Introduction
Cardiothoracic surgery constitutes a cornerstone of modern surgical practice, addressing a spectrum of complex diseases involving the heart, lungs, and thoracic cavity. The field encompasses a diverse range of interventions, including congenital and acquired cardiac disease correction, pulmonary resections, mediastinal and esophageal surgery, and management of traumatic cardiothoracic injuries. Despite major innovations in technology and perioperative care, traditional surgical principles remain indispensable, particularly when managing high-risk and anatomically complex cases.
Modern cardiothoracic surgery is inherently multidisciplinary, requiring seamless collaboration among surgeons, anaesthesiologists, perfusionists, intensivists, and critical care nurses.
Careful patient selection, interprofessional decision-making, and adherence to evidence based protocols are central to achieving optimal outcomes [1].
Over the past few decades, major advancements in cardiothoracic surgery have transformed the prognosis of conditions once considered inoperable.
These include refinements in cardiopulmonary bypass technology, myocardial protection, minimally invasive and robotic-assisted techniques, and perioperative monitoring. Equally, anaesthesia for cardiothoracic surgery has evolved from basic physiological support to sophisticated intraoperative management aimed at optimizing myocardial performance, oxygen delivery, and postoperative recovery [2]. The role of the anaesthesiologist has expanded beyond intraoperative care to encompass preoperative risk stratification,
perioperative haemodynamic optimization, and postoperative critical care management. Consequently, both surgical and anaesthetic innovations have contributed to substantial reductions in morbidity and mortality following cardiac and thoracic operations worldwide.
Within low- and middle-income countries (LMICs), however, the pace of progress has been constrained by limited resources, infrastructural challenges, and a scarcity of specialized personnel. Nevertheless, the past two decades have witnessed notable strides in establishing sustainable cardiothoracic surgery programs across several parts of sub-Saharan Africa, reflecting a gradual shift toward self-sufficiency and capacity building. Ghana’s journey in this regard is emblematic of such progress. Komfo Anokye Teaching Hospital (KATH) in Kumasi is a major tertiary referral center serving the Ashanti, Ahafo, Bono East, Northern, Northeast, Savannah, Upper East, and Upper West regions. With a bed capacity of approximately 1,200, KATH functions as both a clinical and academic hub affiliated with the School of Medical Sciences, Kwame Nkrumah University of Science and Technology (KNUST) [3]. A landmark event in Ghana’s cardiothoracic history occurred in October 2007, nearly forty-three years after Professor Charles Odamtten Easmon pioneered the country’s first open-heart surgery. A collaborative effort between a team from Boston Children’s Hospital, USA, and KATH marked the first successful open-heart operation in Kumasi, approximately 250 kilometres northwest of the capital city, Accra. This achievement signified the beginning of a new era in cardiothoracic surgery at KATH, laying the foundation for the establishment of a structured and enduring surgical program.
Since then, the programme has undergone substantial development. In 2015, the Cardiovascular and Thoracic Unit was formally inaugurated, integrating three subspecialties: vascular surgery, adult and paediatric cardiac surgery, and thoracic surgery. The unit currently operates under a dedicated team comprising one cardiovascular and thoracic surgeon, one thoracic surgeon, and one cardiothoracic anaesthesiologist. Despite these limited human resources, the team performs elective surgeries twice weekly, in addition to providing 24-hour emergency services for thoracic and vascular conditions. The unit is supported by a dedicated operating theatre, an intensive care unit, an in-house pharmacy, and a general ward, forming a functional ecosystem for comprehensive cardiothoracic care.
The evolution of the cardiothoracic service at KATH has paralleled improvements in surgical outcomes, patient safety, and quality assurance. In alignment with the Institute of Medicine’s framework, quality in healthcare is defined as the degree to which health services increase the likelihood of desired health outcomes consistent with current professional knowledge [4]. Guided by this principle, KATH has progressively implemented structured quality control mechanisms. Since 2015, adherence to a modified perioperative checklist emphasizing infection control, vascular line insertion protocols, and multidisciplinary preoperative briefings has been closely monitored. Such systematic measures have strengthened perioperative safety culture and clinical governance within the unit.
Despite these commendable advances, challenges remain, particularly in sustaining outcomes comparable to high-income settings where advanced infrastructure, specialized training, and access to technology are more readily available. In resource-limited environments such as Ghana, evaluating and understanding outcome trends is critical for continuous improvement. Regular audit and feedback mechanisms allow identification of modifiable factors influencing surgical success, perioperative morbidity, and mortality.
Against this backdrop, the present retrospective review was undertaken to assess the clinical outcomes, anaesthetic practices, and evolving trends in cardiothoracic surgery performed at Komfo Anokye Teaching Hospital over a fifteen-year period. The study analyses perioperative data, complication rates, and mortality patterns while exploring adherence to established bundle care protocols and checklists. By highlighting local innovations, adaptive practices, and the impact of team-based care within a constrained healthcare system, this analysis aims to contribute to the growing body of literature on cardiothoracic surgery in LMICs. Ultimately, the findings are expected to inform strategies for quality improvement, resource allocation, and capacity strengthening in comparable settings, reinforcing the feasibility of delivering safe and effective cardiothoracic surgical care within the West African subregion.
Materials and Methods
This single centre retrospective analysis evaluated consecutive cardiothoracic surgeries performed at Komfo Anokye Teaching Hospital (KATH), Ghana, from October 2007 to September 2022. KATH is the second-largest tertiary academic referral centre in Ghana, with a 1,200-bed capacity. Ethical approval was granted by the KATH Research and Development Unit. The institutional ethics committee approved waiver of individual written consent; data access was authorised by the Directorates of Anaesthesia & Intensive Care and Surgery. All cases were anonymised and assigned a unique computer generated study code. Records with incomplete variables were excluded.
The primary objective was to describe the spectrum of cardiothoracic surgeries performed over the study period and to examine changes in anaesthesia practice around 2014, when evidence informed, resource adapted protocols were introduced. Protocol modifications emphasised early extubation to minimise ventilator associated morbidity, routine tranexamic acid administration to mitigate postoperative bleeding, rational inotrope selection to prevent dysrhythmia and infection control measures.
Thirty-six perioperative clinical variables were extracted from operative, anaesthesia, and intensive care unit charts. Normality of distribution was assessed with the Shapiro–Wilk test. Continuous variables are presented as mean ± Standard deviation (SD) and were compared using Student’s t-test or Mann–Whitney U test, as appropriate. Categorical variables were compared using Fisher’s exact test or χ² test. A two-tailed p < 0.05 was considered statistically significant. All analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA).
Results
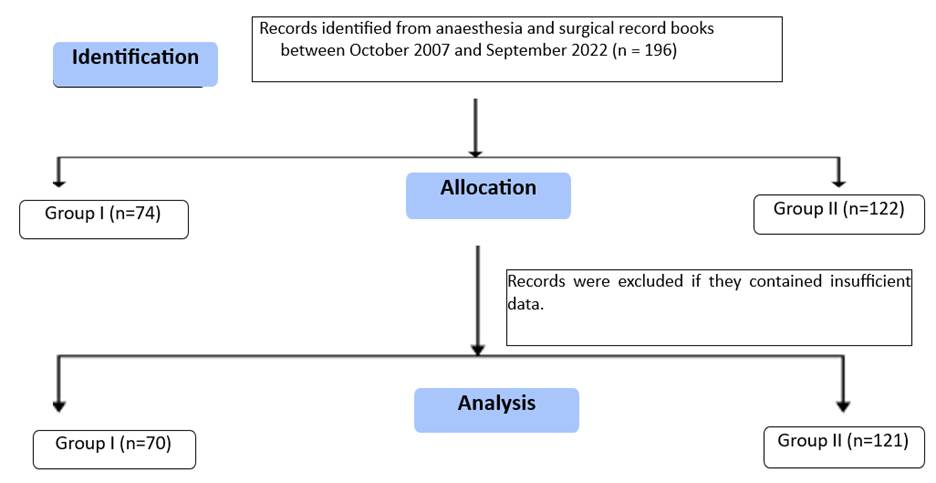
A total of 196 patient records were evaluated, of which 191 patients with complete data were included in the final analysis as shown in [Fig. 1].
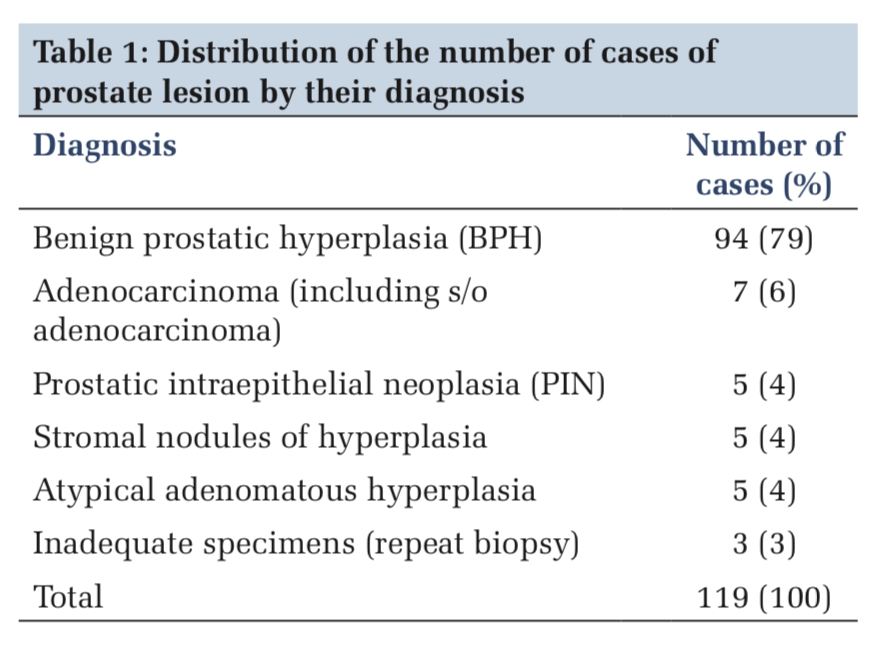
A total of 137 paediatric patients were included (Group I: n=52; Group II: n=85) as shown in [Table. 1]. There were no statistically significant differences between the two groups with respect to basic anthropometric variables. The mean age was comparable in Group I: 5.63 ± 1.06 vs Group II: 5.73 ± 1.73 years; p=0.352. Similarly, mean weight (16.42 ± 0.69 vs 15.63 ± 2.74 kg; p=0.567) and BMI (15.80 ± 0.72 vs 15.30 ± 0.56 kg/m²; p=0.742) did not differ significantly between groups. Sex distribution also showed no significant difference (p=0.138). Although male predominance was observed in Group II (55.29%)
compared to Group I (36.54%), the variation did not reach statistical significance. Overall, demographic parameters in the paediatric population were well balanced between both groups.
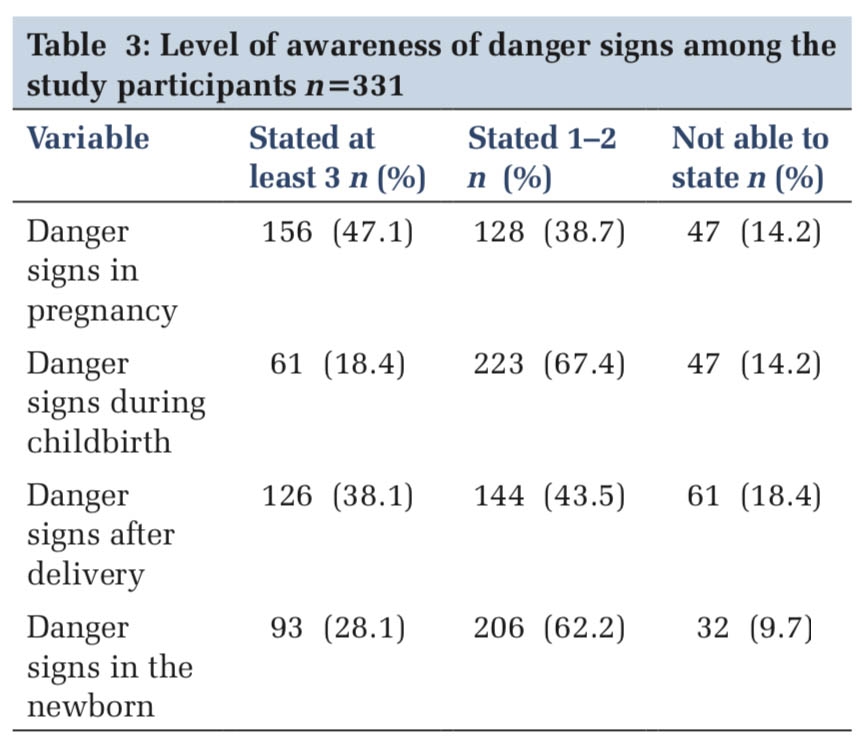
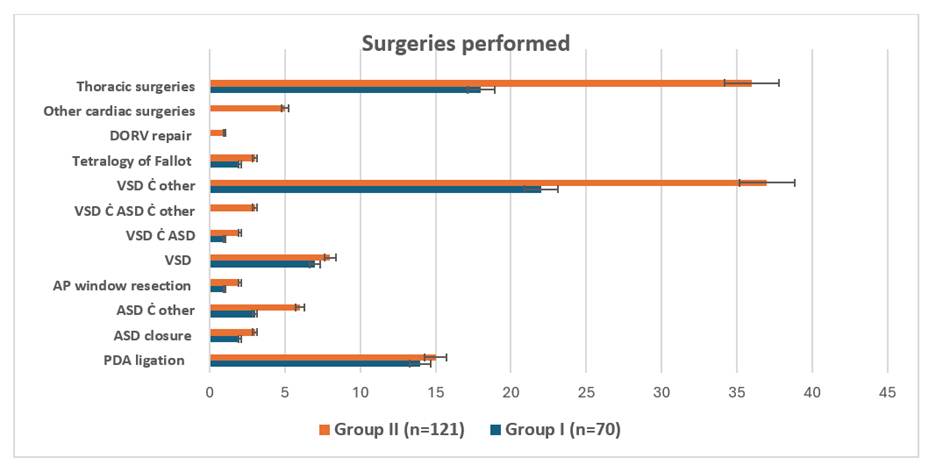
In [Table. 3], A total of 191 patients were categorized according to their preliminary diagnosis (Group I: n=70; Group II: n=121). The most frequently encountered condition in the overall cohort was VSD with associated lesions (VSD ± other/ASD), representing 30.89% of all cases, followed by thoracic injury (28.27%) and isolated PDA (15.18%). Within the subgroups, the proportional distribution of diagnoses was broadly comparable. VSD with associated anomalies remained the dominant diagnosis in both groups (Group I: 22 cases vs Group II: 37 cases). Thoracic injury was also highly represented in both groups (18 vs 36 cases respectively).
| Parameter |
Study (n=137) Mean ± SD |
Group I (n=52)
|
Group II (n=85)
|
p-value
|
|---|---|---|---|---|
|
Mean ± SD |
||||
| Average patient age (years) | 5.68±1.40 | 5.63±1.06 | 5.73±1.73 | 0.352 |
| Average patient weight (kg) | 16.03±1.72 | 16.42±0.69 | 15.63±2.74 | 0.567 |
| BMI kg/m2 | 15.56±0.64 | 15.80±0.72 | 15.30±0.56 | 0.742 |
| Sex, ratio (%) | ||||
| Male | 1 (48.18 %) | 1 (36.54%) | 1(55.29%) | 0.138 |
| Female | 1.08 (51.82 %) | 1.74(63.46%) | 0. 81(44.71%) | |
Data presented as means ± SD, BMI: Body Mass Index, SD: Standard deviation, a P<0.05, was considered statistically significant.
| Parameter | Study (n=54) | Group I (n=18) | Group II (n=36) | p-value |
|---|---|---|---|---|
|
Mean ± SD |
||||
| Average patient age (years) | 31.15±13.07 | 31.58±11.17 | 30.72±14.97 | 0.174 |
| Average patient weight (kg) | 65.28±19.34 | 64.73±18.94 | 65.83±19.73 | 0.284 |
| Sex, ratio (%) | ||||
| Male | 1 (83.38%) | 1 (84.62%) | 1 (82.14%) | 0.289 |
| Female | 0.19 (16.62%) | 0.18 (15.38%) | 0.21 (17.86) | |
Data presented as means ± SD, Kg: Kilograms, SD: Standard deviation, a P<0.05, was considered statistically significant.
| Diagnosis | Study (n=191) n, (%) | Group I (n=70) | Group II (n=121) |
|---|---|---|---|
| PDA | 29 (15.18%) | 14 | 15 |
| ASD | 5(2.62%) | 2 | 3 |
| ASD Ċ other | 9(4.71%) | 3 | 6 |
| AP window resection | 3(1.57%) | 1 | 2 |
| VSD | 15(7.85%) | 7 | 8 |
| VSD Ċ ASD | 3(1.57%) | 1 | 2 |
| VSD Ċ ASD Ċ other | 3(1.57%) | - | 3 |
| VSD Ċ other | 59(30.89%) | 22 | 37 |
| Tetralogy of Fallot | 5(2.62%) | 2 | 3 |
| DORV | 1(0.52%) | - | 1 |
| Other cardiac issues | 5(2.62%) | - | 5 |
| Thoracic Injury | 54 (28.27%) | 18 | 36 |
Ċ: With, ASD: Atrial septal defect, DORV: Double outlet right ventricle, PDA: Patent ductus arteriosus, VSD: Ventricular septal defect.
Less frequent congenital lesions included isolated ASD (2.62%), ASD with associated anomalies (4.71%), AP window resection (1.57%), DORV (0.52%) and combined VSD-ASD (1.57%). Minor variations in the frequency of individual cardiac lesions were noted across the groups; however, no large disproportion favouring one group was evident.
Overall, the diagnostic spectrum suggests a heterogeneous mix of congenital cardiac defects and thoracic trauma presentations, with VSD-related pathologies and thoracic injury accounting for the majority of surgical indications in both groups as shown in [Fig. 2].
To evaluate the complexity of cardiothoracic procedures in both study groups, preoperative status was assessed using the Ross/NYHA functional classification and Aristotle Comprehensive Complexity (ACC) score [Table. 4]. The overall mean ACC score for the cohort was 6.95 ± 0.32, with Group I demonstrating a mean of 6.8 ± 0.36 and Group II showing a mean of 7.1 ± 0.28. All procedures fell within ACC Level 2 complexity (range 6.0–7.9). The observed difference in ACC scores did not
reach statistical significance at the 0.05 threshold (|Z| < 1.96), indicating that surgical complexity was broadly comparable between the two groups.
Similarly, although minor variations were noted in the distribution of NYHA/Ross functional classes, these differences were also non-significant. Hence, both groups exhibited similar preoperative functional capacity, supporting the interpretation that baseline disease severity was equivalent across the two cohorts.
| Classifications | Group I (n=70) | Group II (n=121) | Z- value |
|---|---|---|---|
| ACC Score: (mean ± SD) | 6.8±0.36 | 7.1±0.28 | -1.48 |
| NYHA/ross preoperative functional class (n) %: |
|||
| I | (41) 58.57% | (73) 60.33% | -0.25 |
| II | (26) 37.14% | (37) 30.58% | +0.64 |
| III | (3) 4.28% | (11) 9.09% | -0.75 |
Data presented as means ± SD, CL‑95%, Z critical value ±1.96, ACC: Aristotle Comprehensive Complexity, NYHA: New York Heart Association, SD: Standard deviation, *P<0.05, was considered statistically significant.
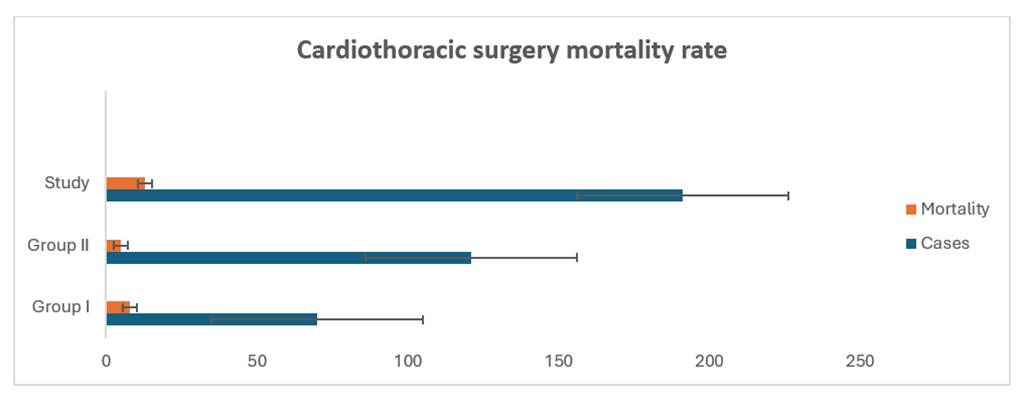
An overall mortality rate of 6.8% was observed among cardiothoracic surgeries in last 15 years. Mortality occurred in both groups, with Group I demonstrating an 11.4% mortality rate and Group II a 4.13% rate (p = 0.032). Mortality within the first 7 postoperative days showed a statistically significant reduction in group II as shown in [Fig. 3].
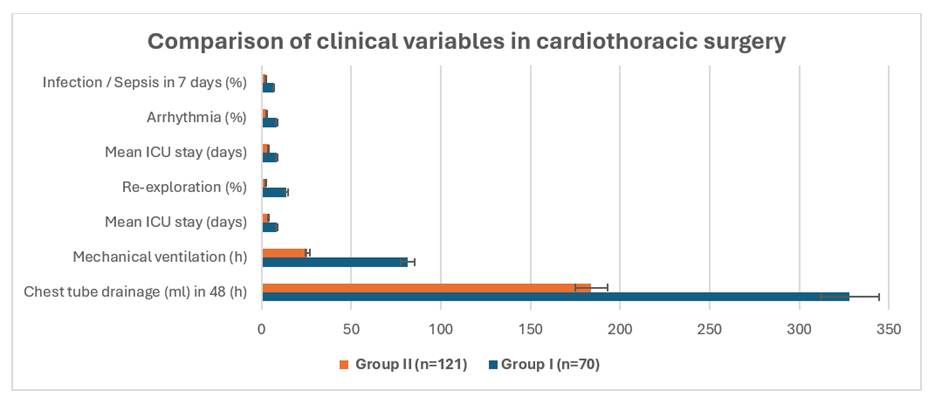
[Table. 5] summarises the comparison of key clinical outcomes between Group I and Group II. The rate of ultra-fast track (UFT) extubation was significantly higher in Group II than in Group I (37.31% vs. 7.84%; p = 0.015) in paediatric cardiac surgery cases. The mean duration of postoperative mechanical ventilation was significantly shorter in Group II (22.73 ± 6.49 hours) compared to Group I (82.34 ± 11.70 hours; p = 0.028). Chest tube drainage in the first 48 postoperative hours was also lower in Group II (97 ± 15.83 mL) than in Group I (133 ± 28.46 mL; p = 0.036) in paediatric cardiac surgery cases. Similarly, the mean length of hospitalisation was significantly reduced in Group II (4.18 ± 3.52 days) compared to Group I (6.87 ± 3.51 days; p = 0.047). Hypoglycemia was observed only in Group I (1.99%).
No statistically significant differences were observed in intensive care unit (ICU) stay duration (p = 0.279) or the incidence of arrhythmia (p = 0.072). Re-exploration was significantly more frequent in Group I, as determined by Fisher’s exact test (χ² = 0.0428, p = 0.018). In contrast, the incidence of infections/ Sepsis did not differ significantly between groups (χ² = 0.577, p = 0.279) in paediatric cardiac surgery cases. When comparing cardiothoracic cases, statistically significant differences were observed only in the mean duration of mechanical ventilation and in chest tube drainage volume (mL) during the first 48 hours postoperatively, as shown in [Fig. 4].
| Clinical variables | Group A (n=51) | Group B (n=83) | p-value |
|---|---|---|---|
| UFT extubations (%) | 7.84 | 37.31 | 0.015* |
| Mean duration of mechanical ventilator in postoperative period (h) | 82.34±11.70 | 22.73±6.49 | 0.028* |
| Mean ICU stay (days) | 3.14±2.37 | 1.91±2.94 | 0.279 |
| Chest tube drainage (ml) in the first 48 h in the postoperative period | 133±28.46 | 97±15.83 | 0.036* |
| Mean LOH (days) | 6.87±3.51 | 4.18±3.52 | 0.047* |
| Re-exploration (%) | 11.77 | 1.21 | 0.018* |
| Arrhythmia (%) | 5.88 | 1.21 | 0.072 |
| Infection/ Sepsis (%) | 3.92 | 1.21 | 0.238 |
Data presented as means ± SD, and percentage, ICU: Intensive care unit, LOH: Length of hospitalization, SD: Standard deviation, UFT: Ultra-fast track, *P<0.05 significant, Data presented as means ± SD and percentages.
Discussion
This one-and-a-half-decade retrospective review of cardiothoracic surgery at a major West African teaching hospital provides an important insight into the evolution of perioperative care, anaesthetic practice, and institutional governance within a low- and middle-income country (LMIC). By contrasting two distinct periods before and after the 2014 introduction of a modified World Health Organization (WHO) perioperative safety checklist the study demonstrates that structured, evidence-based interventions can substantially improve outcomes, even in resource constrained environments.
In the earlier phase (Group I), mortality was notably high at 11.4%, prompting a comprehensive review of anaesthesia and surgical protocols in 2014. This institutional audit initiated a paradigm shift toward refined perioperative management, early identification of risk factors, and enhanced case selection. Simpler congenital and acquired cardiac lesions were prioritised initially to foster progressive skill acquisition and ensure safer programme maturation. Following these reforms, overall mortality fell to 6.8%, with a significant decline in early postoperative deaths (≤7 days) from 11.4% to 4.13% in Group II figures comparable to those from established high volume international centres, where early mortality typically ranges between 3% and 4% [5].
Importantly, this reduction in mortality occurred alongside an increase in case complexity. Overall, various types of surgeries were performed over the past 15 years, with ventricular septal defect (VSD) and associated lesions being the most common diagnosis (30.89%), followed by thoracic injury (28.27%) and isolated patent ductus arteriosus (PDA) (15.18%). Patients in the later cohort presented higher Aristotle Comprehensive Complexity (ACC) scores and more severe New York Heart Association (NYHA) or Ross classifications [6-8], signifying that improved outcomes reflected genuine advances in perioperative safety rather than a shift toward less complex operations. These results affirm that systematic quality improvement and adherence to standardised, evidence based pathways can yield measurable benefits within LMIC surgical systems [9]. Similar progress has been reported by Khan et al. from Pakistan, underscoring the replicability of such approaches in comparable contexts [10].
Several targeted interventions were instrumental in this improvement. Early program mortality associated with ventilator-related complications led to the adoption of ultra-fast-track (UFT) extubation [11] protocols in 2014. This modification eliminated ventilator-associated infections and reduced postoperative morbidity, consistent with findings from Wu et al [12]. The introduction of antifibrinolytic agent tranexamic acid (TXA) into routine intraoperative practice further reduced postoperative bleeding (chest drainage 133±28.46 vs. 97±15.83ml; P=0.036), and re-exploration rates (11.77% vs. 1.21%; P=0.018), an especially valuable outcome where blood resources are limited. These findings align with global evidence supporting TXA’s efficacy and cost-effectiveness in cardiac surgery [13].
Overall, the study highlights the transformative effect of continuous audit, feedback, and iterative refinement of clinical protocols. The progressive improvement observed parallels experiences from other LMIC cardiac centres, such as those reported by Aljanadi, where structured quality-improvement frameworks and multidisciplinary collaboration enhanced surgical safety [14].
The trajectory at Komfo Anokye Teaching Hospital demonstrates that even within constrained systems, outcomes approaching international standards are achievable when guided by data driven decision making, disciplined teamwork, and contextually adapted clinical pathways tailored to local realities. Sustained commitment to education, governance, and innovation remains essential for the continued advancement of cardiothoracic surgery across developing regions.
Limitations
This study is limited by its retrospective design, single-centre scope, and relatively small sample size compared with large international datasets. Nevertheless, the one-and-a-half-decade span provides a unique longitudinal perspective on evolving practices in a resource limited setting.
Conclusion
This one-and-a-half-decade cohort highlights progressive improvements in perioperative care, surgical safety, and patient outcomes within a low- and middle-income country context. The strategic adoption of ultra-fast-track extubation, routine use of the antifibrinolytic agent tranexamic acid, strict implementation of WHO infection control guidelines, and strong multidisciplinary teamwork have collectively contributed to improved survival and reduced morbidity. Sustained investment in specialized training, local capacity building, and regional collaborations remains essential to further strengthen cardiothoracic surgical programs across West Africa.
Disclosure
Funding: None.
Conflict of Interest: None.
Data availability statement: All the data are available within the manuscript. In addition, the datasets used and analyzed during the current study are available from the corresponding author based on reasonable request.