Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i3.24.186
Year: 2024, Volume: 10, Issue: 3, Pages: 241-246
Original Article
Navdeep Khangura1 , Sonal Bhati2 , Gunjan Bhatia3 , Namita Goyal4 , Sandeep Kaur Khangura5
1Resident, Department of Pathology, RNT Medical college, Udaipur, Rajasthan, India,
2Associate Professor, Department of Pathology, RNT Medical college, Udaipur, Rajasthan, India,
3Assistant Professor, Department of Pathology, RNT Medical college, Udaipur, Rajasthan, India,
4Senior Professor, Department of Pathology, RNT Medical college, Udaipur, Rajasthan, India, 5GP Registrar, Tamaki Health
Address for correspondence:
Sandeep Kaur Khangura, GP Registrar, Tamaki Health.
E-mail: [email protected]
Received Date:14 June 2024, Accepted Date:27 July 2024, Published Date:21 August 2024
Introduction: Meningiomas are group of mostly benign and commonest non glial tumours. The revised 5th edition of WHO 2021 classification of tumours of the central nervous system categorized meningiomas into single type, with its broad morphological spectrum reflected in 15 subtypes. Aim and Objectives: The main objective of new classification was on grading of tumour along with molecular emphasis. New classification also favoured use of Arabic numerals for grading compared to traditional Roman numerals. The biological behaviour and recurrences are difficult to predict from morphology alone, so Ki-67 Proliferation Index aide in grading of meningioma. The aim of study was to evaluate the histomorphology and grade of meningiomas according to CNS 5th edition classification and correlating the grading and subtyping of meningiomas with Ki-67 Proliferation Index. Materials and methods: This was a cross-sectional observational study of 18 months duration. Sample size included 30 cases. After processing and staining with H and E, cases were classified according to WHO 5th edition classification; Ki-67 staining was done on respective slides and proliferation index was calculated. Results: Our study observed that meningiomas were more common in female population (73.3%) with common age of presentation was 4th and 6th decade of life and the most common subtype being transitional meningioma (46.66%). Majority of cases belonged to CNS WHO grade 1 (86.66%) followed by grade 2 (10%) and grade 3 (3.33%). Average Ki-67 PI for grade 1, grade 2 and grade 3 tumours were 3.57,12.47 and 23.20 respectively. Significant co-relation was found between higher grades of meningioma and Ki-67 Proliferation Index. Conclusion: Histomorphology along with Ki-67 proliferation index is an important diagnostic tool for grading of meningiomas and helps the surgeon in establishing better follow up criteria and long-term management strategies for the benefit of the patient.
Keywords: Meningioma, New WHO classification, Ki-67 Proliferation Index
Meningiomas are the most common primary brain tumour in adults, making 37.6% of all CNS tumours. They are slowly proliferating extra-axial neoplasm of central nervous system, originating from meningothelial cells of arachnoid mater. The likelihood of developing meningiomas escalates with age with common occurrence in fifth and sixth decade of life showing higher prevalence in females. These tumors are rarer in pediatrics population, specifically among those aged 0-19 years. Long term radiation exposure is a significant risk factor 1 . Meningiomas caused by radiation tend to exhibit more aggressive behavior compared to those that occur sporadically 2. The most common site is cerebral convexities. Extracranial metastases (e.g. to lung, bone, and liver) are unusual, and are most often seen in association with CNS WHO grade 3 meningiomas. WHO grade 3 meningiomas also show higher rate of recurrence (50-94%) compared to grade 2 (29-52%) and grade 1 (7-25%). 1
However, the ability to predict biological behaviour and recurrences solely based on morphology is challenging. So, the revised 5th edition of WHO classification of tumors of central nervous system emphasized on combining histology with molecular parameters for layered reporting and integrated diagnosis 3 . Major highlights of new classification are:
Meningioma is considered a single type, with its broad morphological spectrum reflected in 15 subtypes.
Use of Arabic numerals (1, 2, 3, 4) for grading compared to traditional Roman numerals (I, II, III, IV)
The criteria for distinguishing atypical or anaplastic (i.e. grade 2 and 3) meningioma should be uniformly applied irrespective of specific subtype.
The term ‘entity’ has been substituted with ‘type’ and ‘variant’ has been changed to ‘subtype’.
Combined histological and molecular grading.
Mitotic activity is expressed as ‘per mm2’ along with 10 high power fields.
DNA methylation profiling 4 .
In this study, we have classified meningiomas according to new classification along with Ki-67 corelation with grade of tumour. Ki-67 Proliferation Index, most commonly utilised immunohistochemical marker, is expressed during cell cycle proliferative phase. It offers supportive evidence in grading of meningioma on formalin fixed, paraffin embedded sections. Ki-67 is favoured because it requires minimal tissue and works well with standard fixed tissues, playing a significant role in process of oncogenesis 5. Generally, cellular proliferation escalates in correlation with the tumour grade and Ki-67 proliferation index directly reflects this relationship 6. So, by using Ki-67 in addition to morphology help in predicting risk of recurrence.
To study various meningiomas in relation to age and gender.
To classify meningiomas according to WHO 5th edition classification.
To study Ki-67 proliferation index in various subtypes of meningiomas and it’s correlation with grades of meningioma.
Study design: Cross-sectional observational study.
Study period: 18 Months at Department of Pathology, RNT medical college, Udaipur.
Inclusion criteria: Patients of all age groups of meningioma are included in this study.
Exclusion criteria: Recurrent meningioma cases, on therapy cases and poorly preserved specimens were excluded from our study.
Sample size: After ethical clearance, 30 cases were included.
Comprehensive clinical details, along with radiological findings were noted. After processing and staining with H and E, the cases were categorised based on WHO 5th edition classification.
WHO Grade Criteria includes: (these criteria apply to all subtypes of meningioma. However, to classify a meningioma as atypical, it must meet the criteria for CNS WHO grade 2, and for a diagnosis of anaplastic meningioma, CNS WHO grade 3 criteria need to be satisfied. 1 )
CNS WHO grade 2 : 4 to 19 mitotic figures in 10 consecutive HPF of each 0.16 mm2(at least 2.5/mm2) or Unequivocal brain invasion or at least three of the following:
Increased cellularity
Small cells with high N:C ratio
Prominent nucleoli
Sheeting
Foci of spontaneous necrosis
CNS WHO grade 3 : 20 or more mitotic figures in 10 consecutive HPF of each 0.16mm2 (at least 12.5/mm2) or Frank anaplasia or TERT promoter mutation or Homozygous deletion of CDKN2A and/or CDKN2B. 1
IHC staining for Ki-67 was done on respective slides.
The primary antibody (polymer based) used was Ki-67 (MIB-1) monoclonal antibody and the secondary antibody kit was NoVo link polymer on fully automated machine.
Positive and negative controls were employed throughout the staining procedure.
and then, proliferation index was calculated.
Scoring was done by assessing the percentage of tumour cell nuclei that exhibited staining.
Ki-67 proliferation index was determined by examining 1000 nuclei at 400X magnification, with results expressed as percentage of nuclei positively stained. Average ki67 proliferation index was then calculated for each subtype. 7
Data was analysed in the form of tables and percentage.
Total of 30 cases of meningiomas were included in the study. Our study observed that meningiomas were more common in 4th and 6th decade of life with female predominance (73.3%). Majority cases belonging to 41-60yrs (40%), followed by 19-40 years (30%) followed by >61yrs (26.66%).
The convexity of cerebrum (46.66%) was commonest site among all.
Majority of cases belonged to CNS WHO grade 1 (86.66%) followed by grade 2 (10%) and grade 3(3.33%).
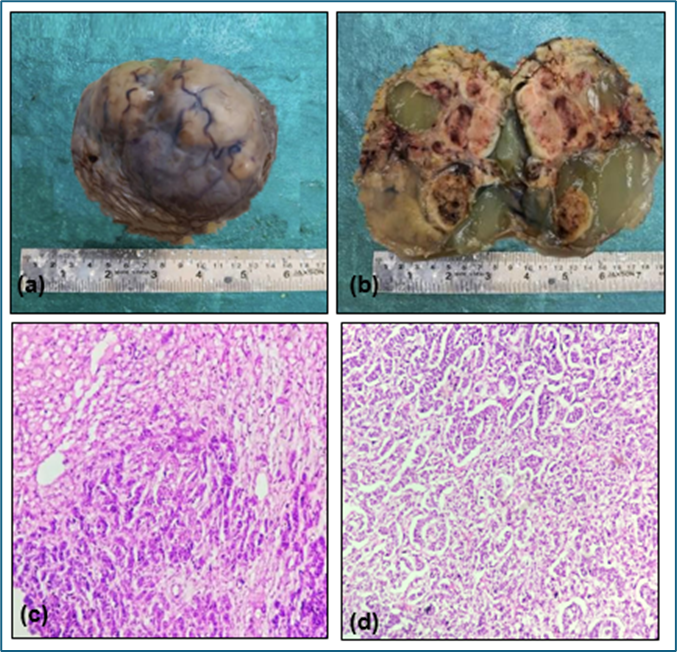
The most common subtype overall being transitional meningioma (46.66%) followed by meningothelial (20%). Figure 1 depicts histopathology image of meningothelial meningioma.
In Grade 2 meningiomas, atypical meningioma constituted 6.66% while clear cell comprised of 3.33% overall. Figure 2 depicts histopathology image of atypical meningioma.
We encountered a case of papillary meningioma, which was classified as a grade 3 meningioma according to new WHO 2021 classification criteria.


Average Ki-67 PI was calculated for each variant.
In grade 1 meningiomas, the transitional subtype demonstrated average Ki-67 proliferation index reaching 4.02. While the most aggressive grade 3 (papillary meningioma) showed highest Ki-67 value, leading at 23.20. Grade 2 atypical meningiomas also displayed significant proliferative activity, evidenced by an average Ki-67 value of 13.95. This data underscores the increasing Ki-67 index with rising tumour grade, reflecting higher proliferative activity in more aggressive forms. Figure 3 depicts histopathology image (a) and Ki-67 staining (b) of grade 3 meningioma.
Overall lowest and highest values were seen in meningothelial (2.90) and papillary meningioma (23.20).
Ki-67 PI displayed minor variation among tumours of same grade, but considerable variation was observed across tumours of different grades. Table 1 summarises Ki-67 Proliferation Index of tumours of different grades.
P value for the Ki-67 PI among grades were calculated using ANOVA, which was <0.001, significant in nature.
Hence, linear correlation of Ki-67 PI to the grade of meningioma was observed.
|
Subtype
|
No of cases
|
Grade of tumour
|
%
|
Average KI-67 PI
|
|
Meningo thelial |
6 |
Grade 1 |
20% |
2.93 |
|
Fibrous |
1 |
Grade 1 |
3.33% |
3.80 |
|
Transitional |
14 |
Grade 1 |
46.66% |
4.02 |
|
Angiomatous |
3 |
Grade 1 |
10% |
3.30 |
|
Microcystic |
1 |
Grade 1 |
3.33% |
3.50 |
|
Secretory |
1 |
Grade 1 |
3.33% |
3.90 |
|
Clear cell |
1 |
Grade 2 |
3.33% |
11.0 |
|
Atypical |
2 |
Grade 2 |
6.66% |
13.95 |
|
Papillary |
1 |
Grade 3 |
3.33% |
23.20 |
|
Total
|
30
|
|
|
|
(%=percentage, PI= Proliferation Index)

Despite their reputation as benign tumours, meningiomas can impair quality of life through focal neurological deficits. Moreover, 20% of cases demonstrate aggressive behaviour, even under optimal standard care 8 . Their biological characteristics present a complex challenge. They can be completely benign, can show atypical features or frankly malignant tumours with increased risk of recurrence and mortality. MRI is recognised as gold standard for diagnosing and monitoring meningiomas. Initial treatment generally involves surgical intervention, with radiotherapy and repeated surgeries being option for recurrent meningioma. Nevertheless, tumour recurrences and progression following surgery are frequent occurrences.
In the present study, 30 cases of meningiomas were studied and classified according to the latest WHO classification 2021. 20 cases of meningiomas were noticed in 4th-6th decade with female predominance. The male to female ratio was found to be 1:2.7. These results were in concordance with the study conducted by Desai et al. 9 , Backer et al. 10 . Studies indicated strong association between hormones and malignancies, possibly due to sex hormone receptors found on tumour cells. Progesterone receptors are found in 80% of women and 34% of men. Research indicates that these receptors actively contribute to tumour growth 11. Paediatric meningiomas are very rare according to many studies, we also encountered only one case of paediatric meningioma in a child of 14 years of age.
Majority of meningioma cases in our study were found in supratentorial in location which is comparable to Shri Lakshmi et al. study. 12 Surgical procedures can be complicated by the location of lesion especially when it is near vital structure. Most common subtype being transitional meningioma (46.66%) followed by meningothelial meningioma (20%). Similar results were recorded in study done by Backer et al. whereas it is different from Shri Lakshmi et al. study where meningothelial meningioma was the commonest overall. Demography variations, race, age, gender, disease incidence, tumour size, location, etc can influence outcomes in various studies.
Our study showed an analogous result with Gadgil et al. 13, with grade 1 (86.66%) being the most common followed by grade 2 (10%) and grade 3 meningioma (3.33%).
Low Ki-67 PI was noted in grade 1 tumours while grade 2 and 3 tumours showed higher Ki-67 PI. Thus, the difference in the Ki-67 index between grade 1 and grade 3 meningiomas fundamentally reflects the underlying biological differences in how these tumours grow and spread, aligning with their histomorphological and clinical characteristics.
The index is a direct measure of fraction of cells in the cell cycle, so a higher proportion of actively dividing cells leads to higher index.
Ki-67 score was low in Grade 1 with only minor difference between the different subtypes i.e. 2.93 being the minimum Ki-67 PI while 4.02 was maximum Ki-67. This minor deviation could be due to different biological behavior of these subtypes as stated by Nowak et al. 14 that in WHO Grade 1 Meningiomas with a Ki-67 value >6% strongly correlated with increased risk of recurrence.
Though there was no significant difference in the Ki-67 PI between histological subtypes within each grade in our study and that is agreement with the observations made by Babu et al. 15.
The average Ki-67 PI in our study showed a statistically significant and linear increase with subsequent grade. Also, correlating linearly with mitotic activity of tumour too.
Similar trends were observed in the study by Rashmi et al. 7 regarding Ki-67 Proliferation index across different tumour grades. Roser et al. 16 reported comparable Ki-67 PI levels in grade 1 tumours, while all 4 studies 7, 16, 17 including ours, showed higher Ki-67 PI in grade 3 tumours.
Variations in Ki-67 interpretation between laboratories occur due to differences in staining techniques used, the antibodies used, and criteria for counting positive cells. Hence, leading to potential differences among Ki-67 proliferation index as illustrated in Table 2.
Although there is a link between the WHO grade of meningioma and its Ki-67 index, Ki-67 is not factored into the WHO’s grading criteria for meningioma.
Therefore, grading of meningiomas along with corelation of Ki-67 index is crucial for clinical decision-making and designing tailored treatment strategies.
Histological grade and extent of tumour excision stand out as pivotal factors in predicting the recurrence and progression of meningiomas. Age at diagnosis is acknowledged as one of most powerful predictors of outcome for patients. Majority of them occur in 4th to 6th decade of life with female predominance. Most fall under CNS WHO grade 1 with transitional meningioma being most common followed by meningothelial meningioma. Ki-67 proliferative index in meningioma increases in proportion with increasing grade. Histomorphology along with Ki-67 proliferation index is an important diagnostic tool for grading of meningiomas and helps the surgeon in establishing better follow up criteria and long-term management strategies for the benefit of the patient. Therefore, Ki-67 PI can be helpful as additional tool to grading system irrespective of subtype of meningioma.
Smaller sample size of our study and unavailability of molecular studies in our institute.
Subscribe now for latest articles and news.