Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i1.25.279
Year: 2026, Volume: 12, Issue: 1, Pages: 104-108
Case Series
Anirban Mallick 1, Jahnavi Dande 2, Anand Bhandari 3, Jeewan Kumar 4
1Sports Physician, Dept of Sports Medicine, Sports Authority of India, Sonipat, Haryana, India.
2Sports Physician, Dept of Sports Medicine, National Institute of Sports, Patiala, Punjab, India.
3PG resident, Dept of Sports Medicine, National Institute of Sports, Patiala, Punjab, India.
4Senior Interventional Cardiologist, Amar Hospital, Patiala, Punjab, India.
Address for correspondence: Anirban Mallick, Sports Physician, Dept of Sports Medicine, Sports Authority of India, Sonipat, Haryana, India.
E-mail: [email protected]
Received Date:16 August 2025, Accepted Date:25 November 2025, Published Date:06 May 2026
Determining eligibility for competition for an athlete who reports no symptom and family history of sudden cardiac death presents a unique dilemma - specifically when the electrocardiogram (ECG) reveals atypical repolarization finding. T wave inversion (TWI) seen in two or more neighbouring anterior or lateral ECG leads poses a significant concern as such finding commonly is associated with hypertrophic cardiomyopathy (HCM) and arrhythmogenic right ventricular cardiomyopathy. In first three cases, comprehensive diagnostic testing failed to identify structural or functional cardiac pathology, leading to medical clearance for competition. In contrast, fourth athlete demonstrated echocardiography finding characteristic of HCM. Current research does not conclusively support that isolated TWI in asymptomatic athletes as a definitive marker of cardiomyopathy. But the broad spectrum of clinical outcomes among athletes with TWI poses a challenge for treating sports medicine specialist. This case series aims to focus on the grey area dealing with athletes having TWI in ECG and their return to play decision by the clinician.
Adaptation of heart due to sustained athletic training often produces noticeable changes on a standard 12 lead electrocardiogram (ECG) often named athlete’s heart[1]. Common benign findings in trained individuals include bradycardia, voltage patterns resembling left ventricular hypertrophy (LVH), conduction delays such as first degree AV block and incomplete right bundle branch block. T wave inversion (TWI) poses a diagnostic challenge specifically since these changes are seen in inherited heart conditions associated with sudden cardiac death (SCD). This leads to a complex challenge faced by physicians tasked with assessing athletes’ eligibility specially when athletes show repolarization anomalies but present no clinical symptoms and normal follow up tests[2].
Juvenile ECG pattern
TWI is often a normal finding in young individuals, especially when limited to anterior chest leads. This is referred to as “juvenile” ECG pattern, which includes inverted or biphasic T waves extending beyond lead V1 in those who are not yet physically matured[3].
During puberty, T waves usually become positive in leads V2 to V6, and remain inverted in V1[4]. Evidence suggests that hormonal and developmental changes during adolescence have greater impact on T wave configuration than athletic training alone[5]. As a result, anterior TWI extending to lead V3 in pre-pubertal individuals, in the absence of symptoms or a family history do not warrant any further investigations[6]. In such cases, routine follow up on an annual basis is often considered sufficient until repolarization pattern normalizes.
Repolarization patterns in athletes of Afro-Caribbean descent
TWI appeared more frequently in this group compared to others. Healthy athletes of this group showed TWI in anterior leads (V1-V4), while those diagnosed with hypertrophic cardiomyopathy (HCM) more often exhibited TWI in inferior or lateral leads. Anterior TWI
(V1-V4) in this group of athletes appeared alongside a specific repolarization pattern characterized by J point elevation and dome shaped ST segment rise[7]. These distinct ECG traits suggest that anterior TWI in presence of early repolarization may reflect physiological adaptation in this group of athletes. However, when T wave involves inferior or lateral leads, or accompanied by ST depression, further evaluation to rule out cardiomyopathy is recommended.
Influence of body position and chest structure on TWI
A shift from lying down to standing can lead to noticeable changes in ECG. Activation of sympathetic nervous system, altered venous return as well as diaphragm movement can alter axis and amplitude of ECG waves, including T waves[8].
Apparent T wave normalization during exercise
Pseudonormalization refers to a situation where T wave that is inverted at rest typically by 1 mm or more appears upright during physical exertion. Studies have shown that athletes with early arrhythmogenic cardiomyopathy (ACM) can also display similar T wave normalization during exercise, even when structural abnormalities are not yet prominent. Specifically, exercise related resolution of TWI in right precordial leads (V1 - V3) was seen in some ACM patients and these changes do not
reliably distinguish between those with disease and with normal athletic adaptation[9].
TWI related to athletic training
Some studies suggested that TWI in leads V1 - V3 occurred more often in endurance athletes[10] probably due to cardiac remodelling. Outward shift of right ventricle due to left ventricular enlargement in these groups of athletes may alter ECG readings without reflecting disease.
All elite athletes undergo a comprehensive medical evaluation and cardiac assessment at National Institute of sports, Patiala, India before being cleared to participate in the national training camps. This assessment includes thorough review of personal and family medical history, cardiovascular examination, and a standard resting 12 lead ECG. In this case series we present four cases of different clinical scenarios of athletes with TWI leading to complex decision making for eligibility to return to play. Patient characteristics are mentioned in [Table. 1]. Informed consent was obtained from the athletes/parent for the purpose of the publication.
Case 1
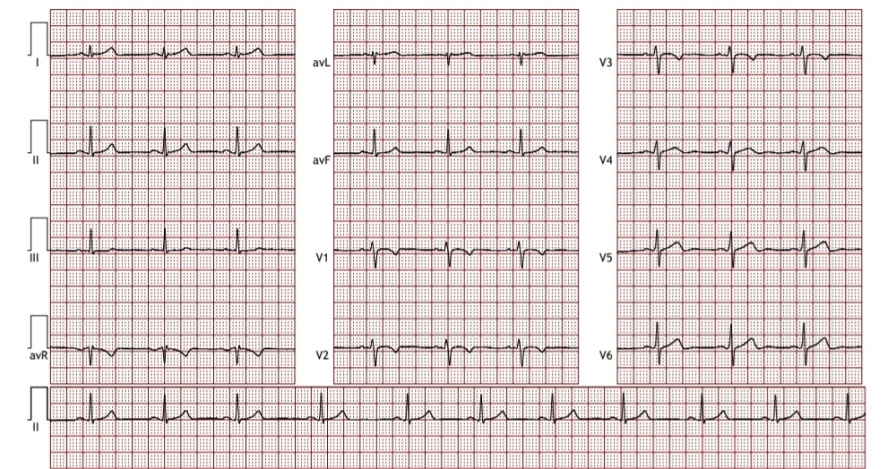
A 26 year old male marathon runner underwent routine pre participation cardiovascular screening. He had been engaged in intense training for past 08 years. He reported no cardiac complaints including chest pain, palpitation etc. and also no family history of SCD. His recorded BP was 110/76 mm Hg and heart rate was 62 bpm, however his resting 12 lead ECG showed TWI in V1 - V3, but no signs of LVH [Fig. 1].
Due to atypical ECG finding, echocardiogram was carried out which suggested left ventricular hypertrophy with normal wall thickness and systolic and diastolic function. This type of ECG changes in ultra endurance athletes suggest endurance training induced physiological adaptation characterized by lateral displacement of right ventricle and its apex toward axilla representing a spatial adjustment to thoracic constraints secondary to cardiac enlargement. Hence, he was cleared for unrestricted sports participation.
Case 2
A 15 years old male fencing athlete underwent evaluation as a part of routine pre- participation medical screening. He had training history of 4 years, without any cardiac symptom or positive family history. His blood pressure was 120/76 mm Hg and heart rate was 86 bpm. ECG demonstrated TWI from V1 to V3 with no other abnormality [Fig. 2]. Since this was his first comprehensive pre-participation evaluation, an echocardiography was advised which did not reveal any abnormality.
In adolescent athletes, anterior TWI extending to lead V3 is considered as normal age related finding and does not necessitate further diagnostic evaluation, hence he was advised to do annual follow up until normalization of anterior TWI with clearance of unrestricted sporting activity. Parents were also counselled accordingly.
Case 3
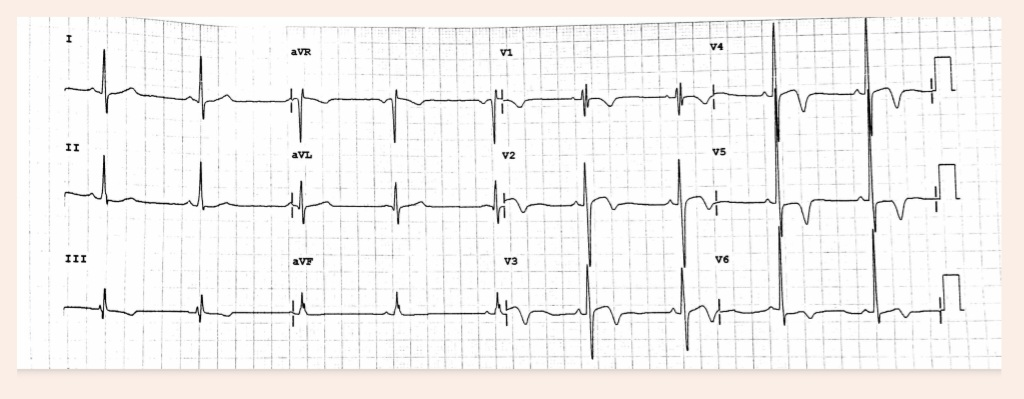
A 30 year old male elite international boxer underwent assessment during routine pre- participation cardiovascular screening. He had engaged in high intensity training for preceding seven years without any positive personal and family history of adverse cardiac event. His resting blood pressure was 126/82 mmHg and heart rate 68 bpm. Physical examination was otherwise unremarkable. A resting 12 lead ECG demonstrated TWI in lead III, aVR, and leads V1-V6 [Fig. 3].
|
Athletes |
Age |
Sex |
Sports |
BMI |
Training |
Clinical |
Family |
|---|---|---|---|---|---|---|---|
|
Athlete 1 |
26 years |
Male |
Athletics (Long |
19.85 |
08 years |
No cardiac |
Negative for |
|
Athlete 2 |
15 years |
Male |
Fencing |
19.25 |
04 years |
No cardiac |
Negative for |
|
Athlete 3 |
30 years |
Male |
Boxing |
23.28 |
07 years |
No cardiac |
Negative for |
|
Athlete 4 |
27 years |
Male |
Athletics |
29.13 |
08 years |
No cardiac |
Negative for |
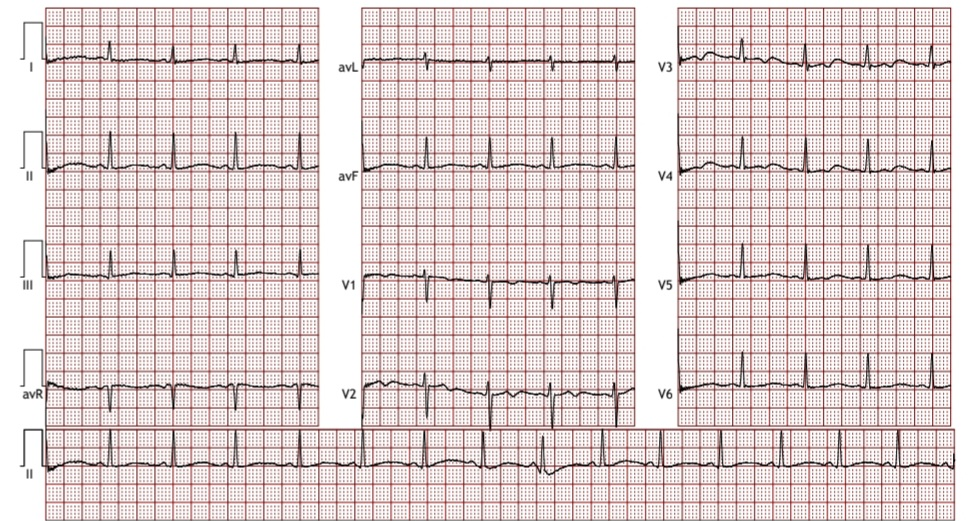
Given this abnormal ECG pattern, transthoracic echocardiography was performed, revealing concentric left ventricular hypertrophy with an end systolic posterior wall thickness of 1.8 cm and interventricular septal thickness of 1.6 cm with preserved cavity size (end systolic diameter 3.0 cm, end diastolic diameter 4.8 cm) and normal systolic function. Transesophageal echocardiography also yielded concordant findings.
Due to this combination of ECG abnormalities and suggestive echocardiographic features, cardiac magnetic resonance imaging (CMRI) was undertaken. CMRI demonstrated cardiomegaly with enlargement of right atrium (RA) and right ventricle (RV). Biventricular wall motion was preserved at rest, with no evidence of focal or diffuse myocardial bulging in RV. There were no abnormal fat signals in either ventricle, and delayed gadolinium enhancement imaging showed no subendocardial or myocardial fibrosis. No pericardial effusion was present and mediastinal vessels displayed normal morphology and anatomical relationship. Overall, the imaging finding did not fulfil diagnostic criteria for dilated cardiomyopathy, arrhythogenic right ventricular cardiomyopathy (ARVC) or HCM.
Hence the athlete was granted medical clearance but advised to undergo annual cardiovascular follow up including echocardiography along with one of the family members (more than 10 years). He was counselled to seek prompt medical attention if symptoms arise.
Case 4
A 27 years old male competitive discus thrower with training history of 8 years underwent pre - participation cardiovascular examination. He reported no cardiovascular symptoms and specifically denied chest pain, palpitations or syncope at rest or during exertion although he reported occasional headaches. Family history was negative for congenital or acquired cardiovascular diseases, diabetes, hypertension or sudden cardiac death.
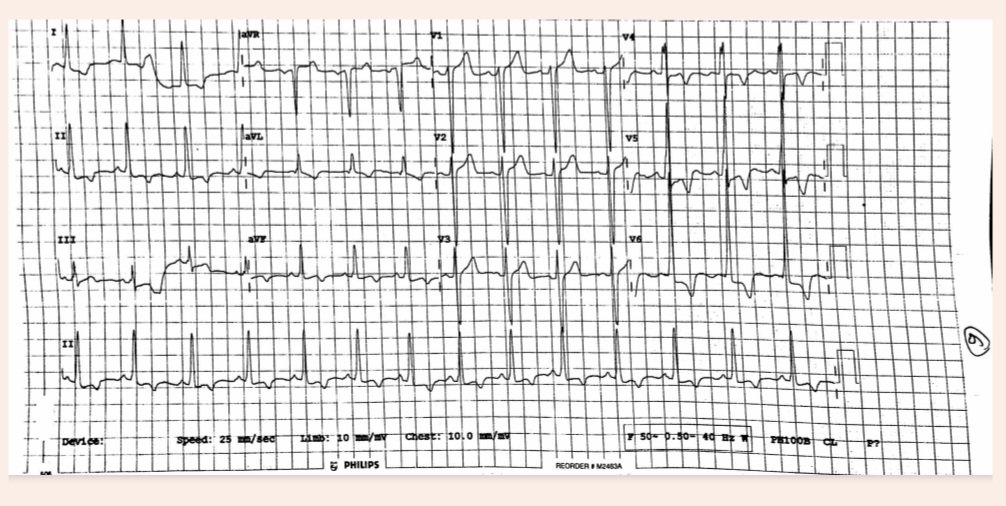
Resting blood pressure was recorded 140/90 mmHg, consistent with stage 1 hypertension with heart rate 90 bpm. 12 lead ECG demonstrated marked left ventricular hypertrophy according to sokolow - lyon voltage criteria, along with deep TWI in leads II, aVL, aVF, and V4 - V6 [Fig. 4].
Transthoracic echocardiography revealed end systolic posterior wall thickness of 2.0 cm and interventricular septal thickness of 2.5 cm. the left ventricular end diastolic diameter measured 5.1 cm and grade III diastolic dysfunction was present. These findings were consistent with HCM. No significant valvular abnormalities were noted.
Given these abnormal findings, the athlete was referred to cardiologist for further evaluation and management, counselled for prognosis and was provisionally deemed unfit for high intensity training and competitive participation.
Marked TWI in lateral leads are clinically significant, as they are recognised electrocardiographic markers commonly associated with HCM and ARVC. Such findings may occasionally be the sole manifestation of an inherited cardiac disorder, preceding any structural or functional abnormalities detectable by imaging. The four athletes described in the present report illustrate distinctly different outcomes despite comparable electrocardiographic abnormalities.
In the first case ECG change was physiological adaptation due to regular endurance training. In the second case, it was age related finding known as “juvenile pattern”. In the third case, repolarisation changes highlight diagnostic challenges faced by clinicians. Unnecessary disqualification from competition was not justified in the absence of genetic mutation analysis in these types of cases. At present, long term prognostic implications of such repolarisation patterns remain uncertain, and individual risk of sudden cardiac death cannot be reliably determined.
In first three cases, comprehensive diagnostic testing failed to identify structural or functional cardiac pathology, leading to medical clearance for competition. In contrast, fourth athlete demonstrated echocardiography finding characteristic of HCM. CMRI would have been useful in this instance to further define pattern and extent of myocardial involvement.
This case series aims to focus on various clinical outcomes of TWI in ECG of athletes. Hence it should not be used to draw any generalized conclusion. As this is a retrospective case series, no causality could be established, and a prospective surveillance study can be done in future to see the prevalence of TWI in athletic population.
A small proportion of athletes exhibit repolarisation abnormalities that may be indicative of inherited cardiomyopathies or ion channelopathies, the conditions recognised as potential mechanisms for SCD. The prevalence and distribution of TWI within this subgroup are influenced by age, sex, ethnicity and cumulative effects of long term, high intensity training. Emerging evidence indicates that anterior TWI is generally benign in adolescents and in individuals of African or Afro-Caribbean descent, whereas lateral TWIs should raise suspicion for underlying pathology.
The broad spectrum of clinical outcomes among athletes with TWI poses a challenge for treating sports medicine specialist. This case series aids better judgement and decision making for the clinicians.
Acknowledgements: All authors equally contributed to the conception and design of the study or acquisition of data, or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content and final approval of the version to be submitted.
Conflict of Interest: None.
Funding: Nil.
1. Physiological Society Symposium – the Athlete's Heart. Experimental Physiology. 2003; 88 (5). Available from: https://doi.org/10.1113/eph8802624
2. Sudden Death in a Young Soccer Player With Marked Electrocardiographic Repolarization Abnormalities. Clinical Journal of Sport Medicine. 2010; 20 (1). Available from: https://doi.org/10.1097/jsm.0b013e3181c9675a
3. Electrical and structural adaptations of the paediatric athlete’s heart: a systematic review with meta-analysis. British Journal of Sports Medicine. 2018; 52 (4). Available from: https://doi.org/10.1136/bjsports-2016-097052
4. The determinants of positivization of anterior T-wave inversion in children. The Journal of Sports Medicine and Physical Fitness. 2021; 61 (11). Available from: https://doi.org/10.23736/s0022-4707.20.11874-7
5. Electrocardiographic Changes Induced by Endurance Training and Pubertal Development in Male Children. The American Journal of Cardiology. 2017; 119 (5). Available from: https://doi.org/10.1016/j.amjcard.2016.11.017
6. Echocardiographic findings in 2261 peri-pubertal athletes with or without inverted T waves at electrocardiogram. Heart. 2015; 101 (3). Available from: https://doi.org/10.1136/heartjnl-2014-306110
7. The prevalence, distribution, and clinical outcomes of electrocardiographic repolarization patterns in male athletes of African/Afro-Caribbean origin. European Heart Journal. 2011; 32 (18). Available from: https://doi.org/10.1093/eurheartj/ehr140
8. Electrocardiographic changes occurring with alterations of posture from recumbent to standing positions. American Heart Journal. 1938; 15 (2). Available from: https://doi.org/10.1016/s0002-8703(38)90852-x
9. Exercise-Induced Normalization of Right Precordial Negative T Waves in Arrhythmogenic Right Ventricular Cardiomyopathy. The American Journal of Cardiology. 2013; 112 (3). Available from: https://doi.org/10.1016/j.amjcard.2013.03.048
10. Right Precordial T-Wave Inversion in Healthy Endurance Athletes Can Be Explained by Lateral Displacement of the Cardiac Apex. JACC: Clinical Electrophysiology. 2015; 1 (1-2). Available from: https://doi.org/10.1016/j.jacep.2015.03.007
Subscribe now for latest articles and news.