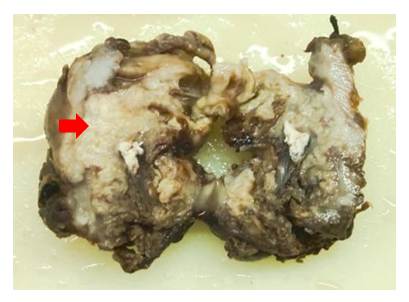
Grossly, right fallopian tube measures 7.5x3x1.5 cm and cut opened right ovarian cystectomy specimen measures 7x6x2 cm. Right fallopian tube was enlarged, congested with cut surface showing a dilated lumen containing grey white friable material ([Fig. 1]A). Right ovary was irregular, congested with focal grey black areas and cut surface showed cystic spaces filled with grey brown friable material. Cyst wall thickness ranged from 0.5 - 0.8 cm ([Fig. 1]B). Left ovary was irregular, congested measuring 5.5x3x2 cm and cut surface showed firm areas with chalky white deposits, bony calcification ([Fig. 2]). Left fallopian tube measures 6 cm was enlarged and congested. Omentectomy specimen was sent in two fragments with congested and inflamed external surface.
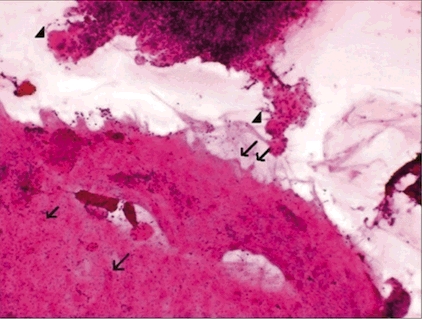
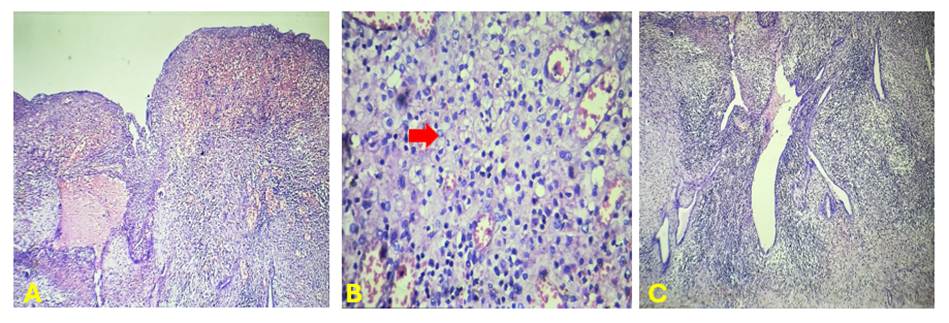
Microscopically, right fallopian tube showed ulcerated, distorted plicae with lamina propria showing dense infiltration of lymphocytes, plasma cells, neutrophils, sheets of foamy histiocytes along with inflammatory granulation tissue. ([Fig. 3] A, B). The muscularis layer showed fibroblastic proliferation, few glands lined by tubal epithelium surrounded by dense lymphoplasmacytic infiltrate, neutrophilic microabscess and foci shows endometrial glands and stroma, suggesting features of Salphingitis Isthmica Nodosa (SIN) and focal endometriosis ([Fig. 3]C).
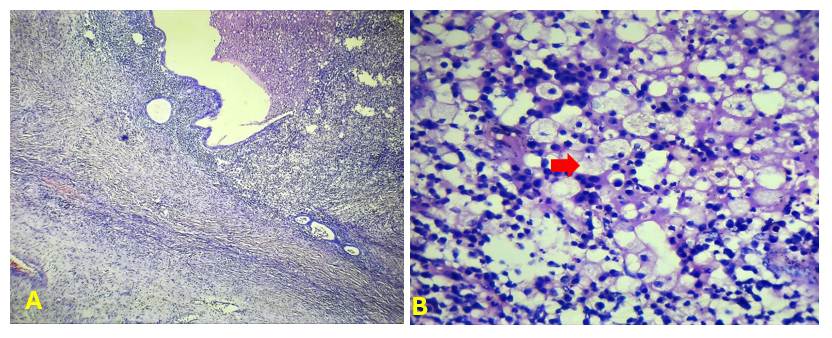
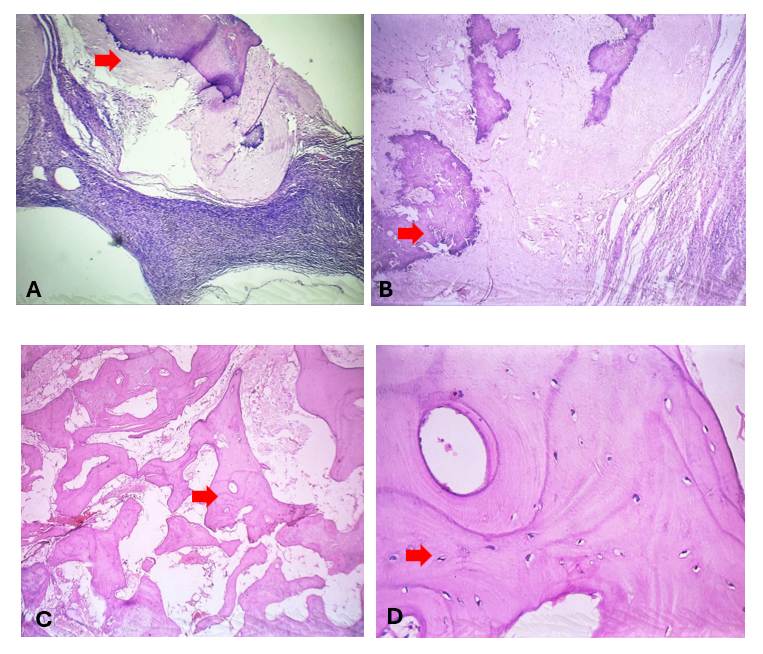
Sections from right ovarian cyst focally lined by columnar to cuboidal epithelium with dense lymphoplasmacytic infiltrates, sheets of foamy macrophages and neutrophilic microabscess. ([Fig. 4]A, B). No evidence of granuloma seen. Special stains PAS and GMS were negative. Hence the diagnosis of Xanthogranulomatous salphingo-oophoritis was given. Sections from left ovary showed chronic inflammatory infiltrates along with calcification and osseous metaplasia ([Fig. 5]A-D). Sections from omentum showed features of acute on chronic inflammation.
Xanthogranulomatous inflammation is an uncommon, non-neoplastic chronic inflammatory condition characterized by the destruction of the affected organ due to extensive infiltration by foamy histiocytes[4]. These are accompanied by multinucleated giant cells, plasma cells, fibroblasts, neutrophils, and areas of necrosis[3]. Xanthogranulomatous inflammation of the female genital tract most commonly involves the endometrium, but it can also affect the fallopian tubes and ovaries[3].
The condition commonly occurs in females of reproductive age group. The exact etiopathogenesis of the disease remains unknown[4]. It is often associated with risk factors such as infections, inappropriate antibiotic use, long-standing pelvic inflammatory disease, endometriosis, intrauterine contraceptive device (IUCD) use, and uterine leiomyomas[4]. The clinical features include history of pelvic inflammatory disease with symptoms of anorexia, fever, menorrhagia, or vaginal bleeding, adnexal tenderness and pelvic mass[5].
It usually presents as a pelvic mass and often misdiagnosed as ovarian neoplasm due to its inflammatory involvement of adjacent organs and the peritoneum, leading to adhesions that further mimic features of malignancy[6]. Hence, gynaecologists need to be aware of this entity. Grossly the affected ovary is enlarged, replaced by a solid yellow tumor-like nodular mass with cystic areas due to liquefactive necrosis. Microscopically, the tissue architecture is replaced by sheets of lipid-laden macrophages or foamy histiocytes admixed with lymphocytes, plasma cells, and neutrophils. Histopathological examination along with immunohistochemistry is essential for the diagnosis. Immunohistochemical markers used are CD8 (foamy histiocytic marker), CD3 (T lymphocyte marker), CD20 (B-lymphocyte marker), and κ and λ (both positive in polyclonal B-lymphocytes)[7].
Non-neoplastic conditions like tuberculosis, malakoplakia, and neoplastic conditions such as lymphoma, leukemia, malignant small cell tumors, and sclerosing stromal tumors, should also be considered in the differential diagnosis[6].
In our case, the patient presented with an adnexal mass and elevated CA-125 levels. Based on the radiological findings, an adnexal cyst was considered, but on subsequent histopathological examination confirmed the diagnosis of Xanthogranulomatous salpingo-oophoritis. Treatment of choice for xantho-granulomatous salphingo-oophoritis is salphingo-oophorectomy[3]. Since this lesion is found to mimic ovarian neoplasm, a preoperative biopsy or frozen section can be planned to avoid such radical surgeries.
Additional interesting findings in our case was the presence of SIN and focal endometriosis in the fallopian tube. The pathogenesis of all these conditions being chronic inflammation possibly explains their co-existence[1]. Another unusual and rare finding is the presence of osseous metaplasia of other ovary, the pathogenesis of which is unclear, but in some circumstances appears to be an unusual reaction to tissue damage and repair[8]. It exists in the context of any ovarian neoplasm or as an incidental finding in grossly normal ovaries and in our case it was found in the other ovary[9].
This case illustrates the diagnostic challenge posed by xanthogranulomatous salpingo-oophoritis and reinforces the need for careful differentiation from malignancy through clinical and imaging correlation in order to avoid any radical surgeries. This case stands out due to the rare and concurrent occurrence of other uncommon pathological features like SIN and osseous metaplasia of ovary.
1. Xanthogranulomatous Inflammation of the Female Genital Tract: Report of Three Cases. Journal of Cancer. 2012; 3 Available from: https://doi.org/10.7150/jca.3929
2. Xanthogranulomatous Salpingooophoritis: The Youngest Documented Case Report. Case Reports in Obstetrics and Gynecology. 2015; 2015 Available from: https://doi.org/10.1155/2015/237250
3. A rare case of xanthogranulomatous oophoritis. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2023; 12 (2). Available from: https://doi.org/10.18203/2320-1770.ijrcog20230146
4. Xanthogranulomatous salpingo-oophoritis mimicking an ovarian malignancy: a clinical dilemma. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2020; 9 (5). Available from: https://doi.org/10.18203/2320-1770.ijrcog20201783
5. Kostopoulou E, Daponte A, Kallitsaris A, Papamichali R, Kalodimos G, Messinis IE, et al. Xanthogranulomatous salpingitis: report of three cases and comparison with a case of pseudoxanthomatous salpingitis. Clinical and Experimental Obstetrics & Gynecology. 2008;35(4):291-4.
6. Rathore R, Chauhan S, Mendiratta S, Sharma R, Nain M, Sarin N. Xantogranulomatous Salpingo Oophritis, Lessons Learnt: Report of Two Cases With Unusual Presentation. Journal of Family and Reproductive Health. 2017 Sep;11(3):174-8.
7. Xanthogranulomatous oophoritis: A case series and literature review. Journal of Medicine, Surgery, and Public Health. 2023; 1 Available from: https://doi.org/10.1016/j.glmedi.2023.100016
8. Osseous metaplasia of ovarian cyst: a rare case report. International Surgery Journal. 2018; 5 (9). Available from: https://doi.org/10.18203/2349-2902.isj20183741
9. RosaSilva JC, Andrade D, Becker AP, dos Reis FJ, Neto OB, Nogueira AA. Isolated osseous ovarian metaplasia: case report. European Journal of Gynaecological Oncology. 2010;31(4):469-70.
Subscribe now for latest articles and news.