Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.018
Year: 2021, Volume: 7, Issue: 2, Pages: 109-111
Case Report
H P Sapna1, T N Harsha2, Gaana Sreenivas3
1 Assistant Professor, Department of Obstetrics and Gynaecology, JSS Medical College, JSS Academy of Higher Education and Research, Mysore, Karnataka, India
2 Senior Specialist and Consultant, Department of Obstetrics and Gynaecology, Kodagu Institute of Medical Sciences, Madikeri, Karnataka, India
3 Registrar, Department of Obstetrics and Gynaecology, Cloudnine Hospital, Bangalore, Karnataka, India
Address for correspondence:
Dr. T N Harsha, Department of Obstetrics and Gynaecology, Kodagu Institute of Medical Sciences, Madikeri, Karnataka, India. Phone: +91-9663655882. E-mail: [email protected]
Fetal growth restriction (FGR) is one among the major factor for perinatal mortality and morbidity. Risk factors for FGR being multifactorial, one among them is a subchorionic placental cyst.Hence presenting a rare of case of 30 years old lady with features of PPROM with previous LSCS along with features of FGR.
Keywords: Intrauterine growth restriction, placental cyst, placental insufficiency.
Fetal growth restriction (FGR) is said to be present in those babies whose birthweight is below the 10th percentile of the average for gestational age.[1] Delayed growth puts the baby at risk of certain health problems during pregnancy, delivery, and after birth. FGR is a condition of varied and extensive etiology.
The risk factors for FGR can be maternal or fetal or placental or unknown in origin. Maternal causes are anemia, hypertension, smoking, alcohol abuse, drug addiction, poor maternal nutrition, and heart and kidney diseases. Fetal causes are TORCH infections, chromosomal abnormalities (Trisomy 13 or 18 or 21 and Turners syndrome), structural anomalies, and multiple pregnancies. Placental causes include cases of poor uterine blood flow to the placental site for a long time. Placental pathologies include placenta previa, abruption, circumvallate, infarction, mosaicism, and placental cyst.[2]
True placental cysts are rare with a prevalence of 2–7%.[2] Most placental surface cysts are associated with a normal pregnancy outcome. Most such cysts are related to cystic change in an area of sub associated with intrauterine growth restriction (IUGR).[2] chorionic fibrin. Cysts larger than 4.5 cm or more than 3 in number are more frequently. This is a rare case of such a placental cyst causing FGR.
A 30-year-old female with 32 weeks and 4 days of gestation, G4 P1 L1 A2 with cephalic presentation was admitted with history of previous lower segment Cesarean section (LSCS) and Pre-labor Rupture of Membranes (PPROM) with late-onset FGR. Patient was referred from the peripheral center to JSS Hospital, Mysore for further safe confinement.
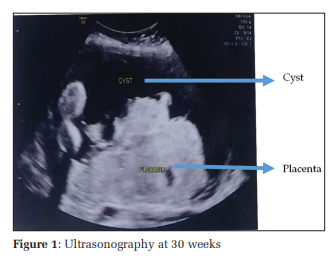
The vitals of the patient and all biochemical investigations were within normal limits. However, Ultrasonography showed a large placental cyst at the surface of the placenta. The cyst was found to measure 8 cm × 5 cm in 22-week scan with normal growth and progressed to measure 10.3 cm × 6.4 cm at scan done on 30 weeks with features of IUGR and normal Doppler as shown in Figure 1. However, 32 weeks scan showed IUGR with abnormal Doppler findings.
She was taken up for emergency LSCS in view of PPROM with FGR and a female baby weighing 900 g was delivered. Liquor was clear and scanty. Uterus and bilateral tubes were healthy. Placenta was fundal and anterior. Placenta weighed 700 g at birth and was unhealthy with a cyst of 10 cm × 8 cm containing brownish-colored liquid with base containing smudge-like material. Baby had a weak APGAR score at birth. Baby was shifted to the neonatal intensive care unit (NICU) as it was a preterm delivery and had FGR. The baby was in NICU for a month and discharged in good health.
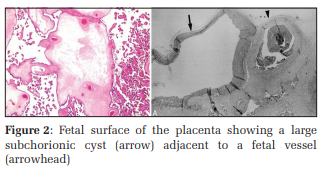
Macroscopically, histopathology showed an unremarkable ruptured cyst on the outer surface of the placenta of 8.5 cm × 7 cm. Microscopically, Multiple sections studied from placental tissue showed maternal floor infarction, extensive perivillous fibrin deposition, large hemorrhage, and focal thrombosis of fetal arteries. Sections of the cyst wall show amnion, chorion, and fibrin infiltrated by intermediate trophoblasts. These features are consistent with a subchorionic cyst as shown in Figure 2.
Fetal growth is a complex, multifactorial phenomenon that is influenced predominantly by maternal health, uterine environment the quality of placental and fetal perfusion. A variety of cysts maybe found in the placenta. Cytotrophoblastic cysts maybe located within the placental tissue (Septal cysts) or under the fetal plate (Subchorionic cysts). The frequency of these placental cysts has been reported to be 5% to 7% for subchorionic cysts and up to 20% for septal cysts.[3] On macroscopic examination, they are usually singular but can be multiple. They maybe central and lie immediately below the chorionic plate. They usually measure <2 cm in diameter and tend to occur more frequently in cases of diabetes mellitus or maternal-fetal incompatibility. Microscopically, the wall of the cyst consists of amniotic and chorionic membranes. The cells that cover the cyst are called X-cells. These cells produce pregnancy-associated major basic protein and are highly toxic and causes tissue degeneration and cyst formation. Sonographically, subchorionic cysts are found as echo-free cavities under the fetal plate and should be differentiated from both chorio angiomas and subchorionic fibrin deposition.[1,3]
Sub chorionic cyst maybe seen as early as the first trimester with transvaginal ultrasound. They usually remain unchanged on serial scans. However, in a few cases, they may increase in size as the pregnancy progresses. Sub chorionic placental cysts are frequent and innocuous. Although they usually have no clinical significance, a large subchorionic cyst attached near the umbilical cord incision maybe a threat to fetal wellbeing if there is a constriction and reduction of umbilical cord blood flow. In prior studies, in all cases of FGR, the cyst was larger than 4.5 cm in diameter at some point in the pregnancy.[4] In our case, a large surface subchorionic placental cyst measuring 10 cm × 8 cm caused FGR.
FGR, a condition with varied and broad aetiology is regularly encountered in day-to-day practice. Sub chorionic placental cysts are ominous findings when attached near the umbilical cord insertion, but in our case, FGR was found even when the placental cyst was not attached in the umbilical cord insertion site. Thus, when identified, a large subchorionic cyst should be followed closely by ultrasound, color Doppler and assessment of fetal wellbeing to rule out FGR.
Hence, this case shows that when a placental cyst of any size, irrespective of its site has to also be taken into account for FGR and is not to be neglected as an inconspicuous finding. This shows that placental cyst should be excluded sonographically when FGR has been considered. Further studies need to be done to evaluate the association found in this study between peripheral subchorionic placental cyst and FGR
Subscribe now for latest articles and news.