Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.242
Year: 2026, Volume: 12, Issue: 2, Pages: 195-198
Case Report
Mekhala Rao 1, Kalyani Raju 2, Prakash Dave 3
1Senior Resident, Department of Pathology, Sri Devraj Urs Medical College, Kolar, Karnataka, India.
2Professor, Department of Pathology, Sri Devraj Urs Medical College, Kolar, Karnataka, India.
3Professor and HOD, Department of Surgery, Sri Devraj Urs Medical College, Kolar, Karnataka, India.
Address for correspondence: Kalyani Raju, Professor, Department of Pathology, Sri Devraj Urs Medical College, Kolar, Karnataka, India.
E-mail: [email protected]
Received Date:04 July 2025, Accepted Date:04 November 2025, Published Date:12 June 2026
Introduction: Merkel cell carcinoma is a rare and aggressive cutaneous neuroendocrine cancer. The incidence of Merkel cell carcinoma in Caucasians is 0.23 per 100,000. The incidence of MCC in India is not known and only isolate cases of MCC have been identified.
Case report: A 76-year-old female came with the complaints of a painless lesion over the skin in the lower abdomen. On examination there was a single ulcerated nodule over the skin measuring 2x2cm in size. The lesion was excised and was sent for histopathological examination. Grossly, we received a single skin covered soft tissue mass measuring 2.5x2x1.5cm. Externally, skin showed an ulcerative nodule. Cut surface of the nodule showed grey white areas. On microscopic examination, sections showed skin tissue along with a tumor composed of tumor cells arranged in organoid pattern and trabeculae. Individual tumor cells displayed high N:C ratio, round to oval nucleus, salt and pepper chromatin, a few showing prominent nucleoli and moderate amount of eosinophilic cytoplasm. The differential diagnosis on Hematoxylin and eosin stained slides were Merkel cell carcinoma and Amelanotic melanoma. On immunohistochemistry, tumors cells showed cytoplasmic positivity for Synaptophysin and were negative for CK20 and melanoma markers. The final diagnosis offered was Merkel cell carcinoma.
Conclusion: This is a rare presentation of MCC in a non-sun exposed area with CK20 negativity. A diagnosis of MCC should not be missed in case of CK20 negativity and a panel of neuroendocrine markers should also be used to confirm the diagnosis of Merkel cell carcinoma.
Merkel cell carcinoma (MCC) is a rare and aggressive cutaneous neuroendocrine cancer. The incidence of MCC in Caucasians is 0.23 per 100,000.[1] The incidence of MCC in India is not known and only isolate cases of MCC have been identified.[2] It usually affects elderly indivi- duals and occurs in sun exposed areas of skin. MCC was first described by Cyril Toker in 1972.[2] He called it “trabecular carcinoma of the skin”.[3] Tang and Toker first postulated that these tumors might be derived from Merkel cells, which are normally found in the skin.[4]
The cell of origin of MCC is still not known.[5] It is also
known as primary cutaneous neuroendocrine carcinoma.[6] It usually occurs due to UV radiation-induced DNA damage and/or Merkel cell polyomavirus.[1] 80% of the MCCs are due to Merkel cell polyomavirus in the Northern hemisphere. Rest of the MCCs are due to ultraviolet radiation induced DNA damage. Carcinogenesis in these patients involve Rb and p53 tumor suppressor pathways.[5] There is increased risk of MCC in immuno-suppressed individuals.[7]
Complete surgical excision of the primary tumor with adequate surgical margins is the treatment of MCC along with adjuvant radiotherapy. Immunotherapy has significantly changed the standard of care and might significantly change the prognosis. According to the 8th edition of AJCC staging system, the two-year overall survival for stage IV disease is only 26%.[6]
A 76-year-old female came with the complaints of a painless lesion over the skin in the suprapubic area for 3 years. The lesion rapidly increased in size in the last 1 month. On examination there was a single ulcerated nodule over the skin measuring 2x2cm. The ulcer was
1x1cm in size with sloping edges. The nodule was firm to hard in consistency.
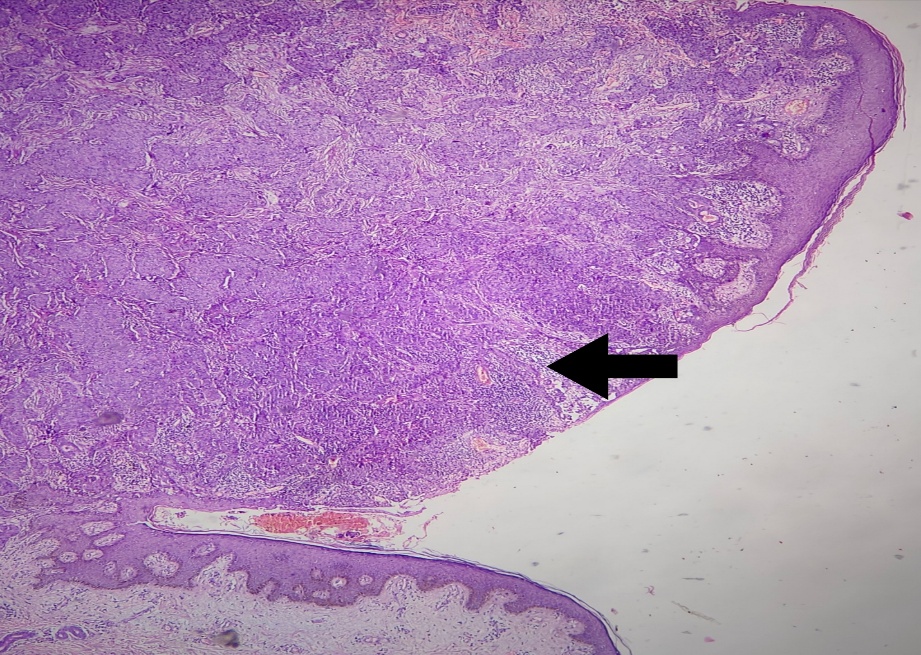
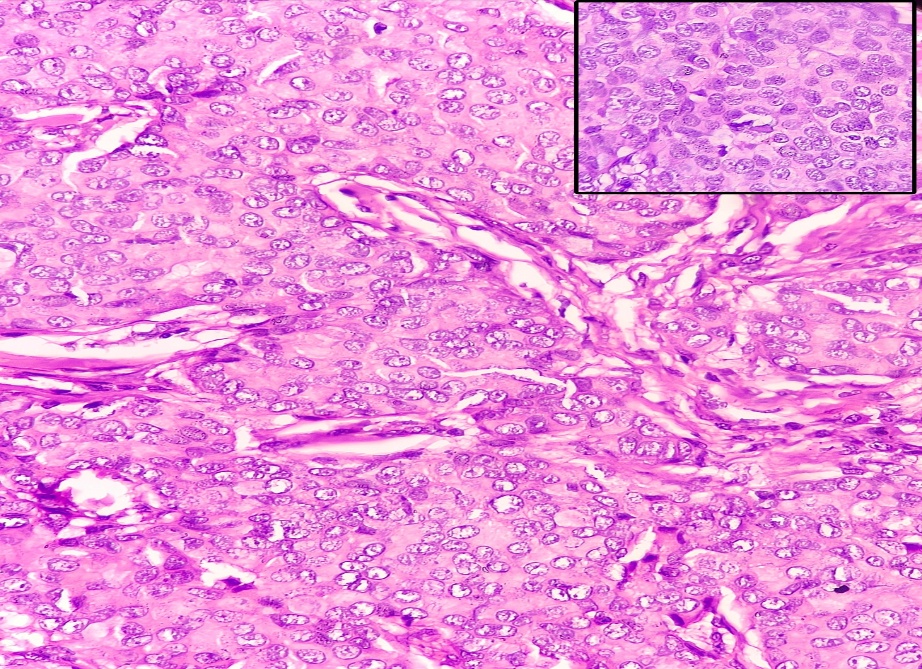
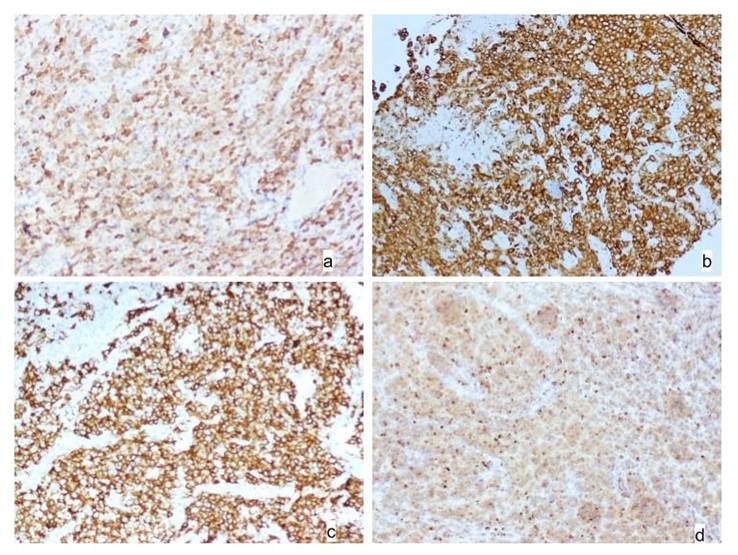
The lesion was excised and was sent for histopathological examination. Grossly, we received a single skin covered soft tissue mass measuring 2.5x2x1.5cm. Externally, skin showed an ulcerative nodule. The cut surface of the nodule showed grey white areas. On microscopic examination, sections showed skin tissue along with a tumor composed of tumor cells arranged in organoid pattern and trabeculae [Fig. 1], [Fig. 2]. Individual tumor cells were round and displayed high N:C ratio, round to oval nucleus, having salt and pepper chromatin, a few showing prominent nucleoli and moderate amount of eosinophilic cytoplasm. The differential diagnosis offered was Merkel cell carcinoma and Amelanotic melanoma.
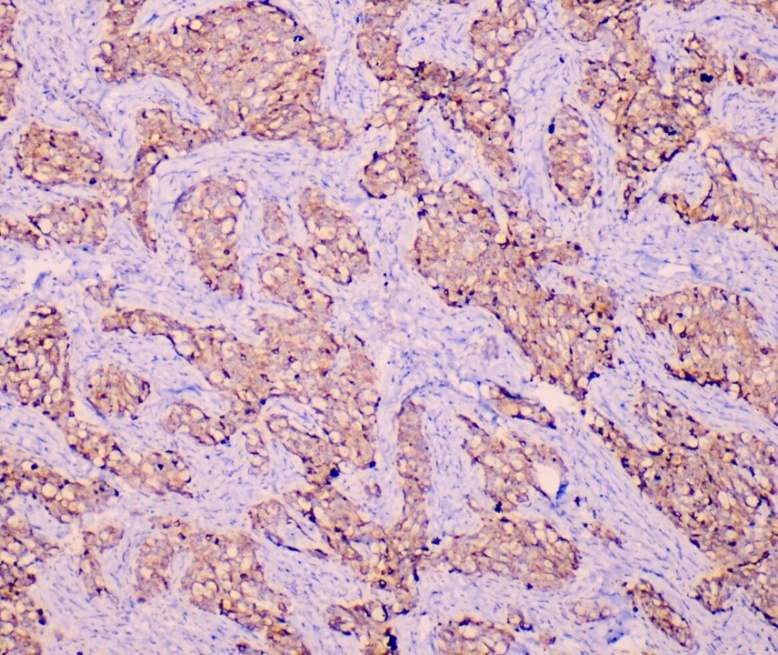
On immunohistochemistry, tumors cells showed diffuse strong cytoplasmic positivity for neuroendocrine marker Synaptophysin [Fig. 3]. Tumor cells also showed diffuse weak cytoplasmic positivity for neuroendocrine marker chromogranin. Tumor cells were negative for cytokeratin 20 (CK 20). The possibility of amelanotic melanoma was ruled out as S100, Melan A, SOX10 and HMB45 were negative on immunohistochemistry. The final diagnosis offered was Merkel cell carcinoma as Synaptophysin was positive and the possibility of metastatic cancer was ruled out as there was no primary tumor elsewhere in the body. The patient was lost to follow up.
MCC occurs mainly among elderly patients over 70 years old.[8] Male gender is considered as a risk factor for MCC.[9] It commonly affects the skin of the head and neck region.[10] MCC frequently presents as a painless, fast-growing red or purple skin nodule.[11] Histologically, MCC can be categorized into three subtypes. The 3 subtypes are trabecular type, intermediate subtype and small cell subtype. The trabecular subtype is the least common and shows tumor cells arranged in organoid pattern, trabeculae and rarely in the form of ribbons. This type of MCC usually occurs next to skin adnexal structures especially hair follicles. The intermediate subtype is the most common histological subtype and is clinically more aggressive than that of tumors of the trabecular type. Tumor cells are less compactly arranged, and the cytoplasm is less abundant when compared to the trabecular type. Mitoses and focal areas of necrosis are frequent. These tumors usually arise next to the adnexa but may invade the epidermis. The small cell type mimics small round cell tumors like small cell neuroendocrine carcinoma.[12] The prognosis of MCC is poor and 44% of the patients have local recurrences. 36% of the patients develop regional lymph node metastasis. Distant metastasis occurs in 40 – 50% of the patients, mostly to the lungs, liver and bone.[12]
MCCs express various cytokeratins on immunohistochemistry. CK20 positivity, being the most diagnostic for MCC, shows a perinuclear dot like positivity. CK7 is usually negative in most cases. They also express neuroendocrine markers like chromogranin and synaptophysin.[14] 95 percent of the patients with this cutaneous cancer express CK20. However, 5% of the patients with MCC fail to express CK20 on immunohistochemistry.[1] When CK20 is negative, at least 1 marker of neuroendocrine differentiation like synaptophysin can be helpful to confirm the neuroendocrine nature of the tumor and to avoid missed diagnoses in the rare CK20-negative MCC.[15]
Our patient was an elderly female with the skin lesion in a non-sun exposed area. The histological subtype in our patient was a trabecular subtype of MCC with the organoid pattern of arrangement of cells. On Hematoxylin and eosin-stained slides, the first differential was MCC in view of the presence of organoid pattern and salt and pepper chromatin. The second differential was amelanotic melanoma in view of the presence of prominent nucleoli in some of the tumor cells. On immunohistochemistry, the possibility of amelanotic melanoma was ruled out and a diagnosis of MCC was made as synaptophysin was positive. However, CK20 was negative in tumor cells. Also, melanoma markers like S100, Melan A, SOX10 and HMB45 were negative.
CK20 negativity is thought to be because of dedifferentiation. It is still not known if CK20 negativity in MCC is associated with difference in prognosis and shows distinct molecular changes when compared to CK20 positive MCC. According to a study by Miner A et al CK20-negative MCC was associated with a low incidence of Merkel cell polyomavirus positivity. MCC associated with polyomavirus and nonviral MCC have huge differences in gene mutation and also have difference in prognosis. Studies have found that patients with MCC detected with antibodies to Merkel cell polyomavirus oncoprotein had a better prognosis.[15]
Surgery is the primary treatment modality for most cases of MCC. Radiotherapy can be used when surgery is contraindicated as MCC is a radiosensitive neoplasm. Radiotherapy alone is inferior to surgical resection because of the risk of distant MCC recurrence. Immunotherapies with PD-1 (programmed cell death 1) and PD-L1 (programmed cell death protein ligand 1) inhibitors is an option in cases of metastasis. According to the 8th edition of the AJCC staging system, the five-year overall survival for the pathological staging of local disease was 62.8% for stage I; 54.6% for stage IIA and 34.8% for stage IIB. The five-year overall survival for stage IIIA was 40.3% and was 26.8% for stage IIIB. In stage IV disease, the two-year survival rate is 26%.[6]
This is a rare presentation of MCC in a non-sun exposed area with the histopathological presence of organoid pattern and salt and pepper chromatin. CK20 negativity was found in tumor cells on immunohistochemistry. A diagnosis of MCC should not be missed in case of CK20 negativity and a panel of neuroendocrine markers should also be used to confirm the diagnosis of Merkel cell carcinoma.
1. Rare but Still There: An Interesting Case of Cytokeratin 20-Negative Merkel Cell Carcinoma. Cureus. 2024; 16 (3). Available from: https://doi.org/10.7759/cureus.55612
2. Merkel Cell Carcinoma: The Past, the Present, and the Future. Journal of Skin Cancer. 2013; 2013 Available from: https://doi.org/10.1155/2013/929364
3. Merkel cell carcinoma. Nature Reviews Disease Primers. 2017; 3 (1). Available from: https://doi.org/10.1038/nrdp.2017.77
4. The Toker Tumor: Spectrum of morphologic features in primary neuroendocrine carcinomas of the skin (Merkel cell carcinoma). Annals of Diagnostic Pathology. 2006; 10 (6). Available from: https://doi.org/10.1016/j.anndiagpath.2006.10.001
5. Merkel cell carcinoma: A review. Journal of Cutaneous Pathology. 2021; 48 (3). Available from: https://doi.org/10.1111/cup.13910
6. Merkel cell carcinoma: epidemiology, clinical features, diagnosis and treatment of a rare disease. Anais Brasileiros de Dermatologia. 2023; 98 (3). Available from: https://doi.org/10.1016/j.abd.2022.09.003
7. Merkel Cell Carcinoma—Update on Diagnosis, Management and Future Perspectives. Cancers. 2022; 15 (1). Available from: https://doi.org/10.3390/cancers15010103
8. Clinical Features and Prognosis of Merkel Cell Carcinoma in Elderly Patients. Medical Science Monitor. 2020; 26 Available from: https://doi.org/10.12659/msm.924570
9. Primary Merkel Cell Carcinoma: A Retrospective Analysis of 31 Cases in Poland. Dermatology and Therapy. 2020; 10 (5). Available from: https://doi.org/10.1007/s13555-020-00424-5
10. Merkel Cell Carcinoma of the Head and Neck: Epidemiology, Pathogenesis, Current State of Treatment and Future Directions. Cancers. 2021; 13 (14). Available from: https://doi.org/10.3390/cancers13143506
11. Merkel Cell Carcinoma Case Reports With Merkel Cell Polyomavirus Test and Review of the Literature. The American Journal of Dermatopathology. 2024; 46 (11). Available from: https://doi.org/10.1097/dad.0000000000002837
12. Merkel cell carcinoma. World Journal of Surgical Oncology. 2006; 4 (1). Available from: https://doi.org/10.1186/1477-7819-4-7
13. A Rare Case of CK20/CK7 Double Negative Merkel Cell Carcinoma. The American Journal of Dermatopathology. 2017; 39 (3). Available from: https://doi.org/10.1097/dad.0000000000000700
14. Merkel Cell Carcinoma. Surgical Pathology Clinics. 2017; 10 (2). Available from: https://doi.org/10.1016/j.path.2017.01.013
15. Cytokeratin 20-negative Merkel cell carcinoma is infrequently associated with the Merkel cell polyomavirus. Modern Pathology. 2015; 28 (4). Available from: https://doi.org/10.1038/modpathol.2014.148
Subscribe now for latest articles and news.