Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.25.355
Year: 2026, Volume: 12, Issue: 2, Pages: 206-209
Case Report
Padmini Chitradurga Vijayasarathy 1, H S Raghavendra 2, T R Supriya 3, S Shanmugapriya 4, B R Vani 5
1Assistant Professor, Department of Pathology, Bangalore Medical College and Research Institute, Bengaluru – 560002, Karnataka, India.
2Post graduate, Department of Pathology, ESIC MC and PGIMSR, Rajajinagar, Bengaluru – 560010, Karnataka, India.
3Assistant Professor, Department of Pathology, ESIC MC and PGIMSR, Rajajinagar, Bengaluru – 560010, Karnataka, India.
4Professor, Department of Pathology, ESIC MC and PGIMSR, Rajajinagar, Bengaluru – 560010, Karnataka, India. 5Professor and Head, Department of Pathology, ESIC MC and PGIMSR, Rajajinagar, Bengaluru – 560010, Karnataka, India.
Address for correspondence: Padmini Chitradurga Vijayasarathy, Assistant Professor, Department of Pathology, Bangalore Medical College and Research Institute, Bengaluru – 560002, Karnataka, India.
E-mail: [email protected]
Received Date:01 November 2025, Accepted Date:16 January 2026, Published Date:12 June 2026
Mollaret meningitis is a term used to describe recurrent episodes of aseptic meningitis with a lymphocyte predominant pleocytosis with characteristic mononuclear Mollaret cell identified in cerebrospinal fluid cytology. Most of these cases tend to be associated with reactivation of HSV - 2 virus infection while only a handful of them can be seen associated with HSV - 1. With the advent of recent technologies, both these viruses can be readily detected using polymerase chain reaction. Although some patients benefit with anti-herpes medications, it typically resolves on its own without any residual neurological effects. Here, we attempt to describe a recent case of Mollaret's meningitis associated with HSV-1 encephalitis we came across in our institute and review the literature where Mollaret cells were noted on CSF cytology in unique cases.
The term Mollaret meningitis was coined by Pierre Mollaret (1898-1987), a French neurologist and epidemiologist and has made significant contributions towards treatments of infectious diseases like malaria and poliomyelitis. He is well known in the field of medicine for describing the anatomical connections of the dentate nucleus, red nucleus and the contralateral inferior olivary nucleus related to palatal myoclonus known popularly as the “Guillain-Mollaret triangle”[1]. He has also reported a case series in French titled "recurrent benign endothelioleukocytic aseptic meningitis" in the year 1944, in which he has described three patients who had recurrent episodes of aseptic meningitis and presented with history of fever and meningism lasting for about 2 to 5 days, followed by spontaneous resolution of symptoms with no residual neurological deficits, later known widely as Mollaret meningitis[2]. He also described the cytology findings in
the cerebrospinal fluid within the first 24 hours as ‘fantomes cellulaires’ which came to be popularly known as the Mollaret cell. These cells are large mononuclear cells with blunt cytoplasm with projections having a bean-shaped, bilobed nuclei. Further, in the year 1982, reactivation of latent infection from herpes viruses was incriminated as the cause for Mollaret meningitis, due to multiple overlapping features between the two. Using electron microscopy de Chadarévian and Becker, proved that Mollaret’s cells were ‘epithelioid looking monocytes or macrophages’[1]. HSV-2 is the most often pathogen identified in this illness, owing to the growing use of molecular diagnostic tools. HSV-1, varicella zoster virus, Epstein-Barr virus, human herpesvirus-6, and enterovirus are other viruses that can seldom cause the illness[3].
A 46-year-old male patient, presented to the emergency department with complaints of headache, fever, slurred speech and difficulty in walking since 3 days. He was noted to have had fever, cough and generalised myalgia since 10 days prior to which he was in his usual state of health and performing his routine activities. The fever was insidious in onset, initially low grade and being associated with cough and myalgia was brushed off as a simple flu by the patient. As the symptoms did not tend to resolve he consulted a local ayurvedic doctor, who had treated the disease symptomatically using antipyretics.
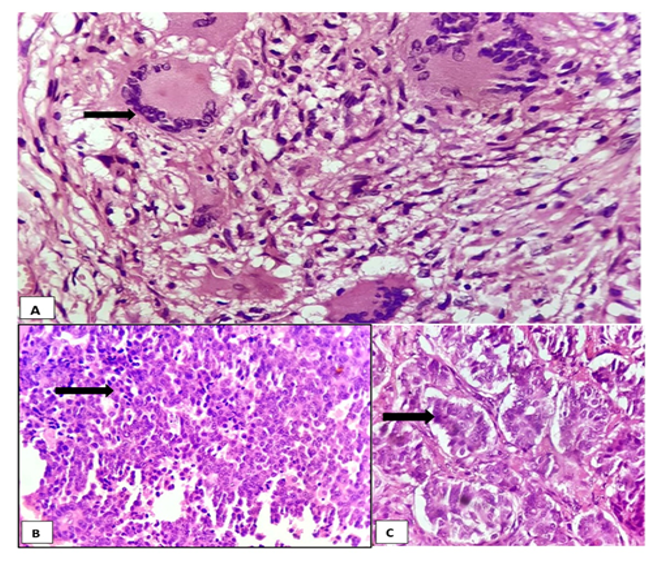
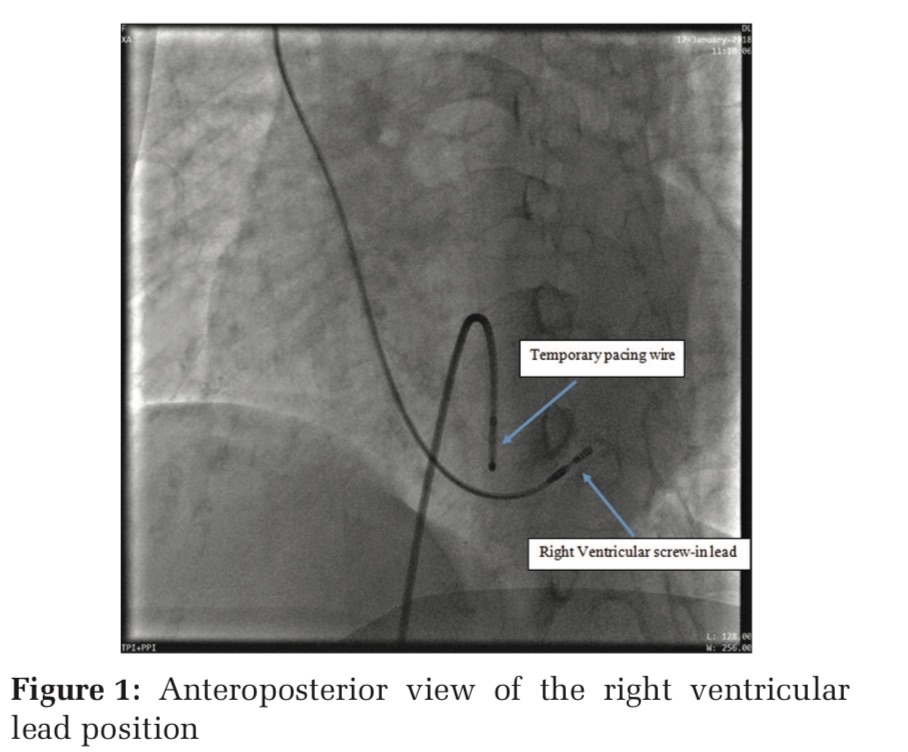
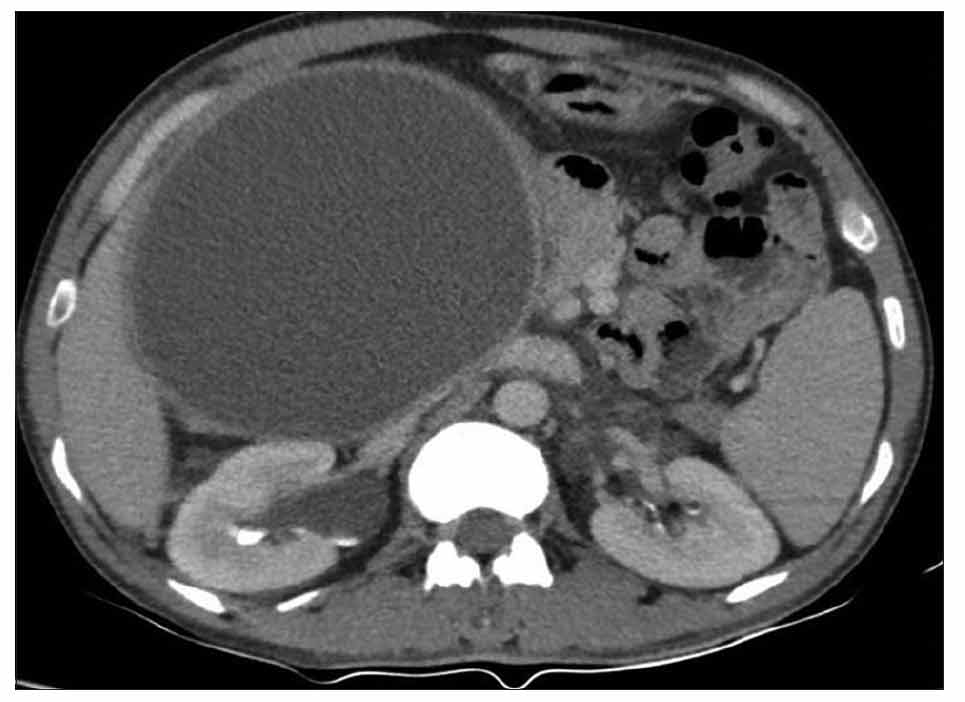
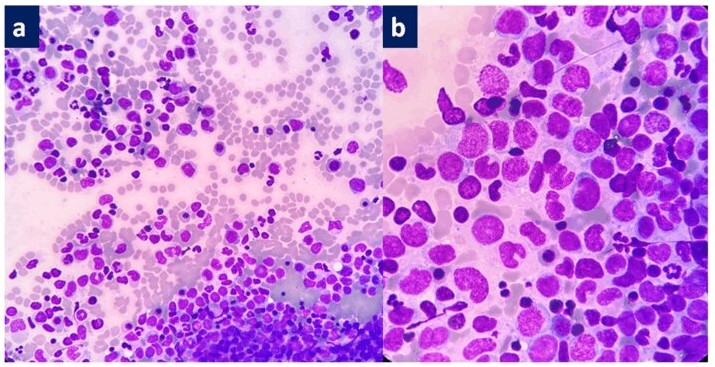
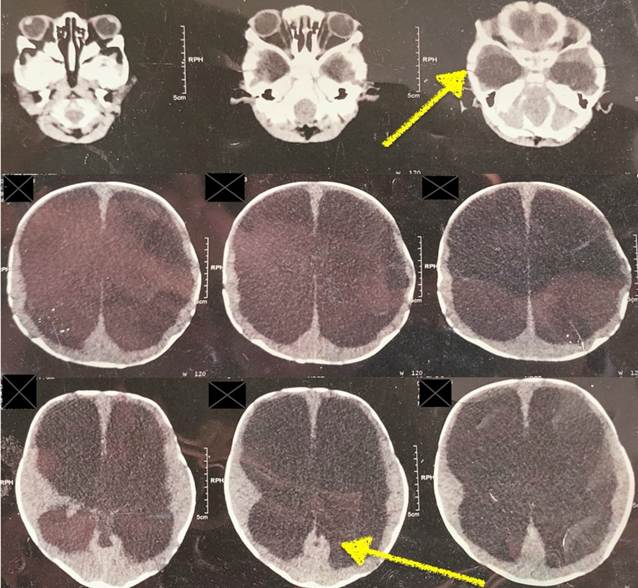
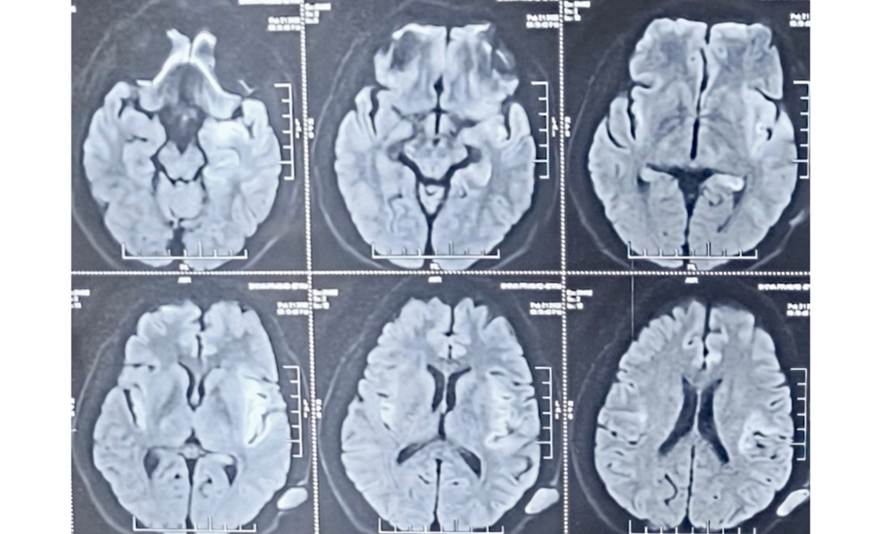
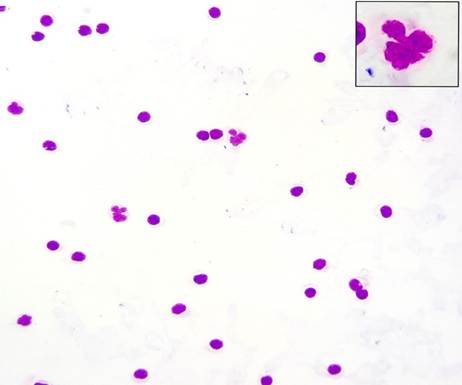
The general condition of the patient further deteriorated in the next few days presenting with altered sensorium, inability to walk and speak, which was when the patient sought medical attention at a higher centre for evaluation. The patient was a known case of ischaemic heart disease, with post coronary angiogram and on regular medication. At presentation, the pulse rate was 119; blood pressure of 130/90 mmHg, respiratory rate of 22 cpm with room air saturation of 98% and the Glasgow coma scale (GCS) score at presentation was E2V1M4 with bilateral constricted pupils of 3mm diameter. The patient was intubated and placed on mechanical ventilatory support. Computed tomography of the brain showed features of an acute ischaemic infarct [Fig. 1]. The Magnetic Resonance Imaging of the brain showed bilateral hyperintensities in T2 flair and DWI in insular cortices, left temporal region, left hippocampus and left pericallosal region which was asymmetrical and more in the left temporal region than the right. Lumbar puncture was done at the level of L4-L5 and the cerebrospinal fluid cytology (CSF) sent to biochemical, pathological and microbiological examination. The CSF examination showed a lymphocyte predominant pleocytosis with 220 cells with 94% lymphocytes, 5% were large monocytes having irregular, multilobated nucleus with abundant pale grey cytoplasm typical of a Mollaret cell [Fig. 2] and 01% neutrophil. CSF glucose (56.00 mg/dL), chloride (119.00 mEq/L) and Adenosine deaminase (1.65 U/L) were within normal limits, while protein was elevated (89.50 mg/dL). The microbiological culture report was non diagnostic. The CSF was subjected to meningoencephalitis panel by polymerase chain reaction, which was able to detect the presence of HSV-1 virus DNA. The patient was treated with intrathecal injection Acyclovir. However, despite the treatment, patient had persistent fever spikes with thick whitish endotracheal tube secretions. Bronchoalveolar lavage culture was sent which showed no growth. Liver function tests and kidney function tests remained unremarkable throughout the stay. The patient had an isolated involuntary movement of bilateral upper limbs of tonic type which was controlled with intravenous Levetiracetam 1 gm twice daily, following which there was no recurrence. The GCS score persistently remained at E1M5 with paucity in right upper limb and lower limb. Repeat lumbar puncture with CSF analysis was done after a week. The CSF cytology showed a decrease in cell count of 150 cells with predominant lymphocytes (95%), Mollaret cells (3%) and occasional neutrophils (2%). CSF glucose (50.00 mg/dL), chloride (121.00 mEq/L) while protein remained elevated (75.00 mg/dL). The clinical status of the patient remained same without any improvement and persistent GCS score of E1M5 over the next one week. A repeat CSF analysis was done on day 14 of admission showed decreases in cell count to 40 cells with similar morphology of cells comprising of lymphocytes (98%), Mollaret cells (1%) and occasional neutrophil (1%). CSF glucose (48.00 mg/dL), chloride (116.00 mEq/L) and protein still remained elevated (68.00 mg/dL). The patient however, succumbed with development of ventilator associated pneumonia and endotracheal tube culture showing growth of multiple drug resistant Klebsiella pneumoniae. We present this case as our patient here had a single episode of HSV-1 associated encephalitis that showed the persistent finding of lymphocytic pleocytosis along with the presence of Mollaret cells in CSF cytology even after a duration of 3 weeks from the onset of symptoms.
Pierre Mollaret described the Mollaret cell and Mollaret meningitis in 1944[1]. Although the symptoms in Mollaret meningitis are abrupt in onset, most of the times these cases have been noted to be self-limiting. There have been isolated reports of symptoms at presentation included memory loss, paresthesia, vertigo, and difficulty in concentrating. Although it is thought to be mild and self-limiting, there have been occasions where unexpected severe neurological outcomes have been observed[2]. Herpes Simplex Virus (HSV) has frequently been considered a potential cause of Mollaret meningitis[4]. It is now known to be often associated with latent infection from HSV-2[3]. Both HSV-1 and HSV-2 are capable of remaining dormant within sensory ganglia. Various triggers such as secondary infections, physical trauma, shock, exposure to chemicals or sunlight, immunosuppression, and surgical procedures can reactivate this virus[4]. HSV-2 is commonly implicated in genital infections can also typically cause viral meningitis in immunocompetent individuals. Whereas HSV-1, particularly known for causing recurrent oral and peri-oral infections, gingivostomatitis, is more frequently connected with sporadic cases encephalitis in adults and children[3, 4]. Chan TY et al.[5] analysed CSF from 14 patients with Mollaret’s meningitis which had a consistent finding of Mollaret cells along with plasma cells or polymorphs. HSV-2 was confirmed in only two of the patients. Majority of cases in their study did not have a confirmed infectious cause, highlighting the recurrent and idiopathic nature of the condition in many patients. Rarely, there has been evidence of a link between HSV-1 and Mollaret meningitis. Steel et al.[4] were the first to report, finding HSV-1 in the CSF of a patient who had four episodes of aseptic meningitis[5].
It is also of great interest to note that isolated case reports have been reported where the findings of Mollaret meningitis was noted in few uncommon cases[4]. Graman S et al.[6] reported a case, in a 19-year-old male patient who had recurrent episodes of aseptic meningitis during an episode of acute infectious Epstein Barr Virus (EBV) infectious mononucleosis. EBV specific antibodies were detected in the serum. The patient had seven episodes of aseptic meningitis ranging over a period of one year. In all of the seven episodes, CSF cytology showed polymorphonuclear pleocytosis[6]. Kumar P et al.[7] reported a case of 8-year-old girl with three episodes of aseptic meningitis with history of frequent headaches over a period of one year. CSF cytology showed the presence of Mollaret cells. PCR for enterovirus RNA in CSF was positive. It is supposedly the first case reported in literature where Mollaret cells were seen in association with enterovirus[7]. Capouya JD et al.[8] reported a case of 16 yr old female patient who was a case of Acute lymphoblastic leukaemia in remission. She developed three episodes of aseptic meningitis over a span of 3 months. HHV 6 isolated from CSF using PCR assay. CSF cytology showed the presence of few monocytes. She was successfully treated with Foscarnet[8]. Procop GW et al.[9], studied 22 cases of patients with West Nile Infection, in Ohio, United States. Of them, 3 patients were noted to have high cellularity in CSF. CSF cytology showed the presence of Mollaret cells. One of the patients had a fatal course, whose postmortem neurological examination showed extensive perivascular lymphocytic infiltrate admixed with mononuclear cells that were consistent with Mollaret-like cells[9]. T. Ohmichi et al. [10] reported a 15-year-old female with a history of herpes zoster presented with headache, fever, and meningism. CSF analysis showed mononuclear pleocytosis and elevated protein. PCR confirmed varicella-zoster virus (VZV) meningitis and CSF cytology revealed characteristic Mollaret cells. She was treated with intravenous acyclovir, leading to rapid clinical improvement and reduced CSF cell counts. Gao et al.[11] reported an unusual case of an 8-year-old girl who suffered 38 episodes of recurrent aseptic meningitis over 27 months. CSF cytology consistently showed mononuclear pleocytosis and the presence Mollaret cells. MRI revealed an intraspinal epidermoid cyst at the T12-L1 level. The cyst was surgically excised, and histopathological analysis confirmed the diagnosis of an epidermoid cyst. The authors suggested that rupture or leakage of cyst contents into the subarachnoid space may have triggered repeated episodes of chemical meningitis and immune activation, resulting in the appearance of Mollaret cells [Table. 1].
|
Study |
Year |
Etiological agent |
|---|---|---|
|
Steel JG et al.[4] |
1982 |
Herpes Simplex Virus -1 |
|
Graman S et al.[6] |
1987 |
Epstein Barr Virus |
|
Chan TY et al.[5] |
2002 |
Herpes Simplex Virus -2 |
|
Procop GW et al.[9] |
2004 |
West Nile Virus |
|
Capouya JD et al.[8] |
2006 |
Human Herpes Virus - 6 |
|
Gao B et al.[11] |
2007 |
Intraspinal Epidermal Cyst |
|
Ohmichi T[10] |
2012 |
Varicella Zoster Virus |
|
Kumar P et al.[7] |
2016 |
Enterovirus |
|
Present study |
2025 |
Herpes Simplex Virus - 1 |
Mollaret meningitis being a generally benign, transient, self-limiting condition, may also have an uncommon potential to manifest in more severe, unanticipated, and potentially fatal forms. Mollaret cell, though frequently seen in cases of Mollaret meningitis, is not specific. The characteristic morphology often aids in swift identification and their occurrence outside the classic self-limiting aseptic meningitis presentation warrants careful consideration. This case highlights that Mollaret cells may represent a broader cellular response to sterile meningeal irritation, potentially triggered by diverse inflammatory or immune-mediated processes.
Declaration of consent: necessary informed written consent was obtained from the patient attenders.
Conflict of interest: Nil.
Financial declaration: Nil.
1. Mollaret’s Meningitis. European Neurology. 2008; 60 (6). Available from: https://doi.org/10.1159/000159930
2. Mollaret's Meningitis: CSF Cytology to the Rescue. Neurology India. 2020; 68 (5). Available from: https://doi.org/10.4103/0028-3886.299162
3. Mollaret’s Meningitis due to Herpes Simplex Virus 2: A Case Report and Review of the Literature. Microorganisms. 2024; 12 (7). Available from: https://doi.org/10.3390/microorganisms12071363
4. Isolation of herpes simplex virus type 1 in recurrent (Mollaret) meningitis. Annals of Neurology. 1982; 11 (1). Available from: https://doi.org/10.1002/ana.410110104
5. Mollaret's meningitis: Cytopathologic analysis of fourteen cases. Diagnostic Cytopathology. 2003; 28 (5). Available from: https://doi.org/10.1002/dc.10261
6. Mollaret's Meningitis Associated With Acute Epstein-Barr Virus Mononucleosis. Archives of Neurology. 1987; 44 (11). Available from: https://doi.org/10.1001/archneur.1987.00520230084023
7. Mollaret's meningitis and enterovirus infection. Current Medicine Research and Practice. 2016; 6 (2). Available from: https://doi.org/10.1016/j.cmrp.2016.03.005
8. Mollaret’s Meningitis Due to Human Herpesvirus 6 in an Adolescent. Clinical Pediatrics. 2006; 45 (9). Available from: https://doi.org/10.1177/0009922806295286
9. Mollaret-like Cells in Patients with West Nile Virus Infection. Emerging Infectious Diseases. 2004; 10 (4). Available from: https://doi.org/10.3201/eid1004.030783
10. Mollaret cells detected in a patient with varicella-zoster virus meningitis. Clinical Neurology and Neurosurgery. 2012; 114 (7). Available from: https://doi.org/10.1016/j.clineuro.2012.02.015
11. Mollaret Meningitis Associated With an Intraspinal Epidermoid Cyst. Pediatrics. 2007; 120 (1). Available from: https://doi.org/10.1542/peds.2006-2053
Subscribe now for latest articles and news.